
Abstract
Abstract
Introduction
I
The case of a giant IMT associated with GP, with the largest diameter of the ovarian tumor measuring 45 cm, and weighing 22.8 kg, in 15-year-old girl, is presented. This appears to be the largest IMT with GP reported in the literature.
Case
A 15-year-old nulligravida came to the Department of Gynecologic Oncology, at the Delhi State Cancer Institute, New Delhi, India, with complaints of abdominal distension and amenorrhea of 2 years' duration. Menarche had occurred when she was 12 years of age; she had regular and normal menstrual periods, lasting up to 3–4 days. Her family, past medical, and surgical histories were unremarkable. Her abdomen was overdistended and showed a huge mass equivalent in size to 30 weeks of gestation. Vaginal examination was not performed because the patient was a virgin.
Hematologic and biochemical test results were within normal limits. Serum tumor markers revealed an elevated alpha-fetoprotein (AFP), CA-125, CA-19.9, CA-15.3, CA-72.4, and carcinoembryonic antigen (CEA), and normal β-human chorionic gonadotropin (hCG) (Table 1). Abdominal ultrasound (USG) examination showed a large, lobulated, multicystic mass with internal calcification and a solid component occupying the entire abdomen along with gross tense ascites. Computed tomography (CT) scan revealed a large solid cystic abdominopelvic mass 40×38×20 cm in size, with multiple calcific and lipid- containing foci, along with an enhancing solid component and thick septation with complicated ascites and thickened omentum (Fig. 1). Ascitic fluid cytology smear was paucicellular and negative for malignant cell. The patient was admitted with a preliminary diagnosis of ovarian neoplasm. A left salpingo-oophorectomy and omentectomy were performed and sent for histopathologic examination, which revealed grade I IMT with GP.

Computed tomography scan image showing a large solid cystic abdominopelvic mass with areas of calcification.
AFP, α-fetoprotein; CEA, carcinoembryonic antigen; β-hCG, β-human chorionic gonadotropin.
Results
General results
Serum tumor markers 2 months postsurgery were found to be within normal limits (Table 1). The patient's menstrual periods resumed 4 months after the surgery. She had no complications at her 6 month follow-up visit.
Pathologic findings
Samples from left salpingo-oophorectomy as well as omentum and right ovarian biopsy were examined by the Pathology Department of the Swami Dayanand Hospital, Delhi, India. On gross examination, the left ovarian mass measured 45×40×24 cm, and weighed 22.8 kg (Fig. 2A). The cut surface was variegated, with solid and cystic areas filled with seromucinous fluid (Fig. 2B). Bony hard areas along with tuft of hairs were also identified. The omentum sample received measured 44×10×1 cm, and was finely granular on palpation.

