
Abstract
Abstract
Introduction
I
The use of ultrasonography at the time of intrauterine surgery provides visualization of the exact location of the endoscopic instruments within the uterine cavity and allows visualization of the myometrium. The close communication between the hysteroscopist and the sonographer provides precise continuous monitoring of the hysteroscopic procedure, allowing completion with safety. Scanlan et al. stated, in 2001, that ultrasonography guidance is helpful for avoiding laparoscopy, which is more expensive. 1 As a noninvasive procedure, intraoperative imaging may preclude the need for simultaneous laparoscopy.2,3 Moreover, ultrasonography guidance was concluded to be even superior to laparoscopic guidance during hysteroscopic resection of intrauterine synechia and septa. Although no complications related specifically to the laparoscopic procedures were found in one study, the researchers stated that the potential for these complications is much higher than the potential for ultrasound-related risks. 4
The availability of a wide range of ultrasound transducers, provides great flexibility in the routes of intraoperative ultrasound guidance, with being transabdominal, transvaginal, or transrectal options. 1 Transrectal, ultrasound, intraoperative hysteroscopic guidance was described by Fleischer et al., 5 in 1990. Despite providing accurate details of the cervix and uterus, the transrectal route did not achieve the expected popularity in practical intraoperative use, requiring the sonographer to stand alongside the hysteroscopist in a relatively small working space with the patient in the dorsal lithotomy position. 1
The spreading of intraoperative ultrasound as a guide for endoscopic procedures, and searching for more-precise techniques and better image clarity, necessitates the use of three-dimensional (3-D) ultrasound. In 2010, intraoperative 3-D ultrasound was described as a novel technique for monitoring hysteroscopic metroplasty using both transabdominal and transvaginal routes. 6
Given that transabdominal ultrasound is not the standard for scanning the pelvic structures—and at the same time, the transvaginal route puts tremendous pressure on the hysteroscopist to remove and reinsert the hysteroscope repeatedly, with subsequent uterine refilling—the efficacy of transrectal 3-D ultrasound guidance for hysteroscopic metroplasty needs to be evaluated.
Materials and Methods
The aim of this study was to evaluate the efficacy of transrectal 3-D ultrasound as a tool of intraoperative guidance for hysteroscopic metroplasty.
Study design
A pilot, prospective, randomized comparative study (Canadian Task Force classification I), was performed at the Shatby Maternity University Hospital (a tertiary-level hospital), in Alexandria, Egypt. The study included 60 patients who had excessive menstrual loss, recurrent miscarriage, or infertility, and who diagnosed with septate uterus via hysterosalpingogram (HSG) and that was confirmed later via transvaginal 3-D ultrasound. All cases with the following criteria or findings were excluded from the study: during menstrual or abnormal bleeding; active cervical or uterine infection; or suspected cervical malignancy.
A septate uterus was diagnosed on 3-D transvaginal sonography (TVS) findings when a septum dividing the endometrial cavity was noted on the coronal plane with the external uterine surface was either normal or showed a sagittal notch of <1 cm. The septate uterus was classified as complete or incomplete (subseptate) according to the extent of the septum from the fundus to the external os. In addition, all patients had an HSG to show the size and extent of the septa and to be used for comparison with postoperative HSG that was performed 3 months later.
Procedures
The patients were randomized preoperatively, using a computer-generated randomization sheet, into two groups of 30 patients each. Allocation to any group was concealed in an opaque envelope, which was opened at the time of each operation.
Group A hysteroscopic metroplasty was performed under transrectal, 3-D ultrasound guidance using a real-time Sono Ace x8 (Samsung Medison Co., Ltd. Korean) device, equipped with a 3-D multifrquency 5–9 MHz endovaginal transducer. This procedure was performed by the same radiologist. In Group B, hysteroscopic metroplasty was performed without any ultrasound guidance.
Spinal anesthesia was given to all patients. Metroplasty was scheduled in the early proliferative phase, without pharmacologic preparation. All patients were operated by the same hysteroscopist and scanned intraoperatively by the same sonographer.
