
Abstract
Abstract
Introduction
P
Case
A 33-year-old Chinese nulliparous woman presented to the reproductive endocrinologist's office in Akron, Ohio in August 2011 with complaint of primary infertility of 1 year's duration. She and her husband had been born in China. She had moved to Canada in 2000 and relocated to Cleveland, Ohio in 2009. During her appointment, she complained of dysmenorrhea and pelvic pain. Her medical history included paratyphoid, pinworms, and childhood mumps. Menarche occurred at age 14 with regular 28–30 day cycles. She had one sexual partner over her lifetime. She had no history of sexual transmitted infections, human immunodeficiency virus, or hepatitis. She denied having current medications, surgical history, or drug allergies. She denied any significant family history of disease. She denied tobacco or drug use, but admitted to occasional alcohol use. Her husband was a 33-year-old Chinese male without significant medical history, who resided in a different state, and visited the patient on the weekends. He was treated for paratyphoid fever as a child. He had no history of sexual transmitted infections. He had no testicular masses. He did not provide a semen analysis and denied having fathered any children.
The patient was a 131 pound slender Chinese female. On pelvic examination, a small, pedunculated exocervical polyp was removed, and found to be benign, per pathology examination. Blood tests completed included complete blood count (CBC), vitamin D level, varicella, rubella, cystic fibrosis, spinal muscular atrophy (SMA), gonadotropins, prolactin, thyroid studies, progesterone, testosterone, dehydroepiandrosterone sulfate (DHEA-S), sperm antibodies, estradiol (E2), human chorionic gonadrotropin (hCG), sex hormone binding globulin (SHBG), androstenedione, and sexually transmitted disease testing. All laboratory results were normal except for a low Vitamin D level, for which supplementation was implemented. A transvaginal ultrasound showed a subserosal small fibroid measuring 18 mm. The patient was scheduled for hysterosalpingogram (HSG) for further evaluation.
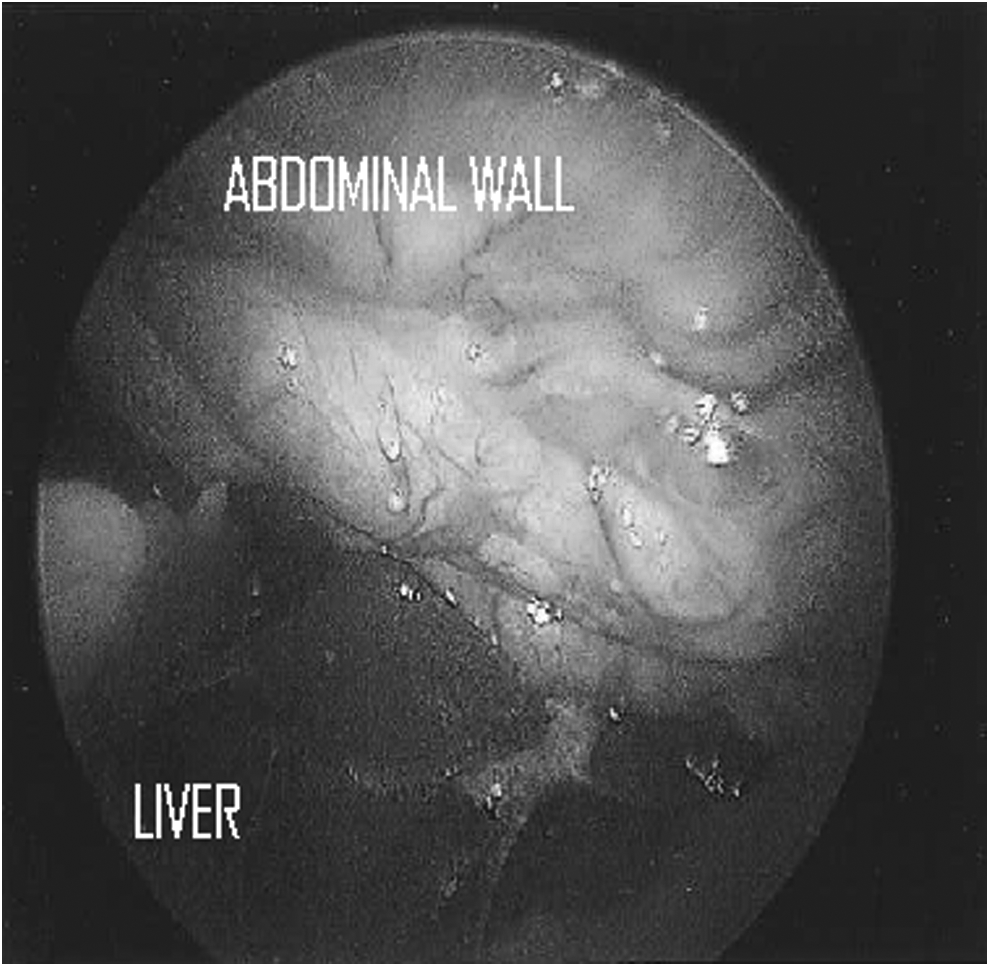
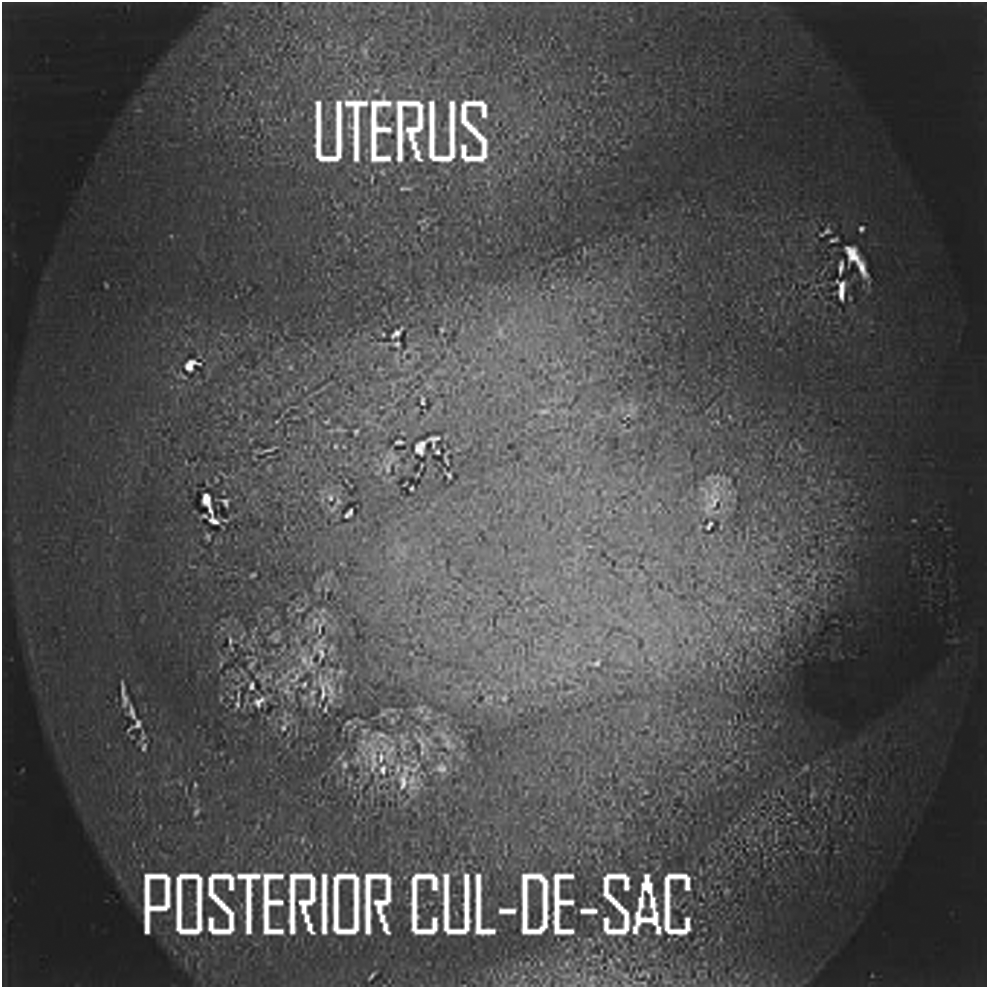
