
Abstract
Abstract
Introduction
T
This article presents a case of a woman who underwent a diagnostic hysteroscopy after an unsuccessful IVF attempt in another center. At that center, she had an embryo transfer although she had a reduced endometrial thickness of 4 mm. This patient had undergone an ovulation-induction treatment cycle with clomiphene citrate (CC) 1 month prior to the abovementioned IVF cycle. She also a history of a dilatation and curettage (D+C) for removal of a polyp in her cervical canal.
Case
A 37-year old woman, para 0+0, presented for an evaluation because of primary couple infertility, after a failed IVF cycle in another IVF center. Her antral follicle count (AFC) during that cycle was 12, her anti-Müllerian hormone level was 10 pmol/L, and mild male-factor infertility was also present. In a prior IVF cycle before this last one, she had undergone a cycle of ovulation-induction with CC and an unsuccessful intrauterine insemination (IUI) attempt. The IVF protocol followed in this case was a standard long protocol, with stimulatory doses of 225 international units of follicle-stimulating hormone daily. Egg recovery took place on day 13 of stimulation, and 10 eggs were retrieved. Embryo transfer took place 3 days later; this was a double embryo transfer of two good-quality, day-3 embryos. This transfer was performed although she had a documented, reduced endometrial thickness of ∼4 mm. Her reduced endometrial thickness was attributed to the CC that she had received nearly 40 days prior to her ovulation-induction. This medication and subsequent ovulation-induction were all according to a standard IVF regimen.
During her clinical examination at the current center, this patient revealed that she had undergone a D+C for removal of a polyp in her cervical canal. A transvaginal ultrasound on day 5 of her menstrual cycle revealed an endometrial thickness of 3.5 mm; but the definition of it was hazy. Therefore, taking all of this into account, a diagnostic hysteroscopy was arranged with the expectation of finding and treating endometrial adhesions.
Results
Indeed, the findings of the hysteroscopy were endometrial and cervical-canal adhesions as well as an unexpected finding of an ∼3-mm-size endometrial polyp (Figs. 1 and 2). The adhesions were treated appropriately with hysteroscopic scissors, and the polyp was removed. Specimens were sent for pathologic examination, and the results proved that the latter diagnosis regarding the polyp was correct.
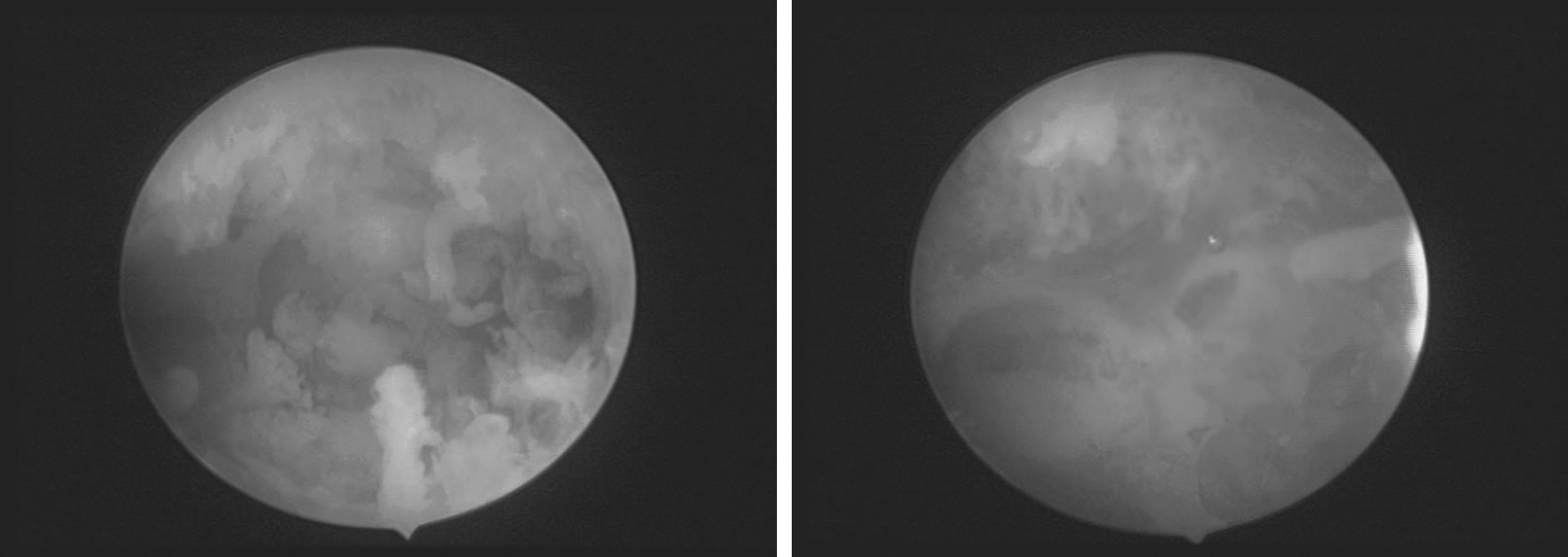
Two views of multiple adhesions of the endometrial cavity.