A 26 F resectoscope, fitted with a monopolar knife electrode and a 0° telescope was used. The uterine cavity was distended with 1.5% glycine at a constant inflow pressure. A Hamou Hysteromat was used to ensure an intrauterine pressure of 35–40 mmHg, with a flow rate of 150 mL/minute. All of this equipment was manufactured by Karl Storz GmbH (Tuttlingen, Germany).
The fluid deficit was recorded by measuring the difference between the infused and drained fluids. The outflow port of the resectoscope and the drained fluid from the vagina were collected in a plastic graduated container, so little fluid was lost in the drapes. In each patient, the septum was incised starting from its lower margin, and proceeding forward with progressive horizontal incisions.
In group A, intermittent transrectal 3-D ultrasound was performed, by the same radiologist, in three stages: (1) preoperatively to measure the septum length, associated fundal indentation (if any), and septum–myometrium interface (Fig. 1); (2) during metroplasty to specify the presence of any residual, and to determine its length and site (at this moment, because of the distending media filling the uterine cavity, the obtained images are actually 3-D sonohysterography images [3-D-SIS]); and (3) at the end of the procedure to ensure completeness with safety. In group B, no intraoperative ultrasound guidance was used, and the procedure was ended depending on the surgeon's experience in recognizing myometrial muscle fibers and blood vessels.
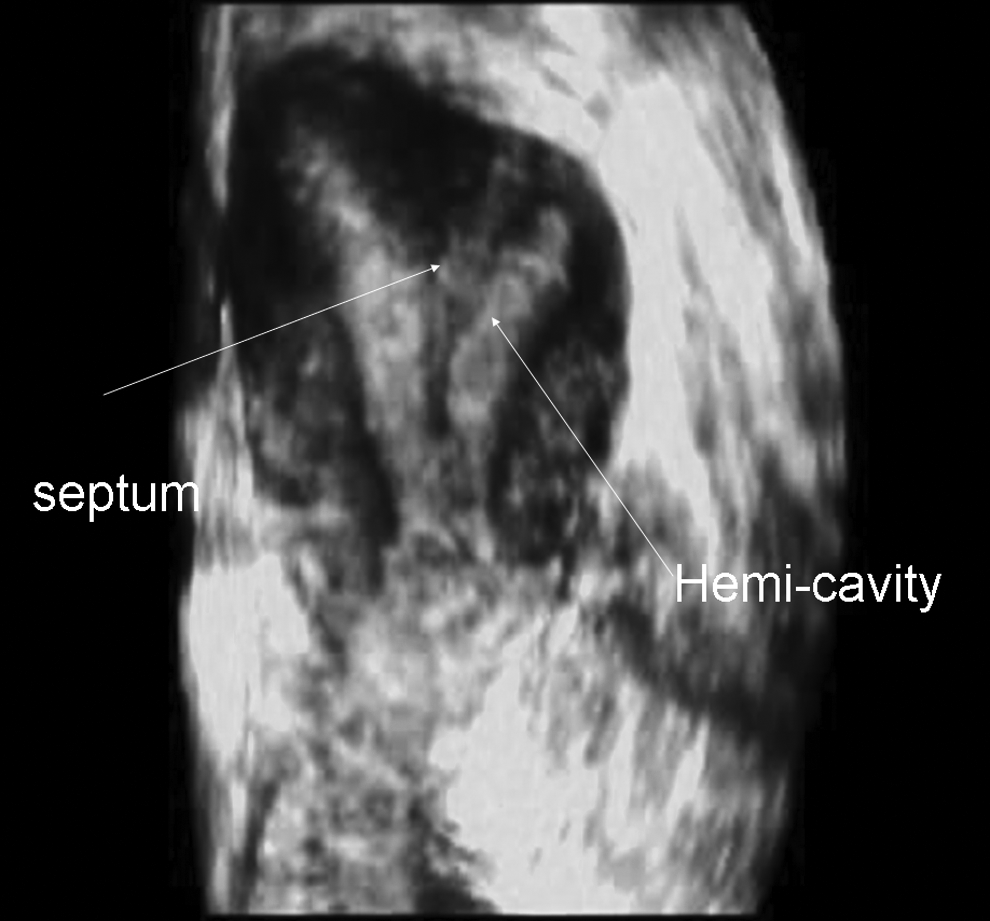
Preoperative, three-dimensional transrectal image of a patient's septate uterus (no fundal indentation).
