
Abstract
Abstract
Introduction
C
Modern clinical practice is evidence based; what forms the gold standard for this evidence-based practice is knowledge from randomized controlled clinical trials. Many of the CS techniques have not yet been rigorously evaluated in randomized controlled trials and it is not known whether any are associated with better outcomes for the women and babies. Because of the huge number of women who undergo CS, even small differences in postoperative morbidity rates between techniques could translate into improved health for a substantial number of women and significant savings of costs and resources for health services.6,9 Hence, we planned this study at a tertiary care hospital to compare the standard lower segment cesarean section (LSCS) with the circular opening and concentric suturing (COCS) technique of uterine incision for CS. This is an innovative technique. 3
Aims and Objectives
1. To study the feasibility of the innovative technique, the COCS method of CS.
2. To compare this novel technique with standard LSCS.
3. To evaluate the merits and demerits of such a technique.
Materials and Methods
A prospective comparative study was performed in a single unit of the Obstetrics and Gynecology Department at a tertiary hospital from 2009 to 2011. Institutional ethics committee approval was sought before commencing the study. Informed written consent from the patients was obtained before their participation in the study.
In this prospective single-center comparative study, patients were recruited with the following inclusion and exclusion criteria.
Inclusion criteria
1. Patients willing to participate in the study where it is feasible to perform this technique.
2. Elective as well as emergency CS.
Exclusion criteria
1. Previously scarred lower uterine segment.
2. Poorly formed lower uterine segment.
3. Anterior placenta previa.
In this study, patients were divided into two groups with 30 patients in each group as follows.
Group 1: Patients in this group were operated by standard LSCS.
Group 2: Patients in this group were operated by a novel technique of COCS method for LSCS.
COCS technique for LSCS
1. Abdomen was opened in layers by Pfannenstiel incision.
2. Parietal peritoneum was opened.
3. Uterovesical fold of peritoneum was identified and a small incision was made in the center on a loose part.
4. Uterovesical fold was then dissected from the lower uterine segment.
5. Bladder was retracted with the use of bladder retractor.
6. A stay suture was taken at the center just above the dome of the bladder on the lower uterine segment.
7. A stab or cruciate incision was made in the lower uterine segment, which was extended in a radial (circular) manner with four right-angled retractors.
8. Baby was delivered.
9. Placenta was delivered by the controlled cord traction method
10. Uterine incision was sutured with delayed absorbable suture (No 1 polyglactin) in a concentric manner (purse string suture) in two throws with uterus in situ.
11. Hemostasis confirmed.
12. Uterovesical fold of peritoneum was then approximated.
13. Peritoneum and rectus muscle were closed in an interrupted manner.
14. Rectus sheath was closed in a continuous interlocking manner.
15. Skin was closed with interrupted or subcuticular sutures (Figs. 1–5).
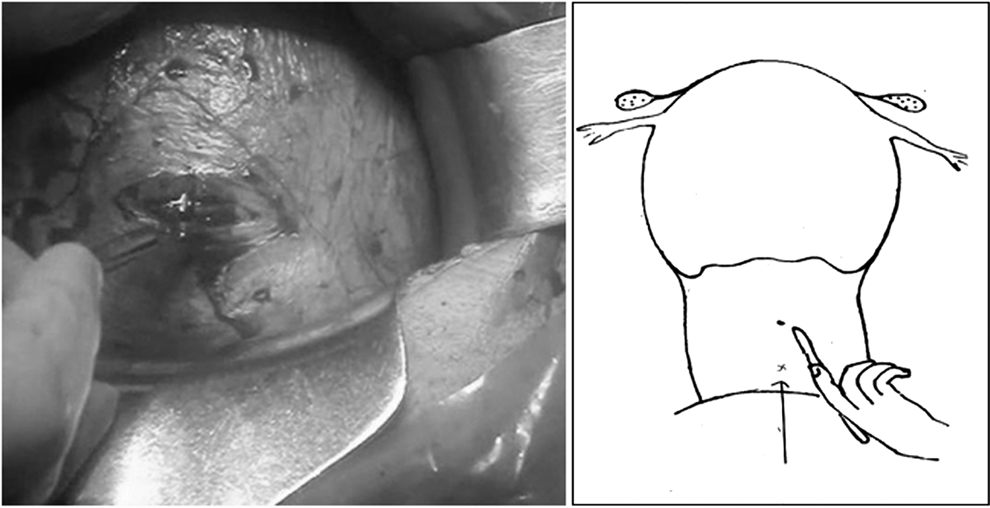
Stab incision is taken on uterus.
