
Abstract
Abstract
Introduction
I
Case
In 2001, a 52-year-old female underwent an abdominal radical hysterectomy to address a cervical adenocarcinoma, FIGO [International Federation of Gynecology and Obstetrics] stage Ib, and was given adjuvant chemoradiation because of pelvic lymph node metastases. Her good condition was noted on a regular 7-year follow-up, until an abdominal mass had developed, since 2008, that caused tenderness and intermittent constipation and urinary symptoms, such as urgency and frequency. As the mass grew larger, this patient's symptoms also worsened gradually. An incisional hernia was diagnosed during this regular follow-up in 2008.
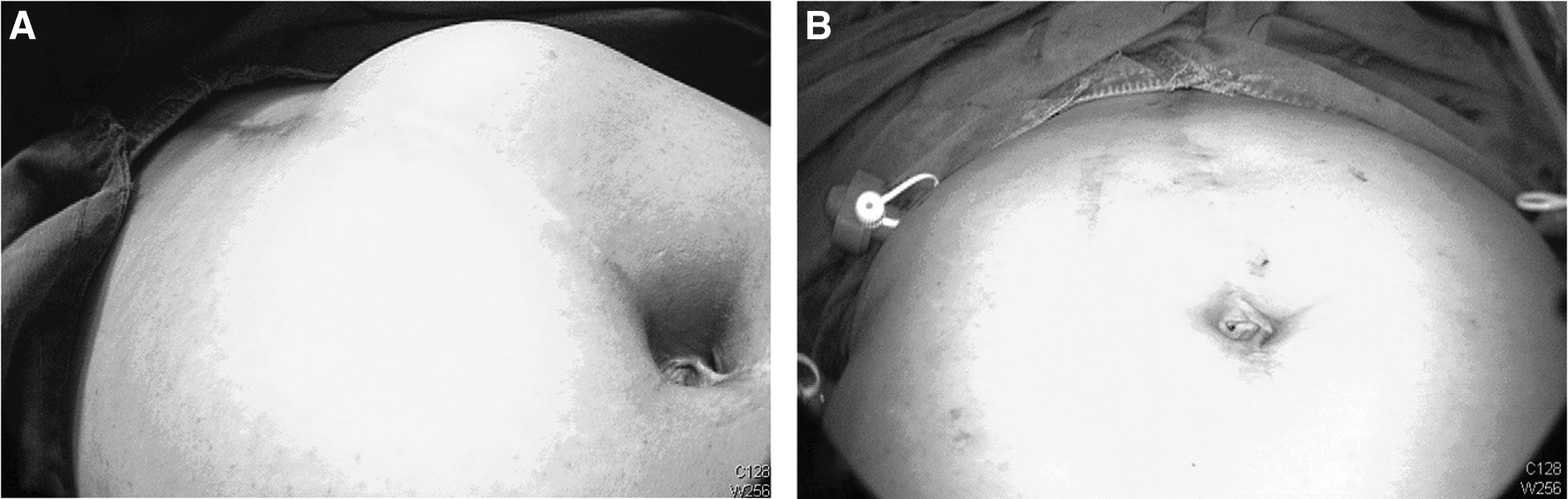
The patient had no history of diabetes mellitus, hypertension, or other systemic diseases. She denied any substance abuse, such as tobacco, alcohol, or betel nuts. No abdominal major surgery other than the radical hysterectomy for cervical adenocarcinoma was recorded. Her body mass index was 24.5 on this current admission. A physical examination showed a bulging, nonreducible mass measuring 8×8×4 cm (Fig. 1A; Fig 1B shows repair of the problem via herniorrhapy) over the previous midline incision wound scar. An abdominal computed tomography scan revealed a horizontal defect at the midline of the abdominal wall measuring 3.75cm (Fig. 2). Surgical intervention with a minimally invasive procedure was chosen.