A single-dose intraoperative intravenous antibiotic was given to each patient, according to the hospital protocol. All patients were discharged to go home on the same day. Operative data, including operative time, fluid deficit, and complications (e.g., fluid overload, bleeding, incomplete resection, or perforation) were recorded.
Each patient had postoperative HSG 3 months later, after exclusion of pregnancy to evaluate complete resection of the septum objectively. The fear of misdiagnosis of bicornuate uterus as being septate was obviated by the preoperative workup and 3-D ultrasound performed intraoperatively. Thus, what is needed postoperatively is to exclude the presence of any residual septum via HSG, which can provide this data accurately.
Statistics
Data were fed to the computer using Predictive Analytics Software (PASW Statistic 18). The distributions of quantitative variables were tested for normality using a Kolmogorov-Smirnov test and a Shapiro-Wilk test. A D'Agstino test was used if there was a conflict between the two previous tests. Quantitative data were described using range, mean, and standard deviation. Associations between categorical variables was tested using the Chi-square test. Significance test results were quoted as two-tailed probabilities. Significance of the obtained results was judged at the 5% level.
Results
In groups A and B, respectively, the patients' ages ranged 20–40 and 18–40, with means of 28.12±6.65 and 26.5±5.75. There was no significant statistical difference between the two groups regarding age (p=0.21).
In groups A and B, respectively, parity ranged from 0–1 and 0–2, with means of 0.74±0.21 and 0.92±0.44 and no significant statistical difference.
With respect to type of septum (incomplete or complete), group A included 17 patients (56.7%) with incomplete septa, compared to 16 patients (53.3%) in group B, with no significant statistical difference between the groups. In addition, group A included 13 patients (43.3%) with complete septa, compared to 14 patients (46.7%) in group B; with no significant statistical difference between the groups.
On comparing the operative time between the two groups as shown in Table 1, group A had a statistically significant longer operative time than group B (p=0.001). With respect to fluid deficits, they ranged between 290 mL and 350 mL with a mean of 325±22.9 in group A and between 270 mL and 320 mL, with a mean of 298.6±19.85 in group B, with no significant statistical difference between the two groups.
SD, standard deviation; min, minutes; t, value of the t-test.
Denotes statistical significance.
On comparing the complication rate, 1 patient (3.3%) in group A had an incomplete perforation (overcorrection), while 1 patient (3.3%) in group B had a uterine perforation, with no statistical difference between the groups.
After 3 months HSG was performed in all patients (with no dropouts), after excluding pregnancy to detect the presence of any residual septa objectively. A statistically significant higher incidence of uterine septa residuals was found in group B (p<0.05) as shown in Table 2.
Denotes statistical significance.
During the procedure on 1 patient in group A (who had a broad-based septum with a fundal indentation of <1 cm), intermittent use of 3-D transrectal sonohysterography identified the presence of missed residual parts of the septum at the lateral ends near the corneal openings with lengths ranging from 5 mm to 10 mm (Figs. 2 and 3). Complete resection of these missed parts was achieved precisely and safely under transrectal 3-D sonohysterography guidance (Fig. 4).