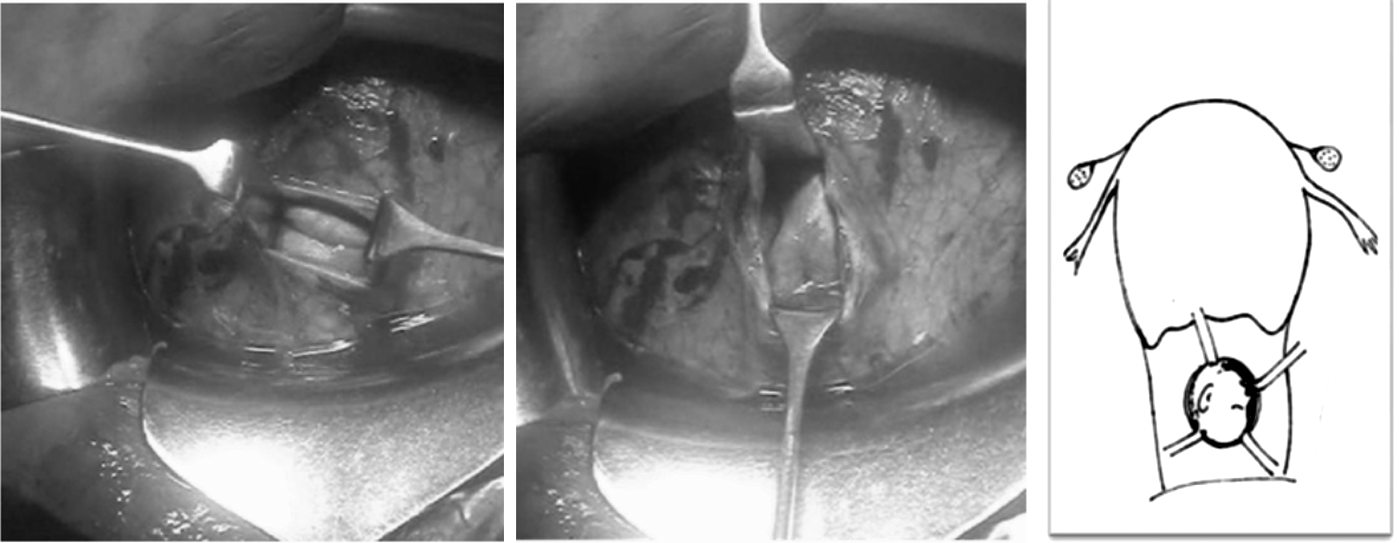
Incision extended with right-angled retractors in a radial manner.

Circular incision is sutured in a concentric manner.
