
Abstract
Abstract
Introduction
U
Case
A 55-year-old multiparous postmenopausal woman presented with a history of abdominal distension, which she had noticed for several years. Prior to presenting to Fernandez Hospital, she had not sought medical attention for this. She had also noticed loss of weight over 3 years, but her appetite was normal. There was no history of abdominal pain, vaginal bleeding, or bowel and bladder symptoms. Both her children had been delivered by Cesarean section. She did not have any coexisting medical disorders. There was no family history of malignancies. She appeared cachectic, and physical examination revealed massive distension of the abdomen, corresponding to term gestation, caused by a large abdominopelvic mass extending up to the xiphisternum. The overlying skin was stretched over the mass. The patient did not consent to a vaginal examination, hence a Papanicolaou smear could not be performed. The provisional clinical diagnosis was ovarian malignancy. Tumor markers and baseline blood investigations were normal, with borderline serum creatinine of 1.2 mg/dL. Computed tomography scan revealed a huge heterogeneous space-occupying lesion measuring 29×27×30 cm, filling the abdomen, with compression of the right mid ureter causing mild hydronephrosis. Calcification, necrosis, and fat were seen in the mass, and the uterus and ovaries could not be seen separately. The impression was that of a degenerated calcified giant leiomyoma.
Exploratory laparotomy was performed through a midline incision. The uterus was uniformly enlarged by a huge vascular mass measuring ∼30×30 cm, and the uterus was twisted by 90 degrees around its long axis at the level of the cervix (Fig. 1). The Fallopian tubes and round ligaments were stretched over the tumor. The cervix and ovaries were atrophic. The rest of the abdomen was normal. Total hysterectomy and bilateral salpingo-oophorectomy were performed. During the procedure, the urinary bladder was inadvertently injured, as it was adherent to the previous Cesarean scars. Under cystoscopic guidance, bilateral ureteric stents were placed, and the bladder defect was repaired. Abdominoplasty was performed after excising redundant skin and subcutaneous tissues. Three units of blood were transfused in the perioperative period, as there was massive hemorrhage of >3.5 L during the surgery because of the abundant vascularity of the tumor. The patient was given broad-spectrum antibiotics and heparin for thromboprophylaxis.
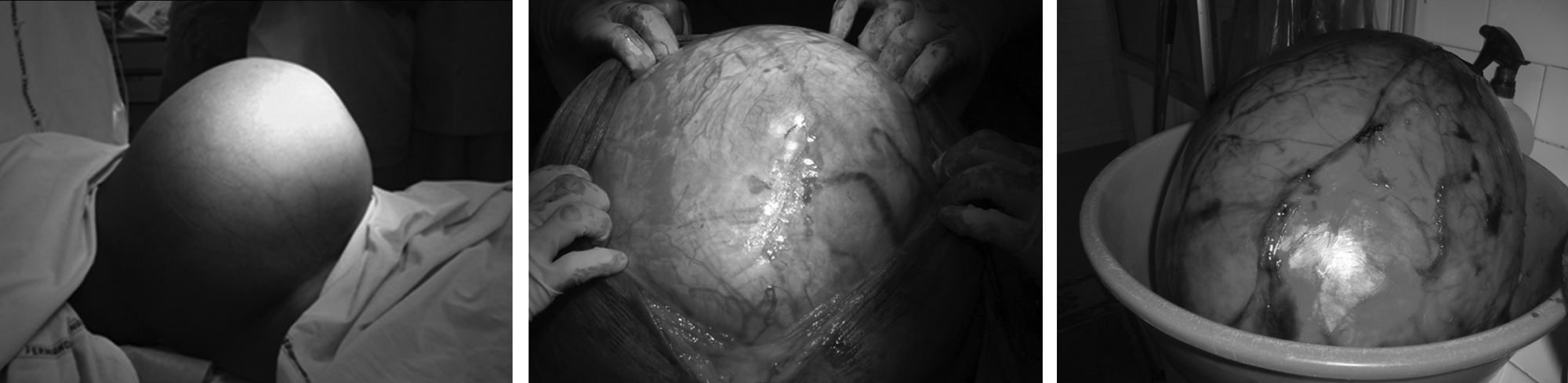
Three views of a giant leiomyoma of the uterus.