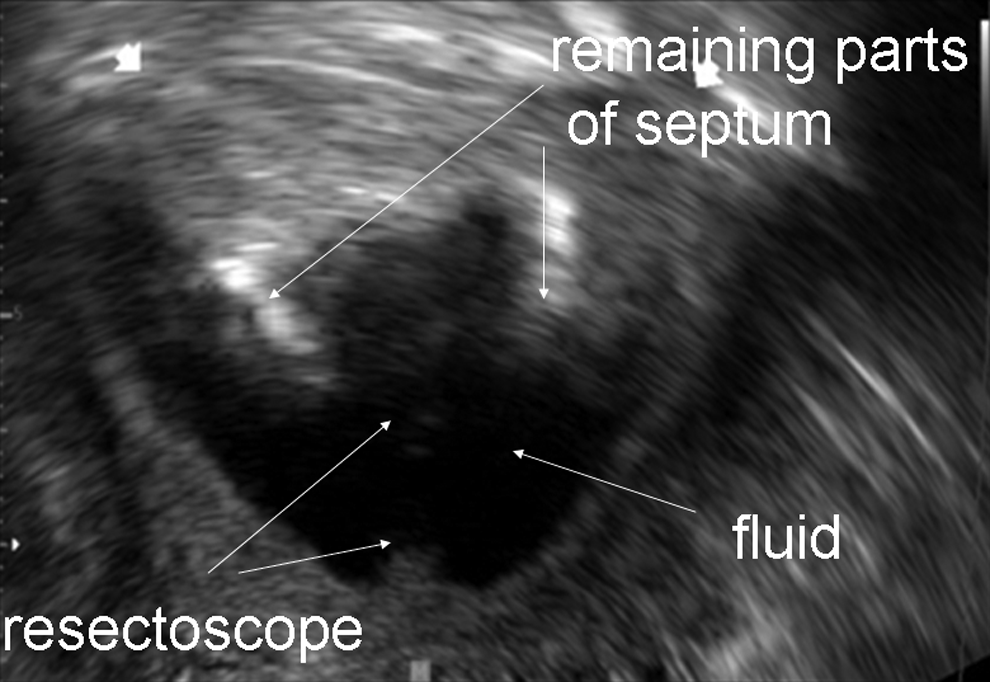
An intraoperative, three-dimensional, sonohysterographic transrectal image showing remaining parts of the septum at the lateral two ends of the septum in another patient.
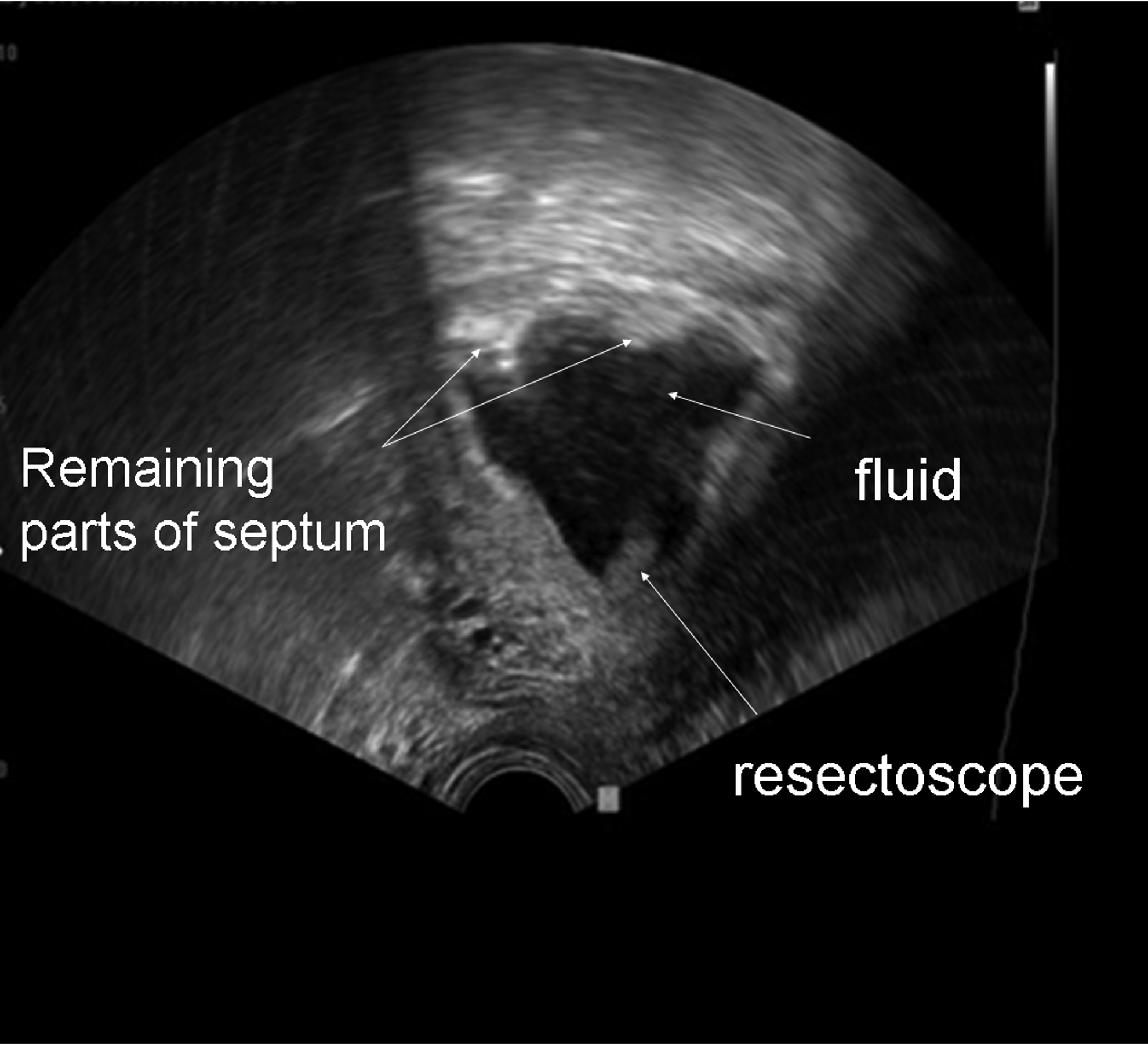
An intermittent, intraoperative, three-dimensional, sonohysterographic