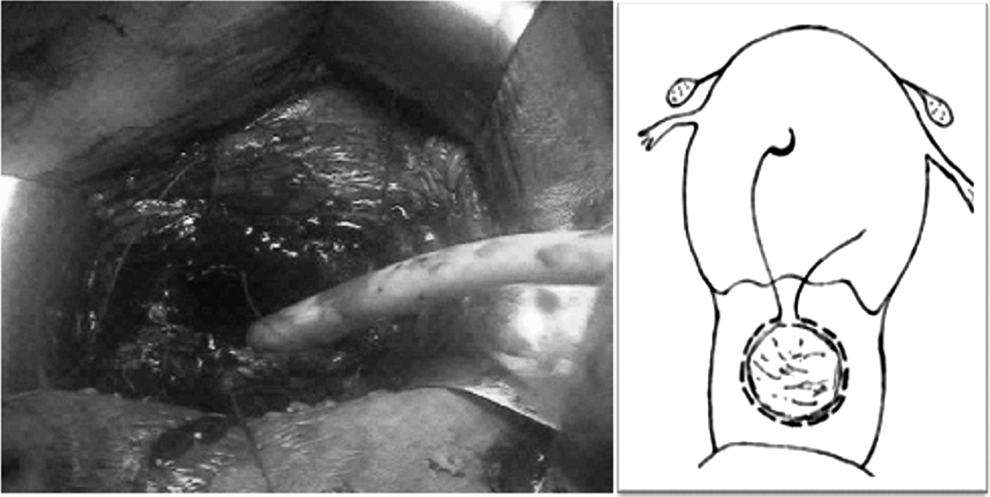
Incision being sutured in concentric suturing.
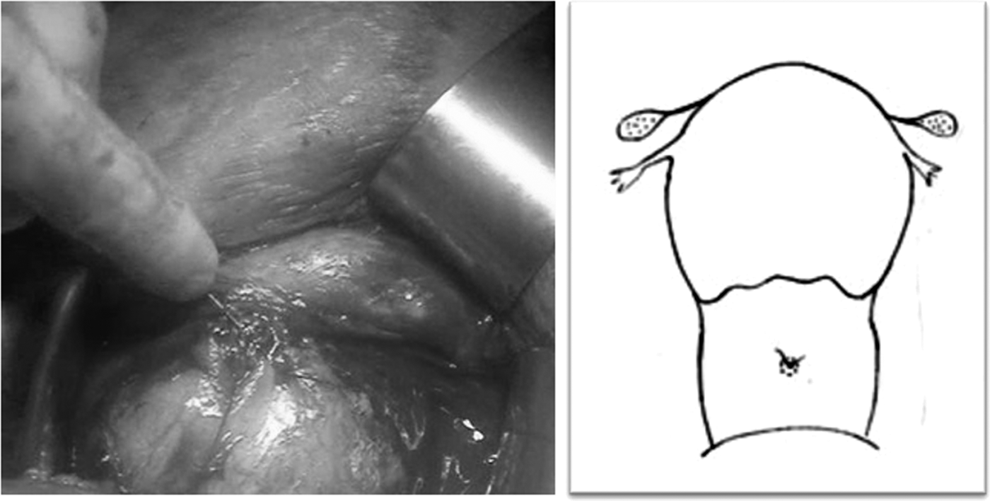
Suturing completed, endpoint is a point suture, compared to linear suture.
Following parameters were studied.
Preoperative data
1. Indications.
2. Gravida and parity of patients.
3. Elective or emergency LSCS.
Intraoperative course
1. Type of anesthesia.
2. Type of abdominal incision.
3. Uterine incision to baby delivery time (UIBD).
4. Baby delivery to uterine closure (BDUC) time.
5. Intraoperative complication.
6. Intraoperative blood loss.
7. Need of additional hemostatic suture.
8. Length of suture material used.
9. APGAR score.
10. Baby weight distribution.
Postoperative course
1. Postoperative complications.
2. Hospital stay.
Statistical analysis
Statistical analysis was performed using the SPSS software version 15. The independent sample t-test and chi square tests were used for comparison among different parameters. Data presented as frequencies, percentages, and mean±SD wherever required.
Results
Table 1 shows the age groupwise distribution of the patients in the two study groups. In total, 60 patients were included in the study. Group 1: The number of patients in the age group of 21–25 years was 22 (73.33%), in the age group of 26–30 years was 7 (23.33%), with a single (3.33%) patient of more than 31 years of age. Group 2: The number of patients in the age group of 21–25 years was 20 (66.7%) and in the age group of 26–30 years was 10 (33.3%).
