
Abstract
Abstract
Introduction
T
Case
A 39-year-old nulliparous woman presented to Dr. Ramesh Hospital with primary subfertility of 1 year's duration. Serum follicle stimulating hormone and luteinizing hormone levels taken on the 2nd day of her menses were elevated. Husband's semen analysis was normal. She was counselled for IVF-ET with donor oocytes. Diagnostic hysteroscopy performed prior to IVF was normal. She conceived in the fourth cycle of IVF-ET. Three embryos were transferred, and serum beta human chorionic gonadotropin (hCG) level taken 16 days after ET was 1132 mIU/mL which increased to 1600 milli-international units (mIU)/mL after 72 hours. Transvaginal ultrasound (TVS) examination revealed a thickened endometrium measuring 13 mm. Two days later, the patient presented with complaints of lower abdominal pain and vaginal bleeding. Clinical examination revealed tenderness in the lower abdomen. Serum beta hCG concentration was 2606 mIU/mL. The uterus was empty, and a 4.6×3.5 cm complex lesion with a central cystic area was noted in the left adnexa on TVS examination. There was a moderate amount of intraperitoneal fluid, with internal echoes suggestive of a ruptured ectopic pregnancy with pelvic hematoma and hemoperitoneum (Figs. 1 and 2). Laparoscopy revealed a hemoperitoneum of 250 mL and a bilateral tubal pregnancy, left tubal abortion, and right unruptured ampullary pregnancy (Figs. 3–4). Bilateral salpingectomy was performed and histopathology confirmed the diagnosis of bilateral tubal pregnancy.

Ultrasound images of the left adnexa and pelvic hematoma.

Ultrasound images of the empty uterine cavity and right adnexa.
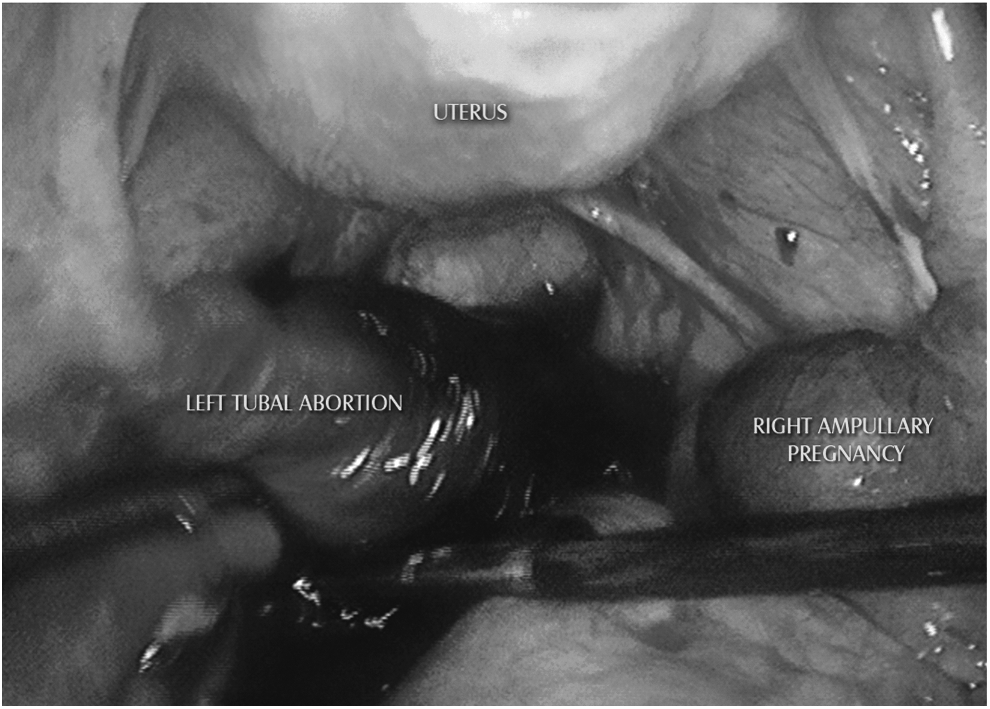
Laparoscopic image of bilateral ectopic pregnancy with pelvic hematoma.