transrectal image of the same procedure showing fewer remaining parts of the septum in the same patient.
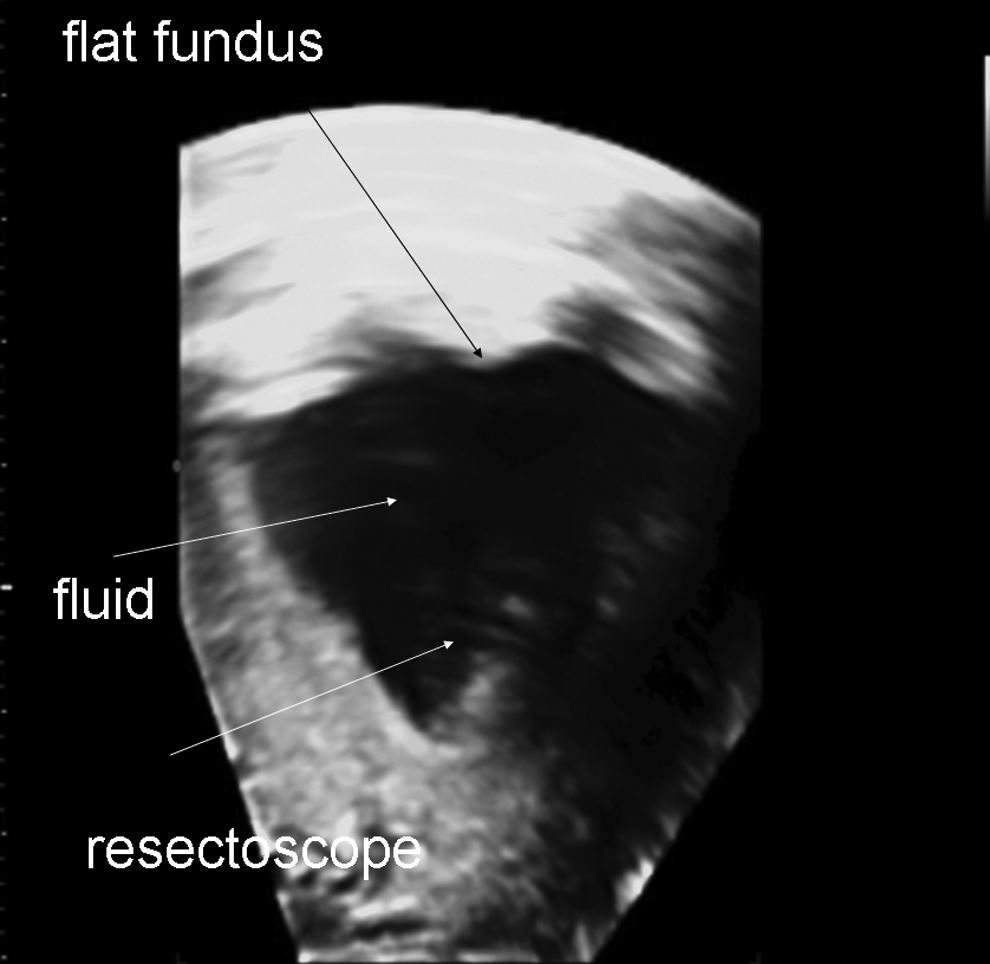
Three-dimensional sonohysterography at the end of the procedure in the same patient, showing a flat fundus and distended uterine cavity with the resectoscope still in situ.