Table 2 shows gravidawise distribution of patients in the two study groups. Group 1: 24 (80%) patients were primigravida, 5 (16.7%) were second gravida, with a single (3.3%) case of third gravida. Group 2: 24 (80%) patients were primigravida, 4 (13.3%) were second gravida, and 2 (6.7%) were third gravida.
Table 3 describes the different indications for which CS was performed in the two study groups. The number of patients with meconium-stained amniotic fluid (MSAF) was 11 (36.7%) in group 1 and 6 (20.0%) in group 2. In group 1 and group 2, the number of primigravida with breech was 5 (16.7%) and 10 (33.3%); the number of cephalopelvic disproportions (CPDs) was 4 (13.3%) and 8 (26.7%); the number of nonprogress of labor was 3 (10.0%) and 2 (6.7%); and the number of oligohydramnios with intrauterine growth restriction (IUGR) was 2 (6.7%) and 1 (3.3%), respectively, with one case of premature rupture of membranes (PROM) and postdatism in each group. Other indications in group 1 with one case of each include preterm PROM, pregnancy induced hypertension (PIH) with MSAF, and premium pregnancy; in group 2, one case of postdated premium pregnancy.
MSAF, meconium-stained amniotic fluid; PROM, premature rupture of membranes; IUGR, intrauterine growth restriction; PIH, pregnancy induced hypertension.
Table 4 shows situation of CSs performed either as emergency or as elective. Group 1: 29 (96.7%) were in emergency setting with 1 (3.3%) in elective setting. Group 2: 27 (90.0%) were in emergency setting and 3 (10.0%) were in elective setting.
Table 5 gives the comparative parameters in the two study groups. The data are presented as mean±SD. The UIBD in seconds is 18.7±2.95 in group 1 and 19.0±2.76 in group 2. This difference was not statistically significant (p=0.720). BDUC time in minutes is 9.6±1.74 in group 1 and 8.2±1.41 in group 2. The differences in BDUC time in the two study groups were statistically significant (p=0.001).
p-Value <0.05.
BDUC, baby delivery to uterine closure; UIBD, uterine incision to baby delivery time.
The blood loss during the procedure in group 1 was 872.6±41.26 mL; in group 2, it was 791.3±27.0 mL. The difference in blood loss was statistically significant in the two groups (p=0.000).
The length of suture material required for closure of the uterus was 127.57±5.49 cm in group 1 and 88.3±4.51 cm in group 2. The difference in length of suture material required in the two groups was statistically significant (p=0.000).
Table 6 depicts the intraoperative complications that occurred in the two study groups. Group 1: The only complication was uterine incision extension, which was present in 2 (6.66%) cases. Group 2: No complications occurred in any of the patient.
Table 7 shows the number of patients who required additional hemostatic suture in the two study groups. Group 1: 7/30 (23.3%) patients required additional hemostatic sutures. Group 2: 2/30 (6.7%) patients required additional hemostatic sutures.
p<0.05 is considered significant.
AHS, additional hemostatic suture.
Table 8 gives the newborn parameters like the APGAR score at 1 minute and mean body weight. In group 1, APGAR scores at 1 minute of 8, 9, and 10 were achieved in 14 (46.7%), 14 (46.7%), and 2 (6.6%), whereas in group 2, it was in 12 (40.0%), 17 (56.7%), and 1 (3.3%) newborns, respectively. Mean baby weight in kg was 2.73±0.50 in group 1 and 2.9±0.48 in group 2.
Table 9 gives the postoperative course of the patients. In postoperative complications, one case (3.3%) of each of rectus sheath hematoma, wound discharge, wound gape in group 1, with a single case (3.3%) of wound induration in group 2. Postoperatively, the total duration of hospital stay in group 1 was 5.97±2.67 days and in group 2 was 4.8±1.27 days. The difference in hospital stay was statistically significant in the two groups (p=0.035).
p<0.05.