The uterus weighed 15 kg and measured 30×27×21 cm. The external surface appeared congested. On cut section, endometrial cavity and myometrium could not be identified separately, and the fibroid showed a nodular appearance. Sections from the fibroid showed smooth muscle bundles in interlacing fascicles, with no significant pleomorphism, mitosis, or necrosis. The impression was that of a giant leiomyoma with degeneration. Ovaries and tubes were unremarkable. The cervix showed normal endocervical lining with subepithelial inflammation.
Results
The patient had an uneventful recovery, and was discharged 1 week after the surgery. The urinary catheter was removed on the 10th postoperative day. Two weeks after the surgery, the patient was treated with ciprofloxacin for urosepsis with Escherichia coli. Ureteric stents were removed 4 weeks after surgery. At a follow up visit 6 weeks later, she appeared to have recovered well, and is in good health 2 years after the surgery.
Discussion
Torsion of the uterus is defined as rotation of >45 degrees around the longitudinal axis of the uterus, and can range up to 900 degrees. 1 It is more common in animals, and in humans it is most often seen in pregnant women. Uterine torsion is observed in all age groups during the reproductive period, in all parity groups, and at all stages of pregnancy. Dextrorotation occurs in two thirds of the cases.
Uterine torsion is normally prevented by round ligaments, broad ligaments, and the uterosacral ligaments.2,3 The causal factors are not well-understood, but structural abnormalities of the uterus or adnexae are demonstrated in 20% of the cases. Abnormal fetal presentation and uterine fibroids are seen in 23% and 21% of patients, respectively. 4 Most of the cases caused by congenital uterine abnormalities are seen in women with bicornuate uteri. Poor isthmic healing after lower segment Cesarean delivery may result in suboptimal restoration of normal cervical length, resulting in an elongated cervix with structural weakness, and angulation in the isthmic region, which may predispose to torsion. 5 Pelvic adhesions 6 and peristaltic movements of the sigmoid colon 2 may also cause uterine torsion.
A myomatous uterus is the most common abnormality seen in nongravid uterine torsion. 6 Torsion of a pedunculated subserous fibroid is well-known, but total uterine torsion caused by a fibroid is rare. The increased size of the uterus caused by the intramural leiomyoma may predispose to uterine torsion. 7 A large heavy fibroid may rotate because of its weight, and exert traction on the uterus. The point of torsion of the uterus usually occurs at the level of the uterine isthmus. 3 Myotonic dystrophy was also implicated as a causative factor in a patient who presented with torsion of a myomatous uterus. 8 Unusual cases of uterine torsion in postmenopausal women with leiomyomata resembling malignant ovarian tumor 9 and others associated with necrosis of the uterus and adnexae10,11 have been described. Dutra et al. reported the case of a 10-year-old premenarchal girl with a large dermoid cyst occupying the entire abdomen, which was twisted 360 degrees in conjunction with the uterine corpus with hemorrhagic infarction. 12
The presentation is often nonspecific. Clinical manifestation varies from acute to chronic, and some patients may be asymptomatic. Symptomatic torsion occurs when the degree of twisting is sufficient to interfere with arterial or venous circulation. Abdominal pain is the most common symptom, and it can present as an acute abdomen. 13 Some women may present with gastrointestinal or urinary symptoms. Specific clinical signs can include vaginal bleeding, uterine tenderness, a twisted vaginal canal, urethral displacement, and posterosuperior displacement of the cervix. 14 The differential diagnoses include appendicitis, fibroid degeneration, torsion of a pelvic tumor, abdominal pregnancy, and placental abruption. 7 Reported radiologic features of uterine torsion are gas in the uterine cavity on plain radiographs and CT scan. Torsion of a myomatous uterus may be suspected if fibroids noted on previous ultrasound scans are seen to have changed position. The whorled appearance of the uterine cervix represents twisting of the cervix. The wall of the upper vagina changes from the normal H configuration to an X-shaped configuration. 15
Conclusions
The clinical challenge of uterine torsion lies in its elusive diagnosis, and definitive diagnosis is often made intraoperatively. At exploration, any contributing pathology of the uterus or adnexa is best removed. Hysterectomy with removal of both adnexae may be considered in postmenopausal women, as in this case.
Footnotes
Disclosure Statement
No competing financial conflicts exist.