
Abstract
Abstract
Introduction
P
A case, which was diagnosed preoperatively as an ovarian tumor, but in which operative findings revealed a tubal lesion, which was diagnosed as PFTC on histopathology, is presented here.
Case
A 48-year-old gravida 3, para 3, postmenopausal woman, presented with gradually increasing lower abdominal pain of 4 months' duration. There was no history of postcoital bleeding, discharge per vaginum, or abdominal distension. The patient's history revealed menarche at the age of 15 years, regular cycles of 3–4 days at 28 day intervals, and menopause 3 years previous to presentation. There was no significant family history. General, systemic, and abdominal examinations did not detect any significant findings. On vaginal examination, the cervix and uterus were normal in size, with a tender mass felt through the left fornix. The right fornix was free. Serum CA-125 was slightly elevated with a value of 80 U/mL (reference range: 0–35 U/mL).
Transabdominal ultrasonography revealed a mass of ∼6.5 cm×2.5 cm of left tubo-ovarian origin, with the possibility of ovarian tumor. The uterus was anteverted and normal sized, with regular and smooth margins. Total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO) was performed, and the specimen was sent for histopathologic examination. A final diagnosis of PFTC was made. The patient is being regularly followed up, and has been disease free for the past 2 years.
Results
Pathologic findings were as follows. On gross examination, the uterus and cervix measured 6×4×2.5 cm, and weighed 72 g, which on cut section revealed an unremarkable endometrium and myometrium. The left Fallopian tube (FT) measured 6 cm in length and 2 cm in diameter, which on cut section showed a friable growth filling up the lumen and involving almost the entire length of the tube (Fig. 1a,b). Both the ovaries and the right FT were unremarkable. The serosal aspect of both ovaries and FTs was grossly uninvolved.

Microscopically, the hematoxylin and eosin (H & E) stained sections from the left FT showed a papillary growth arising from tubal epithelium (Fig. 2). Papillae had a fibrovascular core and were lined by low columnar epithelia showing pseudostratification, with cells having an enlarged nucleus and prominent nucleoli (Fig. 2, inset). The focal area of the lymphocytic infiltrate was found. There was minimal mitosis (<2/high-powered field [HPF]) and no necrosis. The tumor was invading the muscularis propria and was 2 mm away from the serosal surface. Sections from the uterus, cervix, both ovaries, and right FT were unremarkable. Final diagnosis of PFTC, serous papillary type with stage T1aN0Mx was made. As noted above, the patient was followed-up for 2 years and remained free of disease.
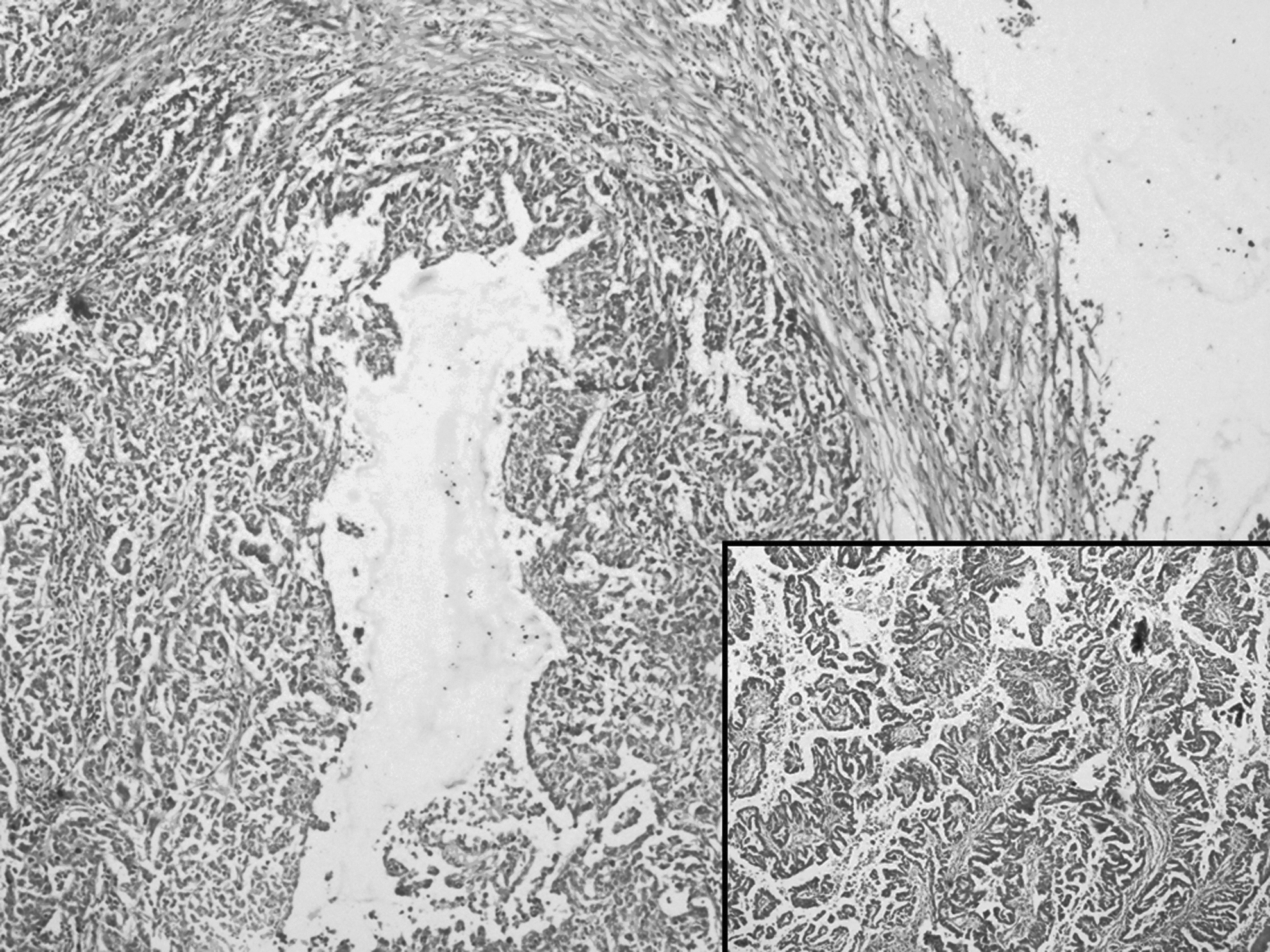
Section showing a papillary growth arising from tubal epithelium (10×, hematoxylin and eosin [H & E] stain), and insert showing complex papillae architecture (40×, H & E stain).
Discussion
PFTC is a rare malignancy in the elderly, most frequently occurring between the fourth and sixth decades, with a mean age of 64 years. 2 The incidence of PFTC is 10% rarer than secondary malignancies in the FT. PFTC and ovarian cancer have a similar etiology. 3 Exposure to high levels of gonadotropins, incessant ovulation, infertility, and pelvic inflammatory disease (PID) increase the risk, whereas high parity, breastfeeding, use of oral contraceptives, tubal ligation, and hysterectomy seem to provide protection. Recent studies have also found evidence that BRCA1 and BRCA2 germline mutations increase the risk of PFTC as well as of ovarian carcinoma. 4