Discussion
CS is one of the most commonly performed operations today. From times when childbirth was an event not necessitating medical attention to the present times where concerns are voiced about high cesarean rates, obstetrics has for sure travelled a long way. As medical science and especially obstetrics has evolved over the recent years, there has been a parallel and steady increase in the rates of cesarean births. According to a population-based cross-sectional study in Chennai, CS rates in the public and private sectors were 20% and 47%, respectively. The total population CS rate was 32.6% with a primary CS rate of 25%, which suggests that with the increasing cesarean rate in the private sector, the general rate of CS will rise substantially. 9
The techniques of CS have evolved much over the last few decades. Many variations in the technique of CS have been devised with the purpose of shortening the operating time, making the operation easier and more efficient, reducing costs, decreasing the risk of adverse effects, shortening postoperative morbidity, and duration of hospital stay. A variety of surgical techniques for all elements of the CS operation are in use. Surgical techniques involving the uterus at the time at CS may differ according to the type of uterine incision (lower transverse uterine incision vs. other types of uterine incision); methods of performing the uterine incision (sharp uterine entry vs. blunt uterine entry); suturing materials and techniques for the uterus at CS; and single- versus double-layer suturing for closing the uterine incision at CS. 8
Among the different incisions on uterus, the widely used one is the transverse lower segment uterine incision. The benefits offered are reduction in operative complications especially hemorrhage, easy repair reduction in morbidity, lower incidence of uterine dehiscence, or rupture in subsequent pregnancies. Other incisions like low vertical or classical are used rarely and recommended in certain clinical situations. 8
Incising the uterus with sharp incision gives rapid delivery of the baby, whereas blunt uterine entry reduces the blood loss and improves healing. Although the single-layer closure is associated with reduced operating time, less tissue disruption, and less introduction of foreign suture material into the wound, the double-layer closure improves hemostasis and wound healing and possibly a reduced risk of uterine rupture in a subsequent pregnancy. 8
Because a large number of women undergo CS, even small differences in postoperative morbidity rates could translate into improved health for a substantial number of women and significant savings to costs and resources of health services. Improvements in health by optimizing CS techniques are likely to be more significant in the developing countries, because the rates of postoperative morbidity in these countries tend to be higher. More women could therefore benefit from improvements in techniques.
We performed a comparative study between the standard LSCS (group 1) and the innovative COCS technique of uterine incision for CS (group 2).
In our study, all CSs performed were primary LSCS. In total, 60 patients were enrolled in the study with 30 in each group of the cesarean procedure. Patients in the age group of 21–25 years were 22 (73.3%) in group 1 (standard LSCS) and 20 (66.7%) in group 2 (COCS), with 8 (26.7%) patients above the age of 25 in group 1 and 10 (33.3%) in group 2.
Twenty-four (80%) of the patients were primigravida in both the groups, whereas second gravida were 5 (16.7%) and 4 (13.3%), with third gravida being 1 (3.3%) and 2 (6.7%) in group 1 and group 2, respectively. This is may be because of exclusion of previously scarred uterus.
Among the different indications for the CS, MSAF was most common and accounted for 11 (36.7%) cases in group 1 and 6 (20.0%) cases in group 2. Patients with indication of primigravida with breech presentation were 5 (16.7%) in group 1 and 10 (33.3%) in group 2. The other indications were with less frequency and include CPD, nonprogress of labor, oligohydramnios with IUGR, PROM, preterm PROM, PIH with MSAF, premium pregnancy, and postdated premium pregnancy in that order.
Fifty-six (93.3%) patients were operated in an emergency setting, whereas 4 (6.7%) were operated electively. Shamshad reported that 69% of cesarean section was performed in emergency, whereas 31% were in elective setting. 10 This suggests that the cesarean procedures are usual in emergency setting. The operative procedure was performed under spinal anesthesia in both groups. The type of abdominal incision was Pfannenstiel incision in all cases. The other type of incision for abdominal opening was the Joel-Cohen-based incision. It results in less blood loss and shorter opening time, but no benefit in terms of occurrence of wound infection, postoperative hematocrit level, return of bowel function, or time to mobilization. 2
The standard LSCS (group 1) was compared to the novel technique of COCS LSCS (group 2) on different parameters like time to baby delivery after uterine incision, time for closure of uterus after baby delivery, intraoperative blood loss, intraoperative complications, total length of suture material used, need of additional hemostatic suture, APGAR score, baby weight, postoperative complications, and days of hospital stay.