Hematoxylin and eosin (H & E) stained sections from the ovarian mass revealed a predominantly ectodermal component along with various structures representing differentiation toward all three germinal layers. (Skin with adenexal structures, respiratory epithelium, gut mucosa, smooth muscle, adipose tissue, bone, cartilage, and astroglial tissue are shown in Fig. 3 A–D). The focal area showed a blastemal element. H & E stained sections from the omentum showed nodular mature astroglial tissue (Fig. 4A) which was positive for glial fibrillary acidic protein (GFAP) (Fig. 4B) and S-100, and negative for smooth muscle actin (SMA). Isolated lymph nodes showed features of reactive lymphoid hyperplasia. A section from the right ovarian biopsy showed normal histology. A final diagnosis of grade I, stage Ia IMT with GP was made.
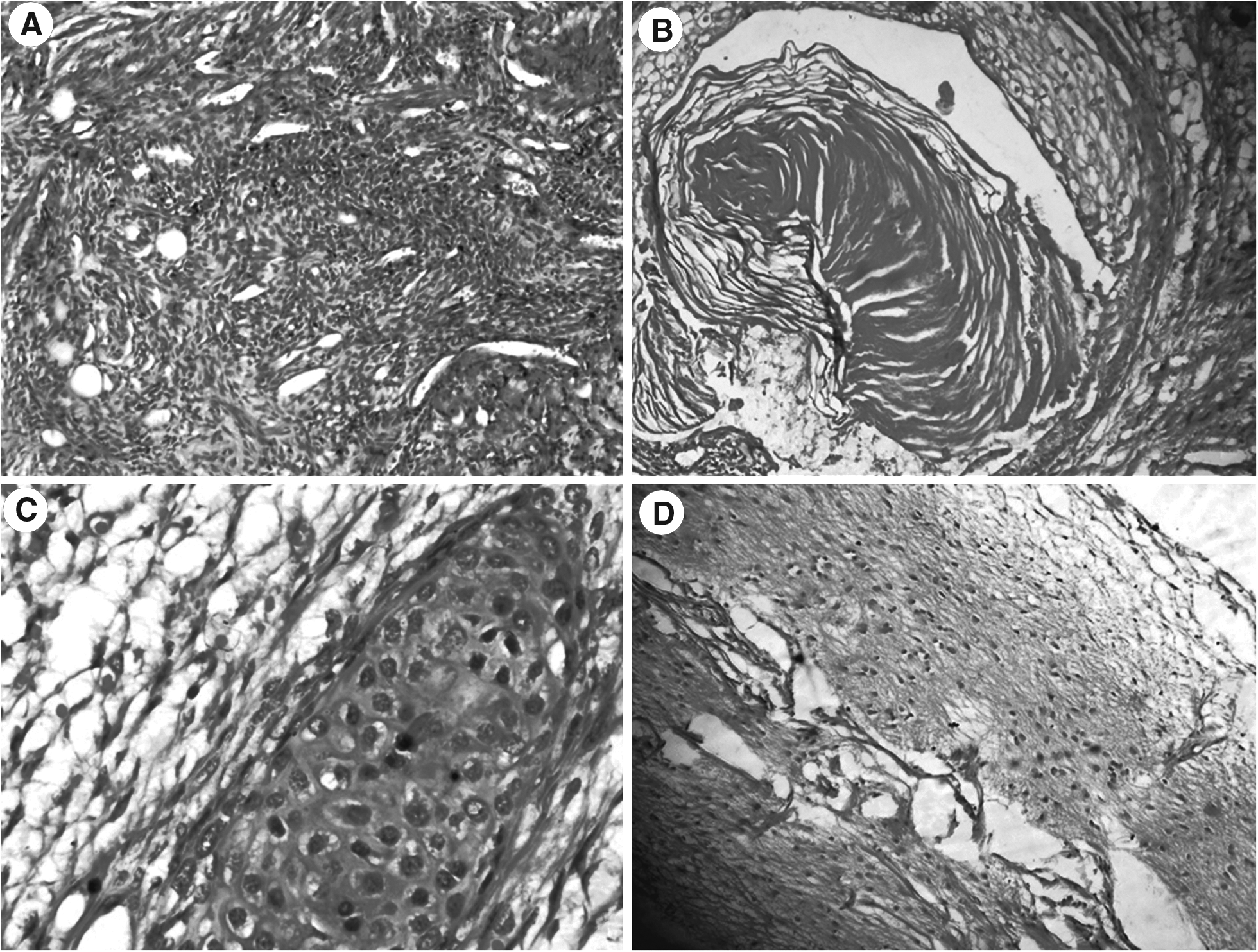
Photomicrographs showing various structures with differentiation toward all three germinal layers (hematoxylin and eosin [H & E stain],×10 and×40).
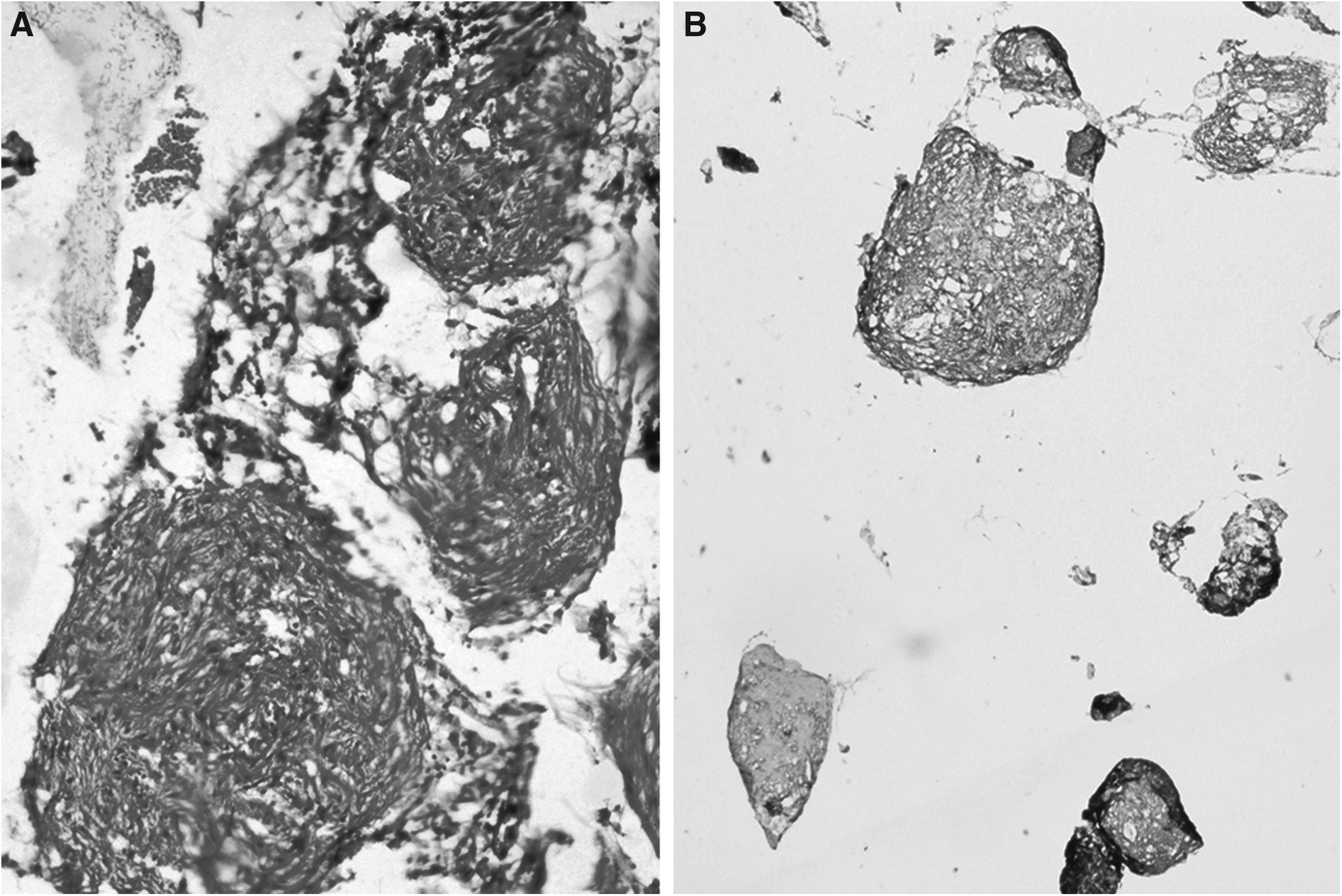
Photomicrograph showing:
Discussion
Ovarian IMT is a malignant germ cell tumor, and represents 3% of all teratomas, 1% of all ovarian cancers, and 20% of malignant ovarian germ cell tumors. 5 IMT is composed of tissues derived from all three germ layers (ectoderm, mesoderm, and endoderm), with immature or embryonic structures. 1 IMT are seen most commonly in childhood and adolescence, with peak incidence at 15–19 years of age. 1 The tumor size ranges from 5 to 31 cm, with median size of 17 cm.3,4 The case of a giant IMT with the largest diameter measuring 45 cm, in 15-year-old girl, was reported here. This is believed to be the largest IMT with GP reported in the English language literature. Abdominal mass and abdominal pain are the most common presenting symptoms, as occurred in this case. 6 IMT is almost always unilateral; however, bilateral IMTs have also been reported. 1 Histologic grading of IMT is essential for therapeutic and prognostic consideration. Thurlbeck and Scully 7 graded these tumors based on the amount of neuroepithelium present. Older patients tend to have lower grade tumors than younger patients. 8
The serum tumor marker most commonly related to IMT is AFP. Diagnosis of IMT by tumor marker is more sensitive when combined with detection of CA-125, CA-15.3, and AFP. 9 Imaging studies of IMT show cystic appearance with fat content and calcification.
