
Abstract
Abstract
Introduction
A
Although peritoneal tuberculosis is uncommon, an increase of disease incidence has been noted in the Western world, because of the the high volume of world travel, of immigration from countries with a high prevalence of tuberculosis, and of patients with autoimmunodeficiency syndrome.2–5 Given that the clinical manifestations of PT may resemble those of ovarian carcinoma, with ascites and abdominopelvic masses, many surgeons in Western countries who are not familiar with PT could diagnose PT erroneously as advanced ovarian cancer, by considering the clinical presentation and even, sometimes, by considering the intraoperative findings for this disease. This serious diagnostic error might have dramatic therapeutic consequences, if radical surgery is performed during the initial surgery without histologic documentation.
This article presents the case of a pregnant woman with abdominopelvic tuberculosis. The diagnostic and therapeutic problems associated with such a case are discussed and a brief review of the relevant literature is provided.
Case
A 38-year-old, gravida 5, para 3, Chinese woman was referred to the current facility department at 28 weeks of gestation for ascites, a 2-month history of intermittent upper-abdominal pain, increased coughing, and shortness of breath for 3 days. She had no associated history of any menstrual disturbances. Two months prior to presentation, she had complained of localized abdominal pain, located mainly under both costal margins, which increased in intensity after eating; however, these symptoms were left untreated. One month prior to her current presentation, she went to a local hospital complaining of anorexia, a cough with yellow phlegm, and shortness of breath. She had made good progress after i.v. antibiotics (product unknown) were administered to her for 3 days, but she still had some coughing and sputum, anorexia, and general fatigue.
A physical examination of this patient showed a blood pressure of 120/70 mm Hg, a cachectic appearance, malnourishment, and a dull appearance. Auscultation revealed a diminished right lower lung and a wheezing breath from her left side. Her heart rate (HR) was 102 beats per minute (bpm) with a regular pulse. No pathologic heart murmur was found. Her abdomen was mildly distended with obvious upper-abdominal tenderness. Abdominal auscultation revealed a weakened intestinal sound. No rebound tenderness or hepatosplenomegaly was noted. A shifting dullness test was positive. On palpation, no pathologic abdominal masses were found. The fetal HR was heard in the right-lower quadrant at 156 bpm with a regular pulse. Upon obstetric examination, the patient was noted to have a fundal height of 28 cm and an abdominal circumference of 92 cm. The fetus, with a high-floating head, was located in her lower abdomen. Fetal movement was palpable through the maternal abdomen. Gynecologic examination showed a normal appearance of her vulva. No vaginal obstruction was noted except for a large quantity of “curdy” leucorrhea inside the vagina. Mild cervical erosion was present, with a purple-blue color. A laboratory blood test showed a total protein level of 51 g/L and an albumin level of 15 g/L. A tuberculin skin test was positive. Color Doppler ultrasound showed a late-stage pregnancy with a single viable fetus at a cephalic presentation. The fetus presented with signs of tachycardia. The ultrasound scan also showed the presence of intra-abdominal fluid, mainly in her lower abdomen. An electrocardigram showed sinus tachycardia in the patient and nonspecific ST–T changes.
This patient was admitted with presumed diagnoses of (1) ascites and shortness of breath (unknown reason); (2) pregnancy with 28+3 weeks, gravida 5, para 3; (3) infection of the upper respiratory tract; (4) vaginitis; and (5) hypoproteinemia. Initially, she was treated conservatively (i.v. administration of fluids and antibiotics), but this treatment failed to improve her clinical condition.
Six days later, the patient underwent an abdominohysterotomy delivery. At surgery, the patient's peritoneal membrane was found to be markedly thickened, with no obvious miliary nodules. Approximately 2.5 L of yellowish, clear ascitic fluid was removed from her abdomen. Grossly, the patient's uterus was distended, as expected at this stage of pregnancy, with a congested surface and inflammatory thickening. Her bilateral Fallopian tubes were irregularly dilated up to 6.5 cm in diameter at the ampulary region. Fimbriae of the oviducts were occupied with caseation granuloma, which did not have a “beaded” appearance and which discharged pus when squeezed. No ovarian mass was found, except for inflammatory exudation. The greater omentum became thickened and adhered with the peritoneum to form a single-layer structure. The gut inside the abdomen became adhered and enlarged with the formation of encapsulated effusion. No pathologic mass or intestine blockage was noted, although miliary nodules were found surrounding the transverse colon and stomach. The clinical intraoperative diagnoses were amended to (1) ascites, abdominopelvic tuberculosis; (2) pregnancy with 29+3 weeks; (3) empyema in the Fallopian tubes; and (4) pelvic infection.
Considering the potential for postpartum hemorrhage and severe disseminated pelvic infection, with her agreement, the patient received extended surgery including total abdominal hysterectomy, bilateral salpingectomy, and omentectomy. An excision biopsy was taken, and the pathologic report confirmed the presence of chronic granulomas, with caseous necrosis and multinucleated giant cells (Figs. 1 and 2).