Hysterosalpingogram revealed tubal occlusion at the early ampullary portion of the left Fallopian tube. The right Fallopian tube filled distally, and appeared to be obstructed by a hydrosalpinx (Fig. 1). A decision was made to proceed with laparoscopy. Laparoscopy revealed multiple implants of small nodules disseminated throughout the entire peritoneal cavity extending to the anterior peritoneum over the bladder, uterine serosa, bilateral Fallopian tubes and ovaries, cul-de-sac, cecum, small bowel, appendix, and liver (Fig. 2). The surgeon described them as small, white, hardened, and superficial lesions. There was evidence of perihepatic adhesions indicating Fitz-Hugh–Curtis syndrome (Fig. 3). A 1.5 cm×1.5 cm hardened nodule was noted in the distal ampulla of the left Fallopian tube. There was a left ovarian follicular cyst. Both ovaries were free and mobile. A solitary nodule between the bladder and uterine serosa was removed and sent to pathology for analysis. The gynecologic oncologist was consulted intraoperatively for further expertise, and both surgeons suspected pelvic tuberculosis.
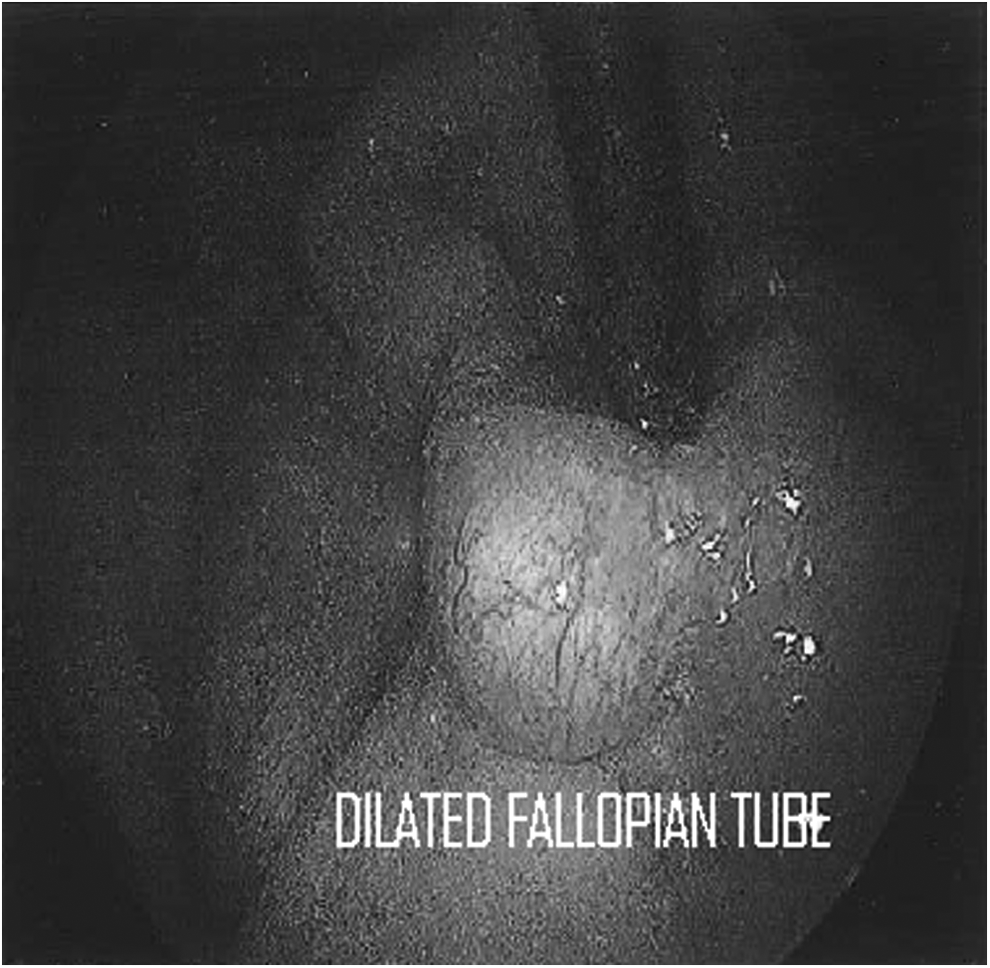
Dilated Fallopian tube.