During metroplasty on another patient in group A (with a short broad septum and fundal indentation ∼5 mm), the sonographer identified a central overcorrection and the start of myometrial injury (incomplete perforation), and recommended stopping the procedure. The patient's postoperative HSG showed an incomplete perforation of 3 mm deep.
Discussion
HSG is considered to have high sensitivity (60%–98%), but low specificity. 7 HSG showed a sensitivity of 81.2%, compared with hysteroscopy, and a specificity of 80.4% with a positive predictive value of 63.4% and a negative predictive value of 83.7%. HSG had a false–negative rate of 90% and a false–positive rate of 21.8%. Overall agreement between the two procedures was 73%. 8 In order to describe a uterine anomaly, it is necessary to visualize both the uterine fundus and serosal outline in the coronal plane. Although the conventional sagittal and transverse images of the uterus, as provided by two-dimensional (2-D) technologies, are still important; the coronal plane is rarely obtained on 2-D scans. This plane can be visualized easily by using the section reconstruction method of a 3-D volume.9–11
The most critical part during hysteroscopic metroplasty is deciding when to stop the incision. A wrong decision can lead to either residual septa with possible need for further intervention 12 or the procedure can end with a perforation that carries the possible risk of uterine rupture in a subsequent pregnancy.13–16
Real-time ultrasound guidance of hysteroscopic procedures has evaluated in different studies,3,4,17–19 but the routes of imaging varied among transvaginal, transabdominal, and even laparoscopic ultrasound probe usage. In a study conducted by Guerrero et al. 6 on 20 patients, 3-D ultrasound guidance of hysteroscopic metroplasty was through the transabdominal and transvaginal routes. The researchers concluded that both transabdominal and transvaginal routes can be used successfully to guide the procedure. In another more-recent study, 19 the transvaginal route was also used and the researchers concluded that intraoperative 3-D transvaginal ultrasound reduced the incidence of suboptimal (>5 mm) septal resections during hysteroscopic metroplasty.
In contrast to the current study, in which the trans-rectal route was adopted, there is no doubt that the transvaginal route well-delineates the pelvic organs. However, it causes technical difficulties, as the resectoscope should be withdrawn completely to allow introduction of the ultrasound vaginal probe, with a loss of uterine distension (losing the advantage of a sonohysterography) and a need for more time and fluid for uterine refilling.
The core of the current study was based on the use of intermittent transrectal 3-D ultrasonography. It provided detailed imaging of the uterine cavity, septum, and myometrium. In addition, because this guidance was performed on a distended uterine cavity, 3-D sonohysterographic images were obtained. The simultaneous application of the resectoscope and the ultrasound probe gave the surgeon the chance to operate freely while the sonographer was able to obtain images. With the resectoscope in place and the uterine cavity distended with glycine, the ultrasound images were detailed 3-D sonohysterography scans, with decreases in the amount of fluid media used and total duration of the procedure.
In the current study, the operative time in the transrectal 3-D ultrasound-guided group was statistically longer than in the nonguided group. In spite of overcoming the extra time needed when using a transvaginal route (to remove the resectoscope, apply the vaginal probe, obtain the needed images, withdraw probe, reapply the resectoscope, and redistend the uterine cavity), the procedure still needs more time. The extra time is necessary so that the sonographer is able to provide accurate data on the length and thickness of the septum, shape of the fundus, and size of the hemicavities, in addition to the ultrasound repetition needed in some cases until confirmation of complete septum excision is achieved. The coordination time between the surgeon and sonographer became shorter (from the experience gained) near the end of the study; this was reflected in the operative times ranging from 46 minutes at the start of the study and reaching <30 minutes near the end of the study. An important fact to be considered is that interference on the ultrasound screen was observed when electrosurgery was used, necessitating halting the procedure while the images were obtained and leaving the resectoscope in situ.