(
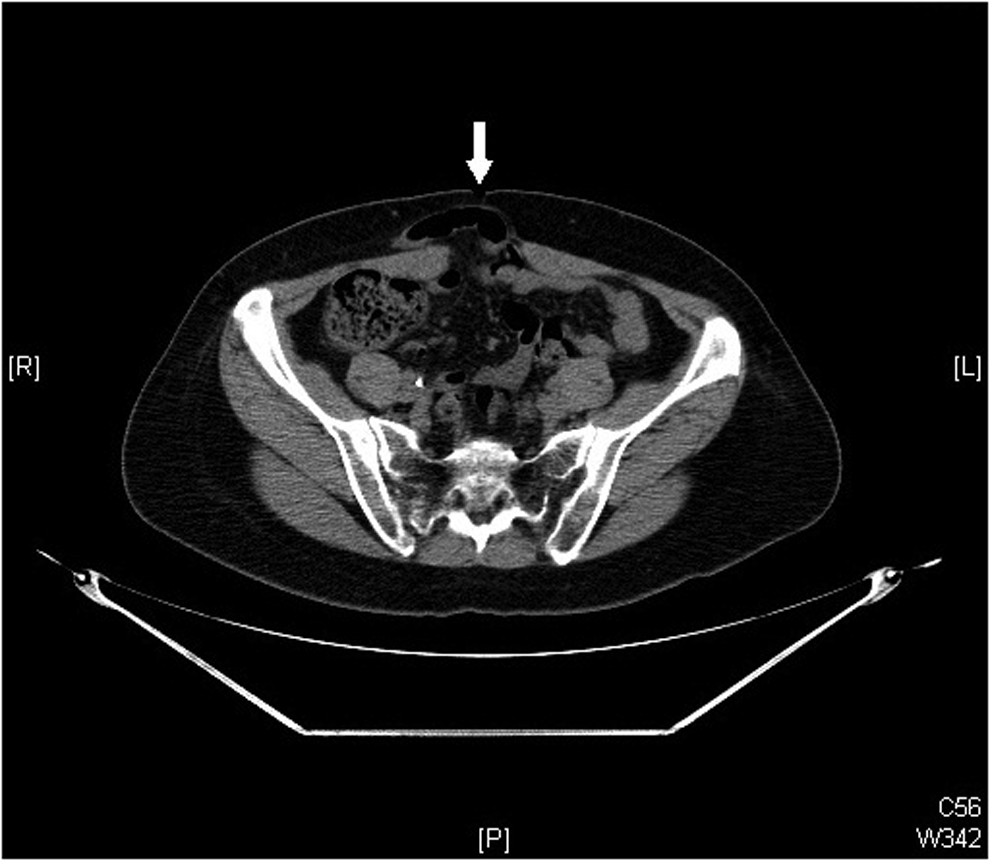
An abdominal computed tomography scan revealed a horizontal midline defect with bowel protrusion (white arrow) measuring 3.75 cm.
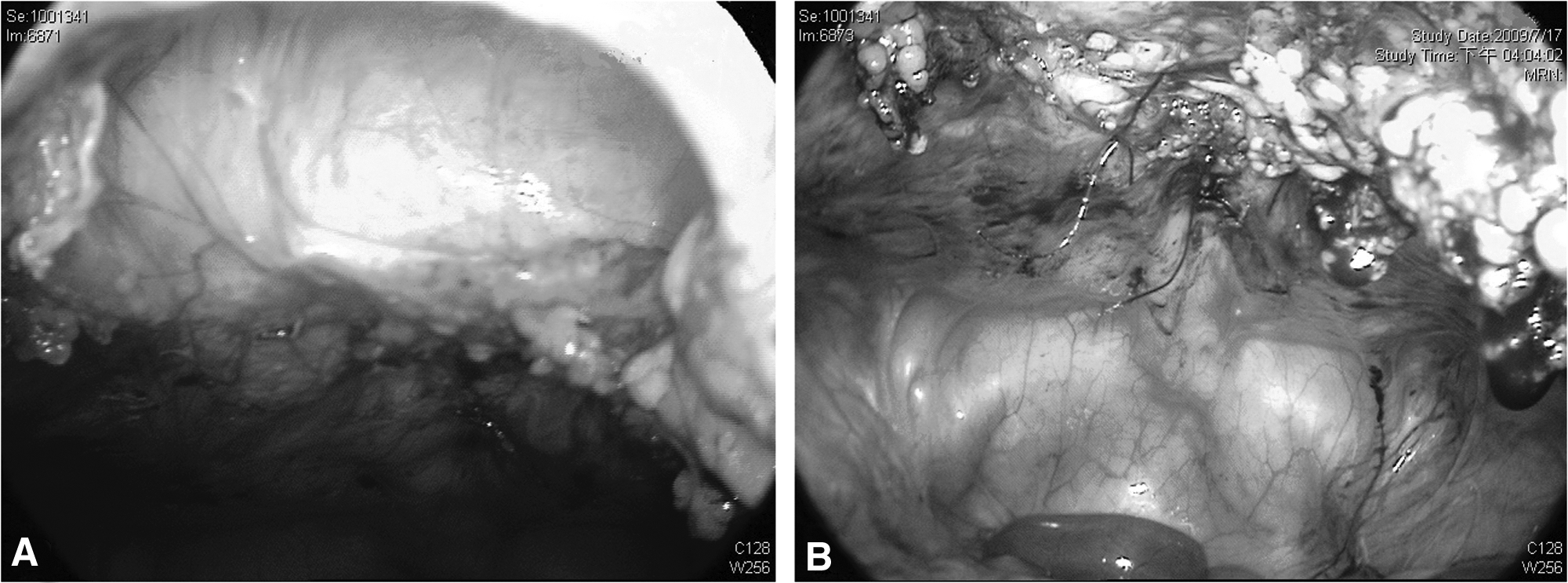
Laparoscopic surgery was performed using a Lee-Huang point, with a first and major trocar and three accessory trocars over the lower abdomen. The hernia sac was 3 cm below the umbilicus, with a defect measuring 8×4 cm (Fig. 3A). There was an extensive adhesion over the previous surgical site, thus, extensive enterolysis and a polypropylene mesh (also known as prolene mesh), with 3 cm overlapping peripherally to the lesion, was inserted into the hernia sac. Transfascial suture fixation was done at 4 directions. The opening sac was closed with an interrupted extracorporeal suture using 1-0 prolene (Figs. 1B and 3B). There was no subsequent air pouch observed after the entire procedure was completed. The patient had a good recovery and was discharged 3 days after the operation.
Results
On the tenth postoperative day, she had mild cutaneous ecchymosis without tenderness. Expectant management was applied and spontaneous improvement was noted with no complaints. As of 4 years, the patient had a desirable recovery without clinical recurrence.
Discussion
Incisional hernia is one of the most common complications following a laparotomy. The incidence of incisional hernia after major gynecologic oncology operations, such as extended abdominal hysterectomy to address cervical or endometrial malignancies, has been reported to be up to 16.9%. 1 Conventional open repair of these hernias with a suture technique yields a failure rate of 63%, while the application of a mesh prosthesis decreases the risk of recurrence to 32%. 2 After the introduction of laparoscopic repair in the 1990s, this minimally invasive procedure with alloplastic materials is gaining increased acceptance in the field of incisional hernia repair. 3 In a review of studies, it was found that, compared to conventional open repair, the minimally invasive technique was considered to be safe, with fewer complications, such as wound infection and hematoma formation. 4 However, inconclusive results were observed when comparing factors such as subsequent seroma formation, and acute and chronic pain. The majority of the trials involving similar issues showed shorter hospital stays after laparoscopic repair, especially for patients who had had longer routine hospital stays (≥5 days) in conventional repair groups, although these results were heterogeneous. The recurrence rate after repair with mesh insertion via laparoscopic and open surgery seemed to be similar, but these results were not conclusive because of short-term follow-up in the studies.
Conclusions
Theoretically, a higher risk of injury to intra-abdominal organs should also be considered. In the current case, a short hospital stay and a desirable treatment outcome were observed, but further long-term follow-up is still required to detect any delayed recurrences.
Disclosure Statement
No competing financial conflicts exist.