
Abstract
Abstract
Introduction
O
Cases of malignant involvement of the remnant ovary have been reported. In the literature to date, 10 cases of endometrioid adenocarcinoma developing in an ovarian remnant have so far been described.8–15 Here, the first case of an ovarian clear cell carcinoma developing 3 years after total abdominal hysterectomy with bilateral salpingo-oophorectomy (BSO) for endometriosis is described.
Case
The patient was a 48-year-old woman, gravida 2, para 2, with a primary ovarian clear cell carcinoma diagnosed through a routine gynecologic examination after total abdominal hysterectomy and BSO for endometriosis. The time course of events from first surgery for endometriosis is depicted in Figure 1.

Timeline of events from initial surgery. TAH/BSO; total abdominal hysterectomy and bilateral salpingo-oophorectomy; 1, carboplatin- and paclitaxel-based chemotherapy; 2, Adriamycin, docetaxel, or irinotecan-based chemotherapy; and 3, pegylated liposomal doxorubicin-based chemotherapy.
At age 42 (August, 2007), she had undergone a total abdominal hysterectomy and BSO for pelvic pain related to endometriosis. The operative record of surgical intervention described that the left endometrioma (5–6 cm) showed severe adhesion to the left ovary, pelvic side wall, and cul-de-sac, whereas the right endometrioma (5 cm) could be separated from the surrounding tissues and was entirely removed. Left salpingo-oophorectomy was reported to have been difficult because of adhesions, resulting in incomplete removal of the left ovary and failure to ligate the ovarian vessels. The histopathologic evaluation of ovarian cyst exhibited endometriosis.
Three years and 5 months after the surgery (January of 2011), the patient experienced lower abdominal pain. A contrast-enhanced computed tomographic (CT) scan depicted a huge cystic mass in the cul-de-sac and the papillary solid components on its posterior inner surface (Fig. 2A). The mass, which measured 10×11×12 cm, encapsulated, with well-defined margin, was connected with left ovarian feeder vessels. No free fluid was found in the peritoneal cavity. Ultrasonography was consistent with the CT findings. Her serum CA-125, follicle-stimulating hormone (FSH) and estradiol (E2) levels were 10.3 U/mL (normal<37), 21.76 milli-international units (mIU)/mL, and 23.6 pg/mL, respectively. All other routine laboratory tests were within normal ranges. A preliminary diagnosis of ovarian cancer originating from the left remnant ovarian tissue was made.