The time to baby delivery after uterine incision measured in seconds was 18.7±2.95 seconds in group 1 and 19.0±2.76 seconds in group 2 and the difference was not statistically significant (p=0.720), whereas time to uterine closure after baby delivery was less in the COCS group (8.2±1.41 minutes) than the LSCS group (9.6±1.74 minutes) and was statistically significant (p=0.001). This suggests that the innovative technique of COCS does not delay the baby delivery and requires less uterine closure time, which could be advantageous.
The mean intraoperative blood loss in group 1 was 872.6 mL and in group 2 was 791.3 mL and the difference was statistically significant in two groups (p=0.000). This suggests that the novel technique of uterine incision may have less bleeding complications intraoperatively.
In intraoperative complications, extension of the uterine incision occurred in two cases in the standard LSCS group, but not in the COCS group. This may result in decreased operative time, decreased blood loss, and need of blood transfusion.
The closure of uterine incision can be achieved by single-layer or double-layer closure. In our study, closure of the uterine incision was performed in double layers in both groups. There has been variable interest on the use of one particular method for closure of uterine incision. Some have suggested that the single-layer closure is as good as the double-layer closure with advantages of reduced operating time, less tissue disruption, less introduction of foreign suture material into the wound, febrile morbidity, endomyometritis, and hospitalization period.11,12 The Cochrane review on surgical techniques in uterine incision observed one study which suggested that single-layer closure of the lower uterine segment at CS is associated with a fourfold increase in the risk of uterine rupture in a subsequent pregnancy, when compared with the double-layer uterine closure. 8 Nancy O'Brien-Abel suggested that surgeons consider using the double-layer closure technique for women who may subsequently experience a trial of labor. 13 This is consistent with our study, in that most of the patients were primigravida and are likely to experience trial of labor in their subsequent pregnancy. Moreover, the outcome of this innovative technique has not been evaluated before. Thus, the double-layer closure of uterine incision seems appropriate and was performed in all the patients.
The closure of uterine incision was achieved with synthetic delayed absorbable sutures. This suture material has good relative tensile strength, low tissue reactivity, and best handling and is suggested for use in closure of well-vascularized uterus. 14 The mean length of suture material required for uterine incision closure in group 1 was 127.5 cm, compared to 88.3 cm in group 2. The difference in length of suture material used was statistically significant in the two groups (p=0.000). This could possibly be because of the concentric (purse-string suture) with near pinpoint closure of incision involved in the COCS procedure. Less suture material use may be associated with less tissue disruption, better healing, and less cost. In one such study, the average length of suture material required for complete closure in a continuous suture line single-suture closure technique was 160 cm, compared to 440 cm in the standard CS. 15
The number of cases that required extra sutures to achieve hemostasis was 7 (23.3%) in group 1 and 2 (6.7%) in group 2. There was no statistically significant difference between the two groups with regard to the requirement of additional hemostatic suture during the procedure (p=0.071). The use of additional suture material could result in more blood loss, increased operative time, and more suture material. Uterine incision extension was noted in 2 (6.67%) cases in group 1, but not in a single case in group 2. This probably suggests that this new technique provides enough space for baby delivery and may reduce complication of extensions.
