
Abstract
Abstract
Introduction
R
Case
The patient was a 25-year-old second gravida who had had an intrauterine fetal demise at 28 weeks in her first pregnancy, which was complicated by preeclampsia and intrauterine growth restriction. Following this, in the interpregnancy interval, she was diagnosed as having a partial septum. This diagnosis was made in a facility located in northern India and the condition was detected via a three-dimensional transabdominal scan (Fig. 1). She had been advised to undergo resection of this septum to improve the outcome of any subsequent pregnancies, and, subsequently, she underwent hysteroscopic resection of her septum under laparoscopic control. However, upon presentation to the current facility, the full intraoperative record of this surgery was not accessible; the only information she could provide was a brief discharge summary. In this summary, there were no mention of the technique used for the resection; the extent of resection; and if there were any intraoperative complications, such as heavy bleeding, perforation, or extensive resection of the septum. However the discharge note did mention that there were no intraoperative complications and that this patient's ovaries and Fallopian tubes were normal.

Three-dimensional ultrasonographic scan showing partial septum.
She conceived 6 months after this procedure and presented to the current facility at 30 weeks of gestation. Because she had moved to southern India, it was not possible for her to obtain her original operative record for review because the original hospital did not provide the record, although it was requested.
Her initial antenatal evaluation was normal. On a subsequent visit, at 34 weeks of gestation, a growth scan was performed. Fetal biometry and estimated weight corresponded to the period of gestation. However, on the next day, she presented to the current facility's emergency medical services with pain in her abdomen and was diagnosed as having “threatened preterm labor.” She was started on nifedipinetocolysis, and was also given dexamethasone to promote fetal lung maturity. Fetal evaluation was performed as she reported feeling decreased fetal movements. Her biophysical profile was normal, and the estimated fetal weight was 2700 g. However, no examination was made for ultrasonographic signs of impending rupture. She was admitted to the hospital for observation. Later that night, she developed bleeding from her vagina and continued to have pain in her abdomen. A clinical examination revealed no significant pallor and normal vital signs, a tense and tender uterus with an intact uterine contour, and absent fetal heart sounds. An urgent ultrasound examination was performed, which revealed a deceased fetus, with evidence of a retroplacental hematoma. Her cervical Bishop score was 4, and, therefore, intracervical dinaprostone gel was instilled for ripening. During this period, she experienced mild contractions and remained hemodynamically stable. A second dose of intracervical dinaprostone was instilled 6 hours after the first dose, as the cervical score was still unfavorable. Within 2 hours of this last dose, she complained of diffuse pain in her abdomen. She was diaphoretic and tachycardic. Her blood pressure was normal. An abdominal examination revealed diffuse tenderness and guarding all over her abdomen. The uterine contour was not detectable. Uterine rupture was suspected, and an immediate scan revealed that her uterus was contracted and retracted; it was imaged in the pelvis, with the fetus, amniotic sac, and placenta in toto located in her abdomen. No significant free fluid was present in her abdomen. Immediately, a laparotomy was done under general anesthesia. The fetus had been expelled encaul into the peritoneal cavity, with an intact amniotic sac and placenta attached to the sac. The retroplacental surface was covered with an adherent hematoma over 60% of its surface. There was a complete transfundal rupture of the uterus (Fig. 2). In view of her obstetric profile, we decided to conserve the uterus, and the rent was sutured in two layers. She received 4 units of packed cells transfusion intraoperatively. Postoperatively, she had 450 mL of blood through the suction drain over 2 days and received one more unit of packed blood cell transfusion.