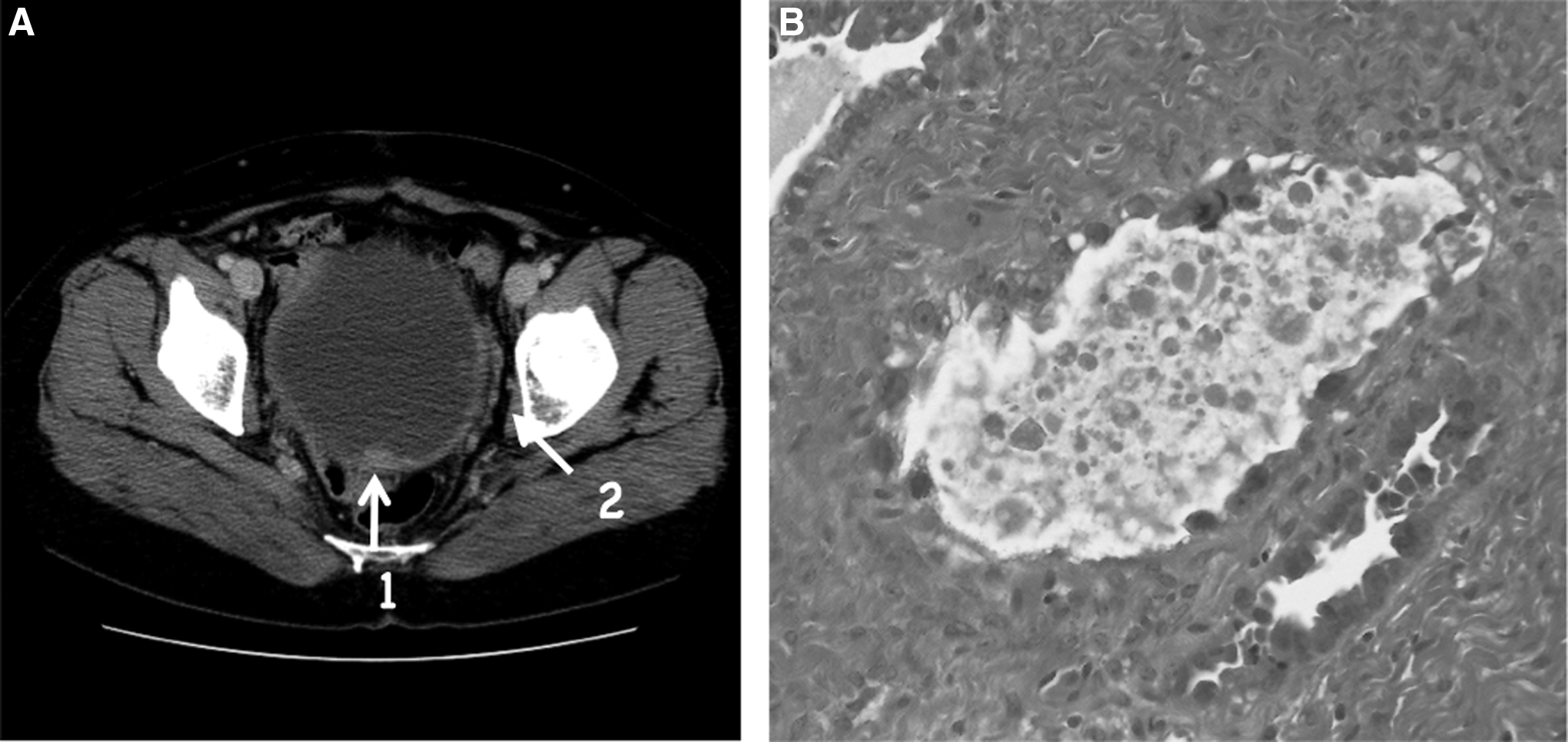
A pelvic 10 cm cystic mass and microscopic view of the tumor.
On the basis of a diagnosis of probable ovarian cancer, surgical resection of these tumors was undertaken. Dissection of the firm, vascularized, encapsulated mass in the left side of the pelvic wall was difficult, but complete removal was possible after ligating the main feeding vessels, and the left ovarian artery and vein. There was no demonstrable dissemination or ascites. Frozen section revealed serous papillary adenocarcinoma. Omentectomy and extensive pelvic lymphadenectomy were performed. The postoperative course was uneventful. Definitive histopathologic examination of the mass revealed an ovarian serous papillary adenocarcinoma associated with a clear cell carcinoma component (Fig. 2B). Washing peritoneal cytology was reported positive. The patient was submitted to six courses of systemic chemotherapy (paclitaxel- and carboplatin-based). During the chemotherapy, the CA-125 level gradually became moderately high (227 U/mL) and an intrapelvic mass measuring 5 cm in diameter was detected by magnetic resonance imaging (MRI). The patient received four additional courses of systemic chemotherapy (Adriamycin-, topotecan-, or taxane-based).
Two years after the first debulking surgery (January, 2013), the patient complained of continuous nausea, appetite loss, thirst, and lower abdominal pain. MRI demonstrated an intrapelvic mass measuring 10×12×15 cm, with relatively well-defined margins and a monolobulated cystic, low-density central area, and stenosis of the lower ureteral segment causing ureterohydronephrosis. Laboratory studies demonstrated an elevated blood urea nitrogen (BUN) level of 35 mg/dL, and a creatinine level of 3.63 mg/dL. CA-125 value was 334 U/mL. A double J stent was then placed. No bone, liver, or lung metastases were found by positron emission tomography (PET-CT). The patient was submitted to the second debulking surgery. A huge cystic mass was identified showing severe adhesions with the left obturator fossa. The liver had a normal structure, and no peritoneal carcinomatosa was observed. Extensive dissection of the left retroperitoneal space was required to completely remove the mass. Ureter stenosis was found to be caused by the huge cystic mass compression and fibrotic process associated with endometriotic lesions. Complete ureteral adhesiolysis allowed the left ureter to be freed up to the bladder.
