
Abstract
Abstract
Introduction
A
Cases
A series of 4 cases of Fallopian-tube torsion, which were encountered at the West Hertfordshire National Health Service (NHS) Trust from 2010 to 2012, is reported here.
Case 1
A 23-year-old woman presented with severe right-sided abdominal pain in February 2010. She had had two previous admissions with similar pain in September and December of 2009. US scans had been performed during the previous admissions. A US scan in September 2009 showed two simple cysts in the right adnexa, with the larger one measuring 4 cm. The US scan in December 2009 showed a 4.3-cm cyst in the right adnexa/Pouch of Douglas (POD) with an 8-mm echogenic area apparently arising from the cyst wall. On the two previous occasions, the patient's pain remitted spontaneously; hence she was not was not treated surgically on an emergency basis. During the current admission, a US scan was not performed; laparoscopy was performed. A right-sided fimbrial cyst was seen, with a torted right Fallopian tube. The uterus, both ovaries, and the left tube were found to be normal. A partial right salpingectomy was performed. Histology showed a normal Fallopian tube and a benign paratubal cyst.
Case 2
A 28-year-old woman was admitted in March of 2010. She was 6 weeks pregnant with lower abdominal pain. A US scan showed a viable intrauterine pregnancy, with several thick-walled cysts in the left ovary, free fluid around the right ovary, which was 84×63×93 mm, and free fluid with debris (possibly clots) in the POD. The findings were considered to be highly suggestive of a heterotopic pregnancy. Laparoscopy was performed, which showed the right Fallopian tube to be grossly enlarged and twisted on itself four times. Hematosalpinx was noted. A partial right salpingectomy was performed. Histology of the specimen showed it to be a Fallopian tube with congested blood vessels. No tubal pregnancy was seen on histology.
Case 3
A 53-year-old woman was admitted for surgery in April 2011, with right iliac fossa pain and rebound tenderness, nausea, and anorexia. She was hemodynamically stable and had a white cell count of 4.1. She had had her last menstrual period 4 days before admission, and had been having regular menstrual cycles. A US scan was performed, which showed a bulky uterus, with a small posterior-wall fibroid growth and a 3-mm endometrium; both ovaries appeared to be normal. Significant fluid was seen in the POD and pelvic region. Prominent bowel loops were seen, but the right iliac fossa was not visualised optimally. Appendicitis was not excluded. Laparoscopy was performed. Bilateral hydrosalpinx was noted. The right tube was torted and necrotic (Figs. 1 and 2). Some hemorrhagic fluid was seen in the peritoneal cavity. The appendix also appeared to be inflamed. A right salpingectomy and appendectomy were performed. The patient was given 2 weeks of doxycycline postoperatively. Histology showed Fallopian-tube infarction and lymphoid hyperplasia of the appendix, with no active inflammation.
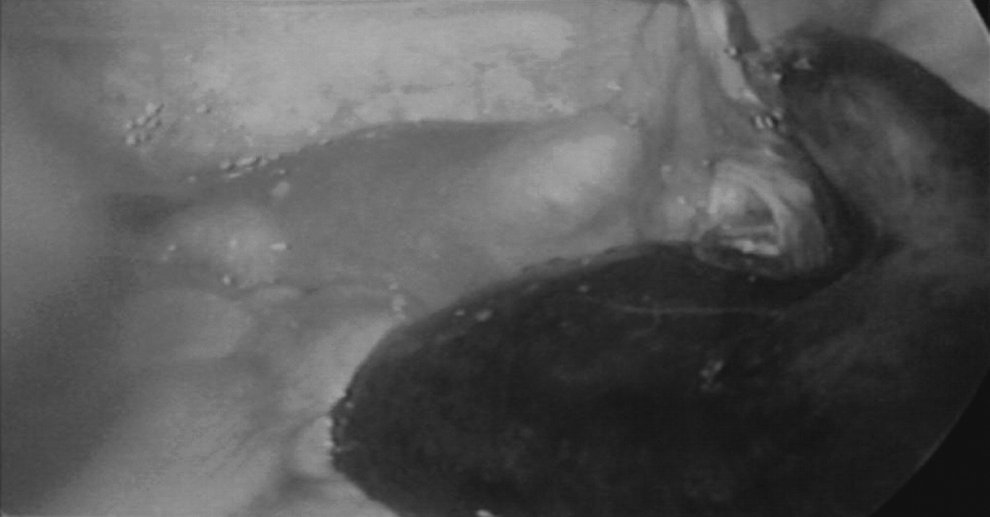
The right Fallopian tube is torted and necrotic.