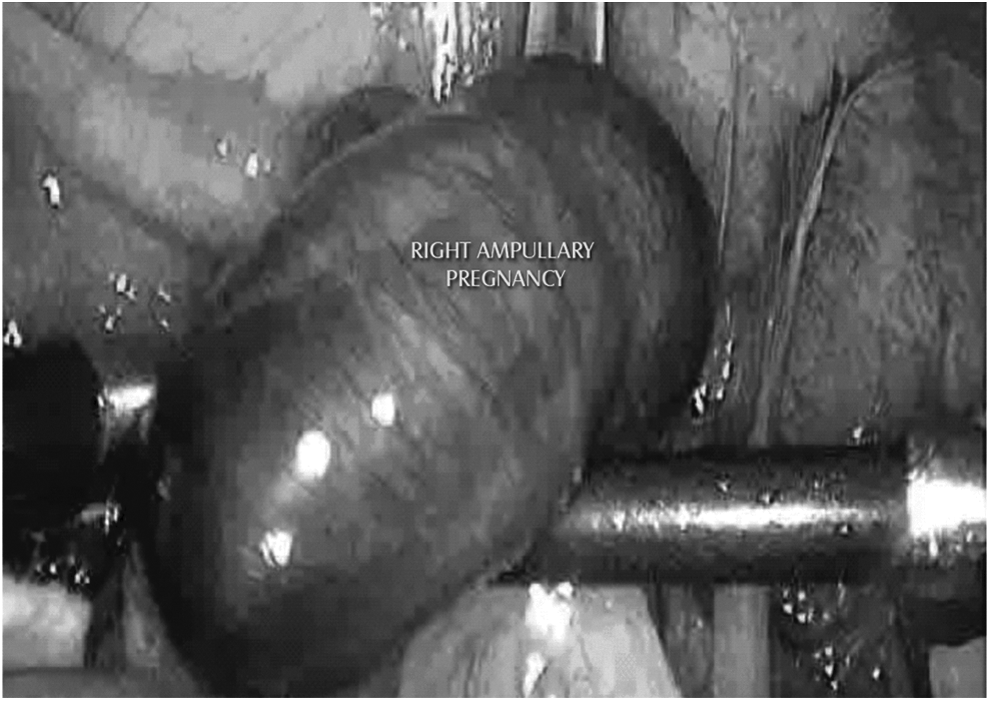
Laparoscopic image of right unruptured ampullary pregnancy.
Results
The postoperative period until discharge was uneventful, and subsequently the patient was lost to follow-up.
Discussion
Bilateral ectopic pregnancies are classified into primary and secondary types. 5 Primary bilateral ectopic pregnancy is defined as the occurrence of at least two concomitant spontaneous pregnancies, none of which are intrauterine, with both being located in structures of the opposite side. In secondary bilateral ectopic pregnancy, two simultaneous gestations take place, neither of them eutopic, localized in structures of opposite sides, and after manipulation of the physiology by means of drugs used for assisted reproduction. In 2007, Rios et al. analyzed 42 reported cases of bilateral ectopic pregnancy that had occurred in the preceding 10 years. 5 Half of them were spontaneous bilateral ectopic pregnancies. In 19 cases (45%), the bilateral ectopic pregnancy was the result of ART that involved ovarian stimulation and in two cases (5%), the authors did not explain the origin of the condition. With regard to the ART, both intrauterine insemination and IVF-ET shared an equal percentage.
To substantiate the anatomic-pathologic diagnosis of bilateral ectopic pregnancy, in 1939 Fishback proposed that two embryos should be observed in any portion of the tubes accompanied by chorionic tissue to substantiate anatomic-pathologic diagnosis of bilateral ectopic pregnancy. 6
Ectopic pregnancies initiating during a woman's natural cycle, and those that are a result of ART, are caused by different pathophysiologic mechanisms. Precedent tubal disease is a common risk factor for both primary and secondary bilateral ectopic pregnancies, and may be found in 12% of patients undergoing IVF-ET for tubal reasons. Apart from the known pathologic factors, double spontaneous ovulation must occur to produce primary bilateral ectopic pregnancy.