Results
The final histopathologic evaluation revealed clear cell carcinoma, a diagnosis consistent with that for the first removed tumor. The patient received six additional courses of systemic chemotherapy (pegylated liposomal doxorubicin) (Fig. 1) and is now receiving intensive care.
Discussion
Ovarian remnant syndrome is a rare but gradually increasing complication after ovarian surgery. Even if devascularized, ovarian specimens left behind in the abdominal cavity are able to reimplant into the peritoneum and remain functional. This has been demonstrated in animal model studies.3,16 Various locations have been identified where residual ovarian tissue was detected after laparoscopic or open ovarian surgeries, including the pelvic wall, cervix, vagina, bladder, and abdominal wall wound.1,2,4–6 The incidence of ovarian remnant syndrome remains unclear because of its rarity. Recognized predisposing factors include endometriosis, pelvic inflammatory disease, and multiple previous surgeries.1–4 Ovarian remnant syndrome usually occurs within 5 years of oophorectomy. 17 As a diagnostic method, serum estradiol and progesterone titration can be helpful. Residual ovarian tissue has shown various histologic spectra, such as normal ovarian cortex, corpus luteum, endometriosis, and, rarely, malignant transformation.
The high prevalence of ovarian endometriosis among cases of malignant development in ovarian remnant syndrome raises a permanent question that has been increasingly debated in recent times; the link between endometriosis and ovarian cancer.8,18 The incidence of endometriosis in women with ovarian cancer is 8%–30%.19–21 The greatest risk is associated with malignancies of endometrioid and clear cell histology.22–24 Brinton et al. 24 evaluated a population-based cohort of women in Denmark between 1978 and 1988, and determined that women with endometriosis had a predisposition to ovarian cancer. However, this association was restricted to endometrioid (relative risk of 2.53, 95% confidence interval [CI], 1.19–5.38) and clear cell (relative risk 3.37, 95% CI, 1.24–9.14) malignancy. Similarly, Rossing et al. 21 interviewed 812 women diagnosed with ovarian cancer. When compared with population-based controls, the risk of endometrioid/clear cell ovarian cancer for women with endometriosis was threefold greater. In contrast, the risk associated with other histologic subtypes of ovarian cancer was not increased.
In the literature, 8 cases of adenocarcinoma (endometrioid type) developing in an ovarian remnant have so far been described,8–15 but the incidence of the adenocarcinoma in ovarian remnants is not known. Among the 186 patients included in the largest study, Magtibay et al. 2 did not encounter any cases of adenocarcinoma after excision of ovarian remnants. The mean time to the development of adenocarcinoma in ovarian remnants is 13.5 years (range 2–24 years) after previous surgery. The indication for previous surgery was endometriosis in 4 cases (50%), but adhesions between the ovaries and the pelvic side wall were present in all cases but 1 (87.5%). The first primary ovarian clear cell carcinoma described after total abdominal hysterectomy and BSO is reported here. Special care should have been taken to ensure extensive dissection of the infundibulopelvic peduncles, in case of severe adhesions or endometriosis, to avoid leaving any active ovarian tissue behind. When ligating ovarian feeder vessels, bipolar electrocoagulation to the infundibulopelvic ligaments may lead to an ovarian remnant, especially in cases of with a history of multiple pelvic surgeries, adhesions, or endometriosis. Surgical treatment may be the better choice.
Because endometriosis is known to possess may features of benign processes, with the potential for malignant development, and to behave as an estrogen-dependent neoplasm, the utility of estrogen replacement therapy must be discussed in menopausal patients. When endometriotic adhesions are diagnosed during BSO, because of the subsequent risk of ovarian remnant syndrome and the subsequent malignant development, the use of estrogen alone is questionable, and it may be preferable to give tibolone or combined estrogen and progestogens in such a case.
Conclusions
For pelvic masses suspected of malignancy after BSO, the possibility of ovarian remnant syndrome should be considered. Use of aspiration for cytologic examination and confirmation of diagnosis can be hazardous, as reported in 2 cases of primary ovarian malignancy with negative cytology study results.10,11 A diagnostic laparotomy or laparoscopy may be recommended to determine the best approach.
Footnotes
Disclosure Statement
No competing financial interests exist.