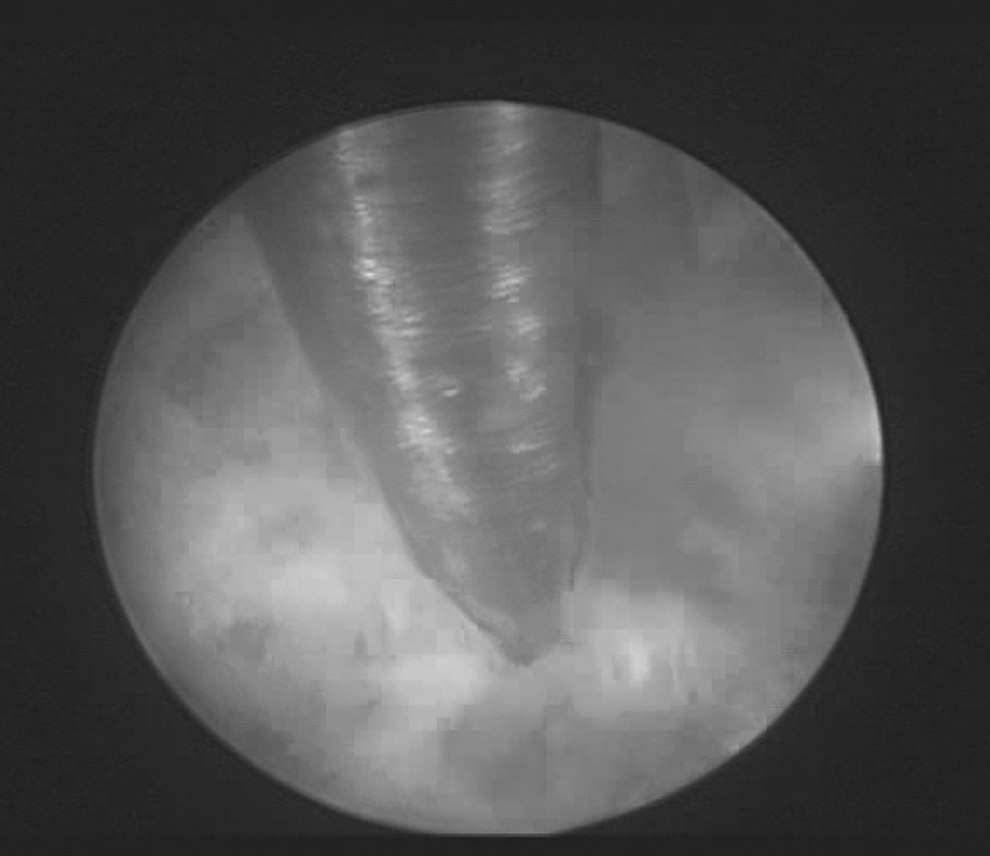
Treatment of endometrial adhesions with hysteroscopic scissors.
No additional treatment—such as oral contraceptive pills or an intrauterine device of any kind—was used postoperatively by this patient, despite the current authors' suggestion to do so. She refused this treatment, because she wanted to have a new IVF treatment cycle as soon as possible.
Discussion
Thin endometrium is a finding that can play a crucial role in IVF as this condition is associated with low implantation rates, especially under a cutoff value of 6 mm.1–3 One of the most common reasons for the presence of a thin endometrium is the use of CC for ovulation-induction. However, the current case showed that, despite the use of CC in a previous treatment cycle, it would have been a mistake to attribute this patient's thin endometrium only to CC alone, as one might have guessed. 4 The value of taking a careful medical history—which revealed the previous D+C (with its possible effect on adhesion-creation) in this case 5 —should never be underestimated. The use of hysteroscopy as a diagnostic and therapeutic tool can help with the management of thin endometrium, as more than one of its etiologic factors may coexist and thus complicate management.
Conclusions
Hysteroscopy should always follow the diagnosis of a thin endometrium when relevant factors may coexist and thus jeopardize IVF success. This case report highlights the need for hysteroscopic intervention in cases of thin endometrium during IVF, especially when there is a relevant past clinical history.
Footnotes
Disclosure Statement
No competing financial conflicts exist.