Tubercles of the posterior cul-de-sac in a rosette pattern.
Tubercles infiltrating the abdominal cavity.
Postoperatively, the patient acknowledged that a purified protein derivative (PPD) was positive 2 months prior, which had been administered for immigration purposes. The chest radiograph at that time had been negative. She had declined treatment for latent tuberculosis because of her wish to avoid medications that were not recommended during pregnancy. She had received the bacillus Calmette–Guerin (BCG) vaccine while living in China. She was referred to an infectious disease specialist, who reported that the initial biopsies were consistent with a hyalinized fibrous nodule. They were negative for acid fast bacilli, fungus, and bacteria. Quantiferon, which is a diagnostic blood test for latent tuberculosis infection, was positive. The specialist requested additional biopsies of the left Fallopian mass because the disease primarily originates from the Fallopian tubes. The patient underwent laparoscopy by the gynecologic oncologist for further collection of tissue samples. Multiple peritoneal biopsies were collected for histologic examination and staining. The surgeon noted multiple small pearly white nodules involving the bowel serosa, peritoneum, and cul-de-sac. There were also two large nodules involving the left Fallopian tube. A left salpingectomy was performed, and the Fallopian tube was sent for analysis. The peritoneal biopsies and nodules revealed granulomatous inflammation with fibrosis. The left Fallopian tube exhibited transmural necrotizing granulomatous inflammation consistent with tuberculous salpingitis. Acid fast stain was negative. The Fallopian tube also showed epithelioid histiocytes forming granulomas, and Langhans type giant cells with necrotic debris. Small scattered areas of calcification were noted. Polymerase chain reaction (PCR) was not done, because of the specialist's recommendation to treat regardless of positivity. A follow-up computed tomography (CT) of the chest was ordered, which revealed several noncalcified right lung nodules consistent with prior granulomatous disease. The infectious disease specialist initiated rifampin, isoniazid, pyrazinamide, and ethambutol (RHZE) per World Health Organization recommendations. The patient was advised against pregnancy for an additional 1 year after completion of medication. The patient began treatment reluctantly.
Results
The patient was treated by the infectious-disease specialist and had not returned to the infectious-disease specialist prior to this writing.
Discussion
The Centers for Disease Control and Prevention (CDC) report that one third of the world's population is infected with tuberculosis. 3 Although cases of tuberculosis are declining in the United States, the physician must always be suspicious of disease in patients with risk factors. Half of the reported cases in the United States are in immigrant populations who have resided in the country for <5 years. 4 Populations most at risk include HIV-positive individuals, intravenous (IV) drug users, alcoholics, urban poor, homeless, prison inmates, and migrant farm workers. 4 If a patient possesses risk factors, a PPD should be administered. Unfortunately, as in the case of this patient, the diagnosis was unsuspected prior to surgery, and the patient did not discuss her positive PPD test with the infertility specialist.