In the current study, the postoperative HSG confirmed complete septum resection without any residual in all cases (except for 1 case with incomplete perforation) in group A, while in group B, 6.5 % had residual septa (5–9 mm) and 6.5% had residual septa >1 cm, with statistically significant difference (p<0.05). In the 3-D ultrasound-guided group, on objective criteria were used when deciding to stop the incision; this information was obtained by viewing the 3-D reconstructed coronal view of the flat uterine fundus, the triangular cavity, and the residual septum length=0 mm. In the nonguided group, halting the resection depended on observation of muscle fibers and myometrial blood vessels (which can vary in recognition according to the surgeon's experience).
This is similar to the results of another recent study 19 using the 3-D real-time imaging during metroplasty. That study was conducted with 19 patients, in which residual septa >5mm was 0% versus 26% (in 3-D ultrasound-guided and nonguided groups, respectively) with p=0.04; and residual septa>10 mm was 0% in the guided group versus 10.5% in the nonguided group, with p=0.48. However, the study differered from the present study in the route of 3-D ultrasound guidance, which was transvaginal, and in the 3 months postoperative follow-up, which was by 3-D ultrasound, which remains operator-dependent in contrast to HSG.
Another advantage of the current study was the selection of transrectal route. The application of the probe transrectally allowed the images to be obtained while the resectoscope was still in situ with the uterine cavity distended by the media, and this led to the acquisition of 3-D sonohysterographic images. Some researchers have suggested that 3-D sonohysterography might be superior to 2-D sonohysterography. 20 In a more-recent study, 21 3-D SIS was compared to 3-D ultrasound and 2-D SIS in the accuracy of diagnosing and differentiating between congenital uterine anomalies. 3-D SIS was the only ultrasound method that produced findings that were completely consistent with combined hysteroscopy and laparoscopy. The researchers also stated that 3-D SIS can also be regarded as an optimal test, which can also be applied in doubtful cases as a reference method instead of using combined hysteroscopy and laparoscopy. 21
The presence of a residual septum and its impact on reproductive outcome became debatable. Many studies demonstrated that septa remnants of <1 cm may not worsen the reproductive outcome, until Fedele et al. 22 proposed better pregnancy outcome in patients with no residual septa, compared to those with residual septa <1 cm, and suggested that a septal endometrium is unsuitable for implantation of the blastocyst, independent of the extent of the uterine abnormality. However, these researchers failed to show a statistically significant difference in their study. Thus, they concluded that the presence of residual uterine septa of (0.5–1 cm) appears not to worsen the reproductive prognosis, compared with that in women in whom the septum has been completely or almost completely corrected. In contrast to another study, 12 the researchers stated that women with remnant septa ≤1 cm have an increased chance of successful pregnancy after normalization of the uterine cavity.
Conclusions
All data obtained by transrectal 3-D ultrasound at the end of the procedures in the current study were exactly the same as those obtained by postoperative HSG. Thus, it could be concluded that adopting this technique during hysteroscopic metroplasty removes the need for postoperative HSG. This conclusion differs from that of Kucera, 23 in a study that investigated if there was any correlation between residual septa and pregnancy outcomes, through calculation of a uterine index from postoperative HSG. This researcher found that a ratio >10% correlates with a higher incidence of spontaneous abortion, making postoperative HSG necessary, especially in difficult cases.
The points to be considered if standardizing 3-D ultrasound guidance during hysteroscopic metroplasty in the routine practice is proposed, aiming to achieve the safe precise complete septum removal, are (1) the availability of the 3-D ultrasound apparatus in the minimal invasive surgical department and (2) the presence of a well-trained sonographer coordinating with the surgeon to reach the desired optimum outcome.
Footnotes
Acknowledgments
The authors sincerely appreciate the efforts, technical assistance, and keen work made by Al-Radwan Co., and Samsung Medison Co., in Egypt, in providing the ultrasound system apparatus in our minimal invasive surgery unit.
Disclosure Statement
The authors have no conflict of interest.