GP is a rare complication of IMT, and can be defined as the occurrence of nodules of mature glial tissue in the peritoneum. It is controversial whether glial tissues are derived from maturation of associated teratomatous tissue that has implanted in the peritoneum, or from glial differentiation of subperitoneal stem cells. 2 GP is an infrequent occurrence associated with mature or immature teratoma of the ovary. Recognition of this entity is important, because it may easily be mistaken for intra-abdominal carcinomatosis, leiomyomatosis, endometriosis, or tuberculosis. On histologic analysis, the implants of GP resemble benign mature glial tissue. Malignant transformation of these implants is exceedingly rare. 10 GFAP immunostains confirm the astroglial nature of these implants. Strong expression of GFAP suggests that tumor cells are mature and often well-differentiated. 11 The mature nature of implants generally implies a favorable prognosis, even in patients with IMT. The presence of GP does not modify the prognosis, and treatment of the patient is warranted per grade and stage of IMT. 12 Thorough and extensive sampling is essential to document the benign nature of these implants, and to exclude presence of immature elements that may imply a poor prognosis and require aggressive therapy. 13
Because these tumors are more prevalent in young adults, treatment should be by conservative surgery. Unilateral salpingo-oophorectomy is the preferred procedure. 14 Patients with grade II or III tumors or a more advanced stage disease should be treated with adjuvant chemotherapy containing bleomycin, etoposide, and cisplatin, in addition to surgery. 14 Thorough microscopic examination is essential to exclude other germ cell elements, and for proper grading of teratoma, and also, to rule out any immature teratomatous component in peritoneal implants. GP are essentially mature deposits that do not adversely affect the outcome of the patient. Because the lesions of GP are extensive, complete excision is mostly difficult, and the potential for recurrence is high and, therefore, careful monitoring of residual lesions is required. Hence, although GP does not have prognostic influence, regular follow-up is needed. 12
Conclusions
This case demonstrates that IMTs can grow to an enormous size (weighing >20 kg) and should be considered whenever gross abdominal distension is seen in young women. GP is a rare occurrence, and is seen most commonly with IMT of ovary. Although grossly mimicking carcinomatosis, GP is essentially benign, and does not adversely affect the prognosis. Therefore, histologic confirmation is mandatory to make the final diagnosis and to exclude the presence of immature elements in peritoneal implants.
Footnotes
Disclosure Statement
No financial conflicts exist.