The complications that occur postoperatively after CS include infections, including endomyometritis, wound infection, urinary tract and bronchopulmonary infections, anemia, thromboembolism, and death. 16 In the postoperative period, complications were not frequent in any of the groups. The complication noted was rectus sheath hematoma, which required exploratory laparotomy, abdominal wound gape and discharge occurred in one patient each in group 1, whereas wound induration in one patient occurred in group 2. This may not be related to the operative technique used and could possibly be explained by many factors such as indications for CS, postoperative care, nutritional status of the patient, and use of antibiotics.17,18
The total duration of hospital stay was 6±2 days in group 1 and 5±1 day in group 2. This difference was statistically significant in the two groups (p=0.035). Thus, this new technique of CS could help in early mobilization and possibly reduce the healthcare facility cost.
A newborn's assessment at birth was done with the help of APGAR score. The total scores in both the groups were equal or above eight in all the babies. This may suggest that the new technique of CS has no deleterious effect on the health outcome of the newborn. The mean baby weight was 2.73±0.50 in group 1 and 2.9±0.48 in group 2.
The quest on the part of obstetricians to improve upon the surgical methodology of CS has led to many modifications that have evolved over the past. Of such modifications, one was the Vejnovic modification, which involved shortening the uterine suture so that the subsequent scar is small. This modification was associated with shorter time, less use of suture material, less blood loss, lesser complications, and shorter hospital stay. 19 In COCS, wound closure is nearly pinpoint, which may result in a small scar, compared to standard LSCS and this could probably have benefited in terms of various parameters studied. 8
A question that could be raised about the innovative technique is how to perform a repeat delivery after this. Since 24 (80%) of the patients were primigravida in the COCS group, they are expected to have a second pregnancy and deliver either vaginally or by repeat cesarean. Vaginal birth after a previous cesarean (VBAC) has been debated. The risk of uterine rupture and adverse neonatal outcome are feared with VBAC. 20
Measurement of thickness of lower uterine segment may help in predicting the dehiscence during subsequent trial of labor. If the thickness of lower segment is more than 1.6 mm, the possibility of dehiscence is very small. 21 Berube L. et al. reported that labor at the time of previous CS and use of synthetic sutures for closure were associated with a thick lower uterine segment in a subsequent pregnancy. 22
This comparative study describes the innovative technique of COCS of uterus at CS. The use of this technique involves fewer complications, less use of suture material, and could benefit the patients in terms of morbidity. It also has no deleterious effect on the immediate health of a newborn. This novel technique could possibly have the lower risk of uterine dehiscence in a future pregnancy since the resulting scar is small. It may also decrease the possibility of morbid adherent placenta.
Our study did not find the long-term outcome of this technique, which needs to be evaluated. Also, the outcome in the subsequent pregnancy needs to be studied, which was not performed in the study. Comparison of this technique in a large randomized controlled trial to estimate its potential benefit is desired.
Conclusion
From this study, we conclude that the COCS technique of CS is feasible.
The said technique “COCS in CS,” was conceptualized and executed in 2007 at a tertiary referral hospital, Mumbai, India. The technical minutes with photograph and videos were presented at various local-, state-, and national-level scientific sessions and conferences and won prizes. Protocol was made and submitted to the institutional review board (IRB) and ethics committee for approval.
The dissertation topic was given to a postgraduate student of the 2009–2012 batch, Maharashtra University of Health Sciences (MUHS), India. This dissertation was complete and accepted by the MUHS University. The said technique is in practice since then. Till date, more than 300 cases have been done.
The time required for uterine closure, length of suture material required, intraoperative blood loss, intraoperative complications like extension are less in this technique, compared to the standard LSCS.
There are certain merits of this procedure like less operative time, less amount of suture material required, less need of extra hemostatic sutures, less chances of extension of uterine incision, less chances of dog ear formation while suturing.
This may lead to better scar healing and less chances of uterine rupture in subsequent pregnancy. Also, the chances of morbid adherent placenta in future pregnancy are less due to pinpoint uterine scar. There are no established demerits of this technique. Subsequent behavior of the scar needs to be studied in future pregnancies.
Footnotes
Acknowledgment
The authors acknowledge their institution, LTMGH–Sion Hospital, Mumbai, where the study was done.
Disclosure Statement
No competing financial interests exist.