There are three theories to explain the cause of bilateral ectopic pregnancy after ART. 7 First, embryos may be injected directly into the tubes because of deficient transfer technique. Second, embryos correctly transferred to the endometrial cavity can migrate regressively to the tubes as a consequence of endometrial secretions that push them in that direction. Third, the spray effect produced during transfer when emptying the hypodermic syringe can possibly push the embryos toward the tubal portions. However, in spite of these mechanisms, in the presence of normal tubes, the embryos should return to the endometrial cavity, simulating the normal journey of a fertilized egg in that direction, but in dysfunctional or damaged tubes, their implantation outside the eutopic endometrium can occur more frequently. Hence, patients with tubal disease and permeable ostia seem to have a higher risk of ectopic pregnancy, either unilateral or bilateral, no matter how careful the transfer technique, the length of the catheter introduced, the quantity of transfer medium, the number of transferred embryos, or the type of ovulation induction used. 8 In an 8-year review of ectopic pregnancy rates in donor egg recipients and standard patients undergoing IVF-ET, the ectopic pregnancy rates were 0.6% and 0.9% in the two groups, respectively. Donor egg recipients were found to have a significantly lower incidence of tubal disease than standard IVF patients. 9 In the patient reported here, although there was no evidence of tubal disease at laparoscopy, it was not possible to comment about the tubal status, as there was no preoperative assessment of tubal patency/function.
Clinical findings of bilateral ectopic pregnancy do not differ very much from that of unilateral ectopic pregnancy; however, there is a greater risk of rupture and hemorrhagic shock. There is more difficulty in diagnosing this condition as neither the serum Beta hCG levels nor TVS are conclusive. In the review by De Los Rios et al., 5 serum beta hCG values were reported at the moment of a presumptive ectopic diagnosis in 15 cases and ranged from 27 to 226.768 mIU/mL. The gestational age in weeks after the last menstruation was 6.7 weeks on average at the moment of diagnosis (range, 5–9 weeks). Serum beta hCG concentration was within ranges recognized for the corresponding gestational ages in 9 cases (60%), lower than expected in 5 cases (33.3%), and above the value regarded as normal for the gestational age in only 1 case (6.6%). In the case reported here, serum beta hCG corresponded to a gestational age of 5 weeks, as per the period of amenorrhea.
Of the 19 cases of secondary bilateral ectopic reviewed by De Los Rios et al., 2 (10.5%) were recognized and diagnosed preoperatively by ultrasonography. The case reported here was diagnosed as unilateral (left) ruptured tubal ectopic pregnancy. A high index of suspicion is necessary to reach a correct diagnosis by means of ultrasound scanning. Laparoscopy is not only the ideal diagnostic method but also the preferred modality for treatment. Treatment of choice for secondary bilateral ectopic pregnancy is laparoscopic bilateral salpingectomy, especially when assisted reproduction techniques such as IVF-ET are used. However, a more conservative procedure, bilateral salpingostomy, may be performed if tubes are essential for future treatment in the form of ovulation induction and intrauterine insemination. Future reproductive performance in such cases has not been followed up or reported by authors. Medical treatment with methotrexate can be offered if a correct diagnosis of unruptured pregnancy is made preoperatively and the patient is clinically stable. Methotrexate can be administered in a dose of 1 mg/kg body weight under ultrasound guidance into the gestational sac. 10
Conclusions
Future reproductive prognosis and recurrence rates of bilateral ectopic pregnancy are unclear, as no follow-up studies are available. There is one case report of a successful intrauterine pregnancy after treatment of a secondary bilateral ectopic pregnancy, which deserves special mention. 11 A woman had conceived after ovulation induction following tubal anastomosis. Bilateral tubal pregnancy was diagnosed at laparoscopy, which was converted to minilaparotomy in view of dense adhesions. Left salpingectomy and milking of the right tube were performed. Subsequently, the patient conceived naturally within 15 weeks of surgery, and had an uneventful pregnancy.
This case report illustrates that clinical diagnosis of bilateral tubal pregnancy after IVF-ET may be difficult, and that laparoscopy is the gold standard for diagnosis. In all pregnancies following ART, along with serum Beta hCG monitoring, there should be a high index of suspicion to diagnose ectopic pregnancy while performing ultrasound, in order to avoid missing concomitant contralateral ectopic and heterotopic pregnancies.
Footnotes
Disclosure Statement
No competing financial interests exist.