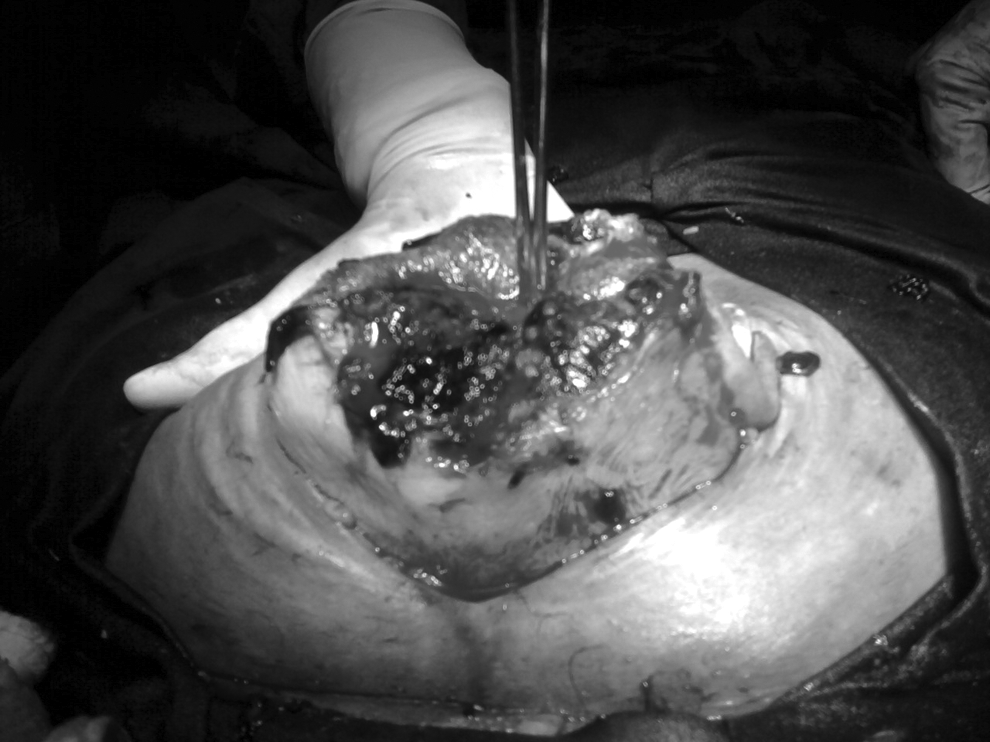
Intraoperative photograph showing complete fundal rupture.
Results
This patient recovered well and was discharged on the ninth postoperative day. She was advised to use contraception for at least 1 year and to make an appointment to be examined early in her next pregnancy.
Discussion
The septate or the subseptate uterus is one of the most common Müllerian anomalies and constitutes about one third of all uterine malformations. 1 In most cases, the septate uterus is an incidental finding during gynecologic or obstetric examinations. Commonly attributed symptoms and complications of septate uterus include subfertility, recurrent abortions, preterm births, and malpresentations. In the past, the uterine septum was addressed by open surgery (abdominal metroplasty). In the early years of operative hysteroscopy, the cumulative pregnancy rates and live birth rates of both endoscopic and open techniques were comparable. 2 With the advent of—and improvements in—endoscopy, hysteroscopic management of uterine septum has become the treatment of choice because of hysteroscopic management's relatively low intraoperative and short-term surgical morbidity when performed by a trained surgeon. The indications for hysteroscopic resection of the septum are evolving. As with any new surgical therapy, before accepting an indication for this kind of resection, the surgeon should weigh the potential short-term and long-term morbidities carefully against the expected benefit. Commonly agreed-upon indications are recurrent miscarriages and otherwise unexplained infertility. The efficacy of hysteroscopic septoplasty in terms of pregnancy rates and live birth rates was reviewed in a systematic review of 18 studies pooling 1501 patients: The overall pregnancy and live birth rate were 60% and 45%, respectively. 3 The association between the actual technique of septoplasty (i.e., scissors, laser, electrosurgery) and the success rate is not clear, although one case-control study favored using microscissors over a resectoscope. 4 Reported short-term surgical complications include uterine perforation, fluid overload, and cervical lacerations. The obstetric morbidity reported with hysteroscopic septal resection has been increased rates of malpresentation, more need for caesarean sections, low–birth-weight babies, 5 and antepartum hemorrhaging. 6 Catastrophic late morbidity associated with hysteroscopic septal resection has been quite rare; this can include uterine dehiscence or rupture in subsequent pregnancies. Many of the large serieshave either have not been reported or researchers have not looked at this complication.