Pelvic tuberculosis is diagnosed in 10%–20% of patients with primary pulmonary disease. 2 Pelvic disease occurs by lymphatic, hematogenous, or local spread from abdominal organs to the Fallopian tube. 2 The Fallopian tubes are involved in 90% of cases. 1 Direct extension from the Fallopian tubes then occurs to the endometrium (50%), ovaries (30%), cervix (10%), and vagina (1%). 4 The gold standard for the diagnosis of genital tuberculosis is isolation of the Mycobacterium tuberculosis in the genital tract. 5 Bacteriologic examination is often negative because 100,000 mycobacteria per milliliter must be present for a positive diagnosis. 6 Falk et al. found that only 29% of patients had a positive diagnosis based on isolation of the bacteria. 7 For patients suspected of disease, endometrial biopsy should be pursued. Parikh et al. demonstrated positive histopathologic cultures in 50% of patients. 8 Menstrual blood should also be collected, as cultures are reported to be positive in 69.9% of patients. 9 A negative culture does not rule out disease, because Fallopian tube disease may be present in the absence of endometrial disease in 30%–40% of cases. 2 Surgical procedures may be required to confirm diagnosis and obtain specimens for pathology, although the risk for perforation and organ damage is high. 10 Specimens collected during laparoscopy should incorporate PCR testing because of the high sensitivity of testing. 11 Biopsies should include samples from either end of the Fallopian tube. 11 HSG and laparoscopy should be avoided during active disease because of the risk of a reactivation of disease. 12 If tuberculosis is suspected, patients should be promptly referred to an infectious disease specialist for proper treatment until biopsies prove otherwise.
HSG is commonly utilized first in the evaluation of infertility, and is an important diagnostic tool for pelvic tuberculosis. Klein et al. established diagnostic criteria for the disease: 1) calcified lymph nodules or smaller irregular calcifications in the adnexal area, 2) obstruction of the Fallopian tube between portions of isthmus and ampulla, 3) multiple constrictions along the Fallopian tube, 4) endometrial adhesions and/or deformity of the endometrial cavity, and 5) a uterine cavity that may appear shrunken or T-shaped. 12 Venous and lymphatic intravasation of contrast may be present. 5 Chavhan et al. reported that 81% of patients had tubal occlusion on HSG. Occlusion with terminal hydrosalpinx was seen in 32%, and a beaded appearance was seen in 16% of patients. 13 HSG is a sensitive screening test because patients with disease will not exhibit normal anatomy. 5
In the United States, pelvic tuberculosis is not common and, therefore, not likely to exist in the differential diagnoses. The question of tuberculosis will likely be raised at the time of routine laparoscopy. The surgeon must be cognizant of the disease appearance in order to obtain proper biopsies and refer the patient to proper specialists. In addition, laparoscopic surgery must be carefully performed because of the presence of dense adhesions. Gupta et al. reported omental adhesions in 45% of patients and bowel adhesions in 37.5% of patients. 14 Sharma et al. observed Fitz-Hugh–Curtis syndrome 16.6% of Indian women with diagnosed genital tuberculosis undergoing laparoscopy for infertility. 15 Because of the risk of bleeding complications, lysis of adhesions is not recommended. 15 The Fallopian tubes appear distorted and tortuous, and may appear enlarged and dilated, similar to a “tobacco pouch.” 10 Tubo-ovarian masses such as hydrosalpinx or pyosalpinx may be present. 15 Chromotubation should not be attempted, because of the risk of flare-up. 15 Tubercles may cover all peritoneal surfaces of the abdomen and pelvis. 2 Granulomas, plaques, exudates, and pelvic congestion can be seen. 15 Pelvic ascites may be present and fluid should be sent for analysis. 2
Conclusions
The presence of pelvic tuberculosis has devastating effects on future reproduction, and patients should be regarded as infertile. 6 In a literature review by Schafer in 1976, after treatment for pelvic tuberculosis, 2.2% of patients had full term pregnancies, 1.8% had ectopic pregnancies, and 0.9% had abortions. 1 In vitro fertilization (IVF) has shown to be successful in select women without tubercular endometritis and uterine synechiae. 16 Successful IVF therapy has been reported among patients with a normal uterine cavity, negative cultures, and functional ovaries. 17 Physicians must be suspicious of pelvic tuberculosis in patients with risk factors who present with infertility. General gynecologists and infertility specialists should not hesitate to refer these patients to infectious disease specialists because of the devastating impact of tuberculosis.
Disclosure Statement
No competing financial interests exist.