The presenting symptoms are nonspecific, which often results in misdiagnosis. The most common symptoms are abnormal vaginal bleeding or discharge and abdominal pain. The clinical symptoms of PFTC and ovarian cancer are similar, with the exception of abdominal pain, which is a frequent complaint in PFTC 4 and may lead to earlier presentation, as in this case. The pain is colicky and lower abdominal in nature. The presence of a pelvic mass often leads to further investigations such as an ultrasound scan. Although the presence of the mass can thus be confirmed on imaging, its origin is not always determined, as in this case. 5
CA-125 is a useful tumor marker for the diagnosis, assessment of response to treatment, and detection of tumor recurrence during follow-up. Although not specific, elevated serum CA-125 levels have been detected in 65%–80% cases,6,7 and more frequently in advanced or recurrent tumors.1,5
The most frequent histologic type of PFTC is the serous type, which accounts for 49.5%–83.3% in different literature. 1 Others are endometrioid, mixed, undifferentiated, clear cell, and transitional cell type. Primary cases of FT carcinomas are much rarer than secondary malignancies in the FT, which most commonly arise from the ovary or endometrium. To mark a tumor as a primary in the FT, the main tumor should be confined in the tube and must arise from the endosalpinx. The ovaries and endometrium should be normal, or contain less tumor than tubes. Preoperatively, PFTC remains undiagnosed in most cases, or is presumed to be an ovarian malignancy, which is more common. Also, during the exploratory laparotomy, often it remains undiagnosed. 1 Hence, adequate sampling and histopathologic examination is essential to make a diagnosis of PFTC in all cases of presumed ovarian malignancy.
At the genetic level, both PFTC and SEOC show a high degree of similarities in the gene expression profile, which suggest that both the tumors originate from FT epithelium. 8 However, PFTC have a higher rate of retroperitoneal and distant metastasis and nodal spread.1,7 Prognosis depends upon staging, and it is poorer than for SEOC. Tubal wall invasion, location of the tumor toward the fimbrial end, bilaterality, advanced age, positive peritoneal cytology, and HER2 neu expression are noted poor prognostic factors.1,9
Management of PFTC consists of extensive surgery comprising TAH-BSO along with lymph node dissection and omentectomy. Platinum-based combination chemotherapy is the most commonly used adjuvant therapy in late stage or early stage patients with tumor infiltrating the serosa or with pre- or intraoperative ruptured tumor. 1 Stage and residual tumor are most important prognostic factors for outcome.
Conclusions
PFTC is a rare incidental diagnosis in patients undergoing an exploratory laparotomy for a presumed ovarian malignancy. Histopathologic confirmation is mandatory to make a final diagnosis and for further management of such patients.
Footnotes
Disclosure Statement
No competing financial interests exist.