Left hydrosalpinx.
Case 4
In April 2012, a 21-year-old woman with achondroplasia and a history of previous appendectomy was admitted, with a current history of right lower abdominal pain of 1 week's duration, radiating to the lower back, and getting progressively worse. She had been given antibiotics by a general practitioner (GP) for suspected pelvic inflammatory disease. She had irregular menses, her last menstrual period having been 2 months earlier; however, the urine pregnancy test was negative. A pelvic US scan was performed, which showed a right ovarian hemorrhagic cyst, 7×5×4 cm in size, that was suggestive of ovarian-cyst torsion. Laparoscopy was performed, and the right Fallopian tube was seen to be twisted twice, and a right ovarian cyst was noted, which was hemorrhagic but not torted. A tube-conserving operation was performed by “un-twisting” the tube, following which it turned pink. A right ovarian cystectomy was performed. This patient's postoperative recovery was uneventful, except for omental herniation in the umbilical wound on POD-2, which was reduced during the patient's hospital stay.
Results
US scan findings were nonspecific and variable. One of the cases was a suspected heterotopic pregnancy. Laparoscopy in all these cases revealed isolated Fallopian-tube torsion. In 3 cases, salpingectomy was performed. In 1 case, tube-conserving surgery was performed to untangle the tube. All of the women had uneventful recoveries.
Discussion
Earlier studies/case reports have reported the incidence of isolated Fallopian-tube torsion to be 1:1,500,000; however, the incidence appears to be higher than that. West Hertfordshire NHS Trust caters to a core population of ∼500,000, and 4 cases were encountered in 3 years.
The cause of Fallopian-tube torsion is unknown. 6 However, various hypotheses have been posited explaining the etiology of occurrence of isolated Fallopian-tube torsion, which includes an initial obstruction of adnexal veins and lymphatics, leading to pelvic congestion and edema, enlargement of the fimbrial end, and subsequent partial to complete torsion of the affected tube. 7 It can occur without ipsilateral ovarian involvement associated with pregnancy, hematosalpinx, hydrosalpinx, ovarian or paraovarian cysts, and other adnexal changes, or even with an otherwise normal Fallopian tube. 8 Various factors have been associated with the occurrence of Fallopian-tube torsion and have been divided into two categories: intrinsic factors such as congenital anomalies of the Fallopian tube, acquired pathology of the Fallopian tube, such as hydrosalpinx, hematosalpinx, neoplasm, surgery, autonomic dysfunction, and abnormal peristalsis; and extrinsic factors such as changes in the neighboring organs such as neoplasm, adhesions, pregnancy, mechanical factors, movement or trauma to the pelvic organs, or pelvic congestion. 9 The right Fallopian tube is commonly affected. This may be because of the presence of the sigmoid colon on the left side, slowing venous drainage on the right side, which may result in congestion.10, 11 However, there have been various case reports of left-sided tubal torsion.12, 13
Conclusions
Laparoscopy is the “gold standard” for treatment, as early diagnosis can spare the Fallopian tube and spare future fertility. 14 However, the possibility of recurrence of torsion of the Fallopian tube, although rare, should be considered as well. 15
Footnotes
Disclosure Statement
No competing financial interests exist.