The precise incidence of uterine rupture during pregnancy following operative hysteroscopy is not known and is probably too rare to be identified in studies with small outcomes. Much of the current knowledge of this particular complication is based on case reports. Uterine rupture has been reported following hysteroscopic adhesiolysis, hysteroscopic septal resection, and hysteroscopic metroplasty. All three major techniques for septal resection have been reportedly associated with uterine ruptures. 7 In the current case, the details of the exact method of the septal resection were not known. Ruptures have been spontaneous (pre labor),8–12 silent (incidentally discovered during caesareans), or symptomatic intrapartum events (manifested as severe abdominal pain with or without fetal distress).6,13,14 The current patient was symptomatic, but her clinical picture was complicated by an antecedent placental abruption.
Published literature on the rates of immediate, intermediate, and late complications15–17 of hysteroscopic septal resection seem to suggest that it is quite safe, which has encourage some researchers to widen the scope of indications. 18 In the absence of strict indications, this apparent “nonmaleficence” status might lead to unnecessary operative interventions that may have dire consequences. The current case is an example of such an intervention when the patient did not have subfertility or recurrent miscarriages. Several case reports have been published on the occurrence of uterine rupture in pregnancies following hysteroscopic septal resection. Sentilhes et al. 19 reviewed the literature on uterine rupture following operative hysteroscopy. Of the 14 cases identified in this review, 12 occurred following hysteroscopic septal resection. The researchers concluded that electrosurgery and uterine perforation increased the risk of subsequent rupture, but that these two procedures could not be considered as independent risk factors for rupture. In addition, the researchers could not find a strategy to predict or prevent uterine rupture during pregnancy. Apparently, laparoscopic control during hysteroscopic resection is not a guarantee against subsequent uterine rupture, as seen in the current case and in many reports.
Recently Valle and Epko reviewed the indications, outcomes, and complications of hysteroscopic metroplasty for septate uteri. 20 These researchers stated that pregnancy rates achieved with hysteroscopic metroplasty were superior to those achieved with open surgery. Furthermore, the researchers cited 18 case reports of uterine rupture during pregnancy or delivery following hysteroscopic surgery of the septum. These ruptures had occurred throughout the third trimester, mostly antepartum, and did not seem to bear any particular relationship with the time to pregnancy after hysteroscopy or the techniques used. More importantly, uterine perforation was not reported in many of these cases. Table 1 outlines seven major studies on hysteroscopic septoplasty outcomes. The current patient had conceived 6 months after hysteroscopy and had a rupture during induction of labor.
Fedele L, Arcaini L, Parazzini F, Vercellini P, Di Nola G. Reproductive prognosis after hysteroscopic metroplasty in 102 women: Life-table analysis. Fertil Steril 1993;59:768.
Pabuccu R, Gomel V. Reproductive outcome after hysteroscopic metroplasty in women with septate uterus and otherwise unexplained infertility. Fertil Steril 2004;81:1675.
Porcu G, Cravello L, D'Ercole C, et al. Hysteroscopic metroplasty for septate uterus and repetitive abortions: Reproductive outcome. Eur J Obstet Gynecol Reprod Biol 2000;88:81.
Roy KK, Singla S, Baruah J, Kumar S, Sharma JB, Karmakar D. Reproductive outcome following hysteroscopic septal resection in patients with infertility and recurrent abortions. Arch Gynecol Obstet 2011;283:273.
Saygili-Yilmaz E, Yildiz S, Erman-Akar M, Akyuz G, Yilmaz Z. Reproductive outcome of septate uterus after hysteroscopic metroplasty. Arch Gynecol Obstet 2003;268:289.
N/A, not available.
Conclusions
Regardless of the hysteroscopy technique used, intraoperative events, and laparoscopy control, it is imperative that clinicians establish attentive surveillance of pregnancies following hysteroscopic metroplasties, monitoring the integrity of the uterine fundus throughout the latter trimesters of pregnancy. This is vitally important if the intraoperative details are not known as the current authors have learned. Therefore, this case illustrates the need to remember “primum non nocere” even if the harm appears to be only potentially possible. The case also illustrates the need to formulate strict selection criteria for hysteroscopic septal resection—such as defining the number of pregnancy losses before they are attributed to the septum; the etiology of the pregnancy loss (or the apparent lack of a cause); and evaluation of infertility for other potential causes—before attempting surgical treatment of the septum.
Disclosure Statement
No competing financial conflicts exist.