Photomicrograph showing granulomas with caseous necrosis in the intraoperational biopsy specimen. (Hematoxylin & Eosin stain, lower magnification of 10×)
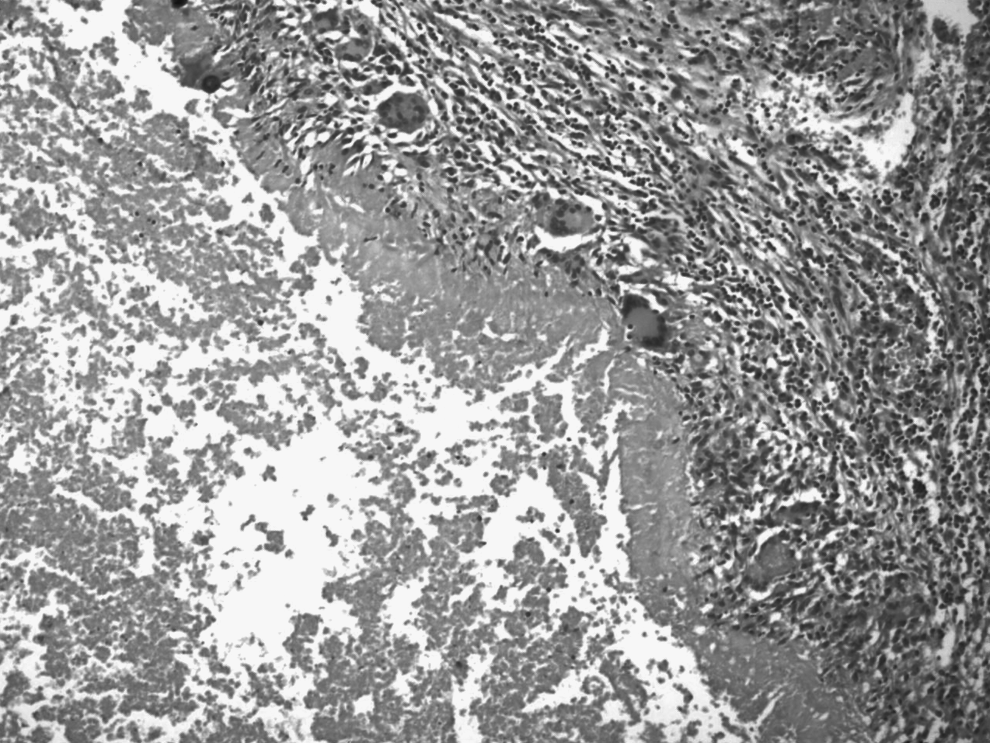
Photomicrograph showing granulomatous inflammation, multinucleated giant cells (Langhan's giant cells), and caseous necrosis. (Hematoxylin & Eosin stain, high magnification of 20×)
Results
The patient recovered well after postoperative treatment. She was discharged from the hospital on day 15 postoperatively, but continued to receive an antituberculous chemotherapy regimen with rifampicin (R), isoniazid (H), pyrazinamide (Z) for 2 months, followed by R&H for an additional 4 months.
At follow-up, the patient had completely recovered and returned to normal life.
Discussion
In pregnancy, the incidence of tuberculosis is low. Although pregnancy with pulmonary tuberculosis has accounted for 2%∼7% of pregnant women,5,6 abdominopelvic tuberculosis in pregnancy is uncommon and rarely reported. This may be, in part, because infertility often occurs when tuberculosis involves the genitals and/or peritoneum. In the current case, the patient was admitted and given conservative treatment with i.v administration of fluids and antibiotics. When the initial medical treatment failed to improve her clinical condition, the patient underwent abdominal hysterotomy delivery and then had extended surgery to prevent potential postpartum hemorrhage and disseminated pelvic infection. After postoperative treatment with antituberculous chemotherapy, the patient improved significantly and was discharged from the hospital.
Based on the experience of this case, abdominopelvic tuberculosis should be suspected when ascites is present in pregnancy, which may deceive a gynecologist to misdiagnose the patient as having an ovarian malignancy. Early diagnosis and treatment of PT in pregnancy are important for minimizing adverse obstetrical and neonatal effects.7,8
Abdominopelvic tuberculosis occurs mostly in young people, and generally is a secondary infection derived mainly from pulmonary tuberculosis or PT. Persistent fever, abdominal pain, diarrhea, constipation, weight loss, anorexia, and discomfort are common complaints. 9 The clinical manifestations of female pelvic tuberculosis progress insidiously and usually show no specificity. Symptoms mainly include infertility, menstrual abnormalities, pain and a bearing-down sensation in the lower abdomen, which are all present in other common gynecologic disorders, such as chronic pelvic inflammatory disease, ovarian cancer, and endometriosis. Thus, clinical discrimination between PT and these disorders may be extremely difficult. 10 It has been reported that the misdiagnosis rate of pelvic tuberculosis may be as high as 65.3%–72%. 11
Lack of awareness of abdominopelvic tuberculosis by a gynecologist may lead to performance of unnecessary extended surgery. Thus, the preoperative and even intraoperative differential diagnosis of PT versus ovarian carcinoma is often difficult and problematic. The following tests are needed to make an accurate diagnosis: (1) ultrasound scanning of the abdominopelvic cavity; (2) the Mantoux test; (3) CA-125 level; (4) computed tomography scanning; and (5) biochemical assessment of total protein of ascites and lactate dehydrogenase level. 12
It has been reported that infertility is one of the most common signs of abdominopelvic tuberculosis. 13 Once abdominopelvic tuberculosis in pregnancy is suspected, the following laboratory tests for aspirates and biopsy specimens are needed to finally confirm the diagnosis: (1) presence of acid-fast bacilli (Ziehl– Nielson staining positive); (2) apositive culture for Mycobacterium tuberculosis; and (3) polymerase chain reaction–positive for M. tuberculosis complex.14,15
Conclusions
If no carcinoma is detected and the diagnosis of abdominopelvic tuberculosis is confirmed, conservative treatment of antituberculosis chemotherapy could be initiated. This can not only save the life of the fetus, but can also protect the mother from unnecessary extensive surgery and major irreversible amputation, such as total hysterectomy.
Footnotes
Acknowledgments
The authors thank Ryan M. Porter, PhD, Beth Israel Deaconess Medical Center, Boston, MA, for his generous review and editing of this article.
Disclosure Statement
No potential conflicts of interest exist.