
Abstract
Abstract
Introduction
P
Over the past few decades, continual and significant improvements in operative techniques, anaesthesia, critical care, and patient selection have decreased the associated mortality and complication rates of this procedure.2–5 Recent articles in the literature have also provided evidence of long-term survival in selected patients who underwent pelvic exenteration.6,7
In gynecologic cancers, in the absence of metastatic disease, pelvic exenteration—with curative intent—can be performed in selected patients with locally advanced primary or recurrent malignancies.8,9 The aim of this study was to describe the current authors' experience of performing pelvic exenteration in patients with locally advanced primary and recurrent gynecologic malignancies.
Materials and Methods
A retrospective review of all patients who underwent pelvic exenteration for gynecologic malignancies from January 1982 to March 2011 was performed. These patients were identified from prospectively collected databases of patients with gynecologic cancers and patients who underwent pelvic exenteration. The study protocol was reviewed and approved by the current authors' institutional ethics committee.
It is the current authors' present-day practice to discuss all patients with advanced pelvic malignancy who are considered for a possible pelvic exenteration procedure in a multidisciplinary tumor board meeting comprising surgical, medical, and radiation oncologists. Each patient with advanced pelvic malignancy would have undergone a computed tomographic (CT) and/or a magnetic resonance imaging (MRI) scan of the pelvis and a positron emission tomographic (PET) or a PET-CT scan as part of the preoperative assessment to delineate the extent of the local disease and to exclude distant disease. If a patient with locally advanced or recurrent gynecologic cancer is deemed suitable to undergo a pelvic exenteration, it would be performed by a dedicated exenteration team comprised of colorectal surgeons and gynecologic oncology surgeons, and, in certain cases, urologists and plastic surgeons.
It is often difficult to confirm the extent of resection needed preoperatively because of the poor definition of margins. As described in the current authors' earlier articles, a total pelvic exenteration encompassed removal of the cancer with all the pelvic viscera in four described anatomical compartments, namely the (1) anterior, (2) central, (3) lateral and (4) posterior compartments. 10 A near-total pelvic exenteration was defined as the en bloc resection of the malignancy together with structures in up to three of these anatomical compartments.
Data collected included patient demographics, types of gynecologic cancer, and details of operative procedures and postoperative complications. The histopathologic reports of the specimens were also documented. An R0 margin is defined as a microscopically clear margin, R1 represents microscopically involved margins, and R2 represents macroscopically involved margins. Recurrence and survival data were retrieved from hospital medical records and a statewide births and deaths registry. Patients data were also analyzed by the decade when the surgery occurred. The duration of follow-up was measured from the date of discharge to the date of last follow-up or death.
Statistical analysis was performed using the SPSS 21.0 statistical package (Chicago, IL). The level of significance for all tests was set to p<0.05. Categorical data were analyzed using a Chi-square test and Fisher's exact test, when these were appropriate. Continuous data that were normally distributed were analyzed using an independent t-test, while those with skewed distributions were analyzed using appropriate nonparametric tests (Mann-Whitney–U). The overall survival probability was estimated according to the Kaplan-Meier method. All survival rates were based on overall survival; defined as survival regardless of the cause of death.
Results
Fifty-nine patients with locally advanced primary or recurrent gynecologic malignancies underwent pelvic exenteration during the study period. The mean age of the study group was 54 (standard deviation: 13.5 years). Ovarian, cervical, vulvar and endometrial cancers were seen in 27 (45.8%), 17 (28.8%), 7 (11.9%), and 6 (10.2%) patients, respectively. One patient had vaginal leiomyosarcoma and another patient had a malignant mixed Müllerian tumor. Adenocarcinoma (n=31, 52.5%) and squamous-cell carcinoma (n=20, 33.9%) were the most common histology types seen, while sarcoma was seen in 3 patients. The histologic subtypes of 5 patients could not be documented because of destruction of their records.
Twenty-one patients were operated on for locally advanced primary malignancy while 30 patients were operated on for recurrent disease. The presentation was not known for 8 patients because of destruction of their records. Interestingly, the proportion of the patients (21/30) who were operated on between 2001 and 2011 was for recurrent disease, compared to mainly primary presentation (14/21) between 1982 and 2000. This observation was statistically significant (p=0.01). Details of demographic characteristics of the study group are presented in Table 1.
Twenty-four (40.7%) patients underwent total pelvic exenteration and 35 (59.3%) patients underwent near-total pelvic exenteration. A urinary conduit was created in 16 (27.1%) patients (ileal: 14; colonic: 2), while a myocutaneous flap was created in 9 (15.3%) patients (vertical rectus abdominis muscle: 6; gracilis: 3). The median length of stay was 18 days. Table 2 shows the operative details and postprocedural outcomes.
Although there was no inpatient mortality, 26 (44.1%) patients developed perioperative complications of varying severity. Ten patients (38.5%) had urologic complications for which 8 patients required further operations for ureteric obstruction; 4 patients needed long-term indwelling catheters for voiding dysfunction; and 1 patient had a long-term suprapubic catheter. Notably, 1 patient required surgical intervention for a significant postoperative hemorrhage arising from a slipped ligature of an artery. Haemostasis was achieved intraoperatively and the patient recovered well. There were also 3 patients with intra-abdominal abscesses that required radiologically guided drainage.
Oncologically, 29 (49.2%) patients had an R0 resection, 14 (23.7%) had R1 margins, and 8 (13.6%) had macroscopically positive margins. There were 8 patients with missing data because of destruction of their patient records.
Over a median-follow up period of 144 months (range: 13–364 months), 41 patients died (70%). The overall median survival was 48.0 (12.7) months (Fig. 1). The 2-year and 5-year survival rates were 70.2% (6.1) and 41.6% (6.8), respectively. The 5-year survival rate for patients who underwent near-total exenteration was 51.6%, compared to 27.3% for patients who underwent total exenteration (p=ns; Fig. 2). The 5-year survival rates for ovarian, cervical, vulvar, and endometrial cancers were 36.6%, 29.4%, 53.6%, and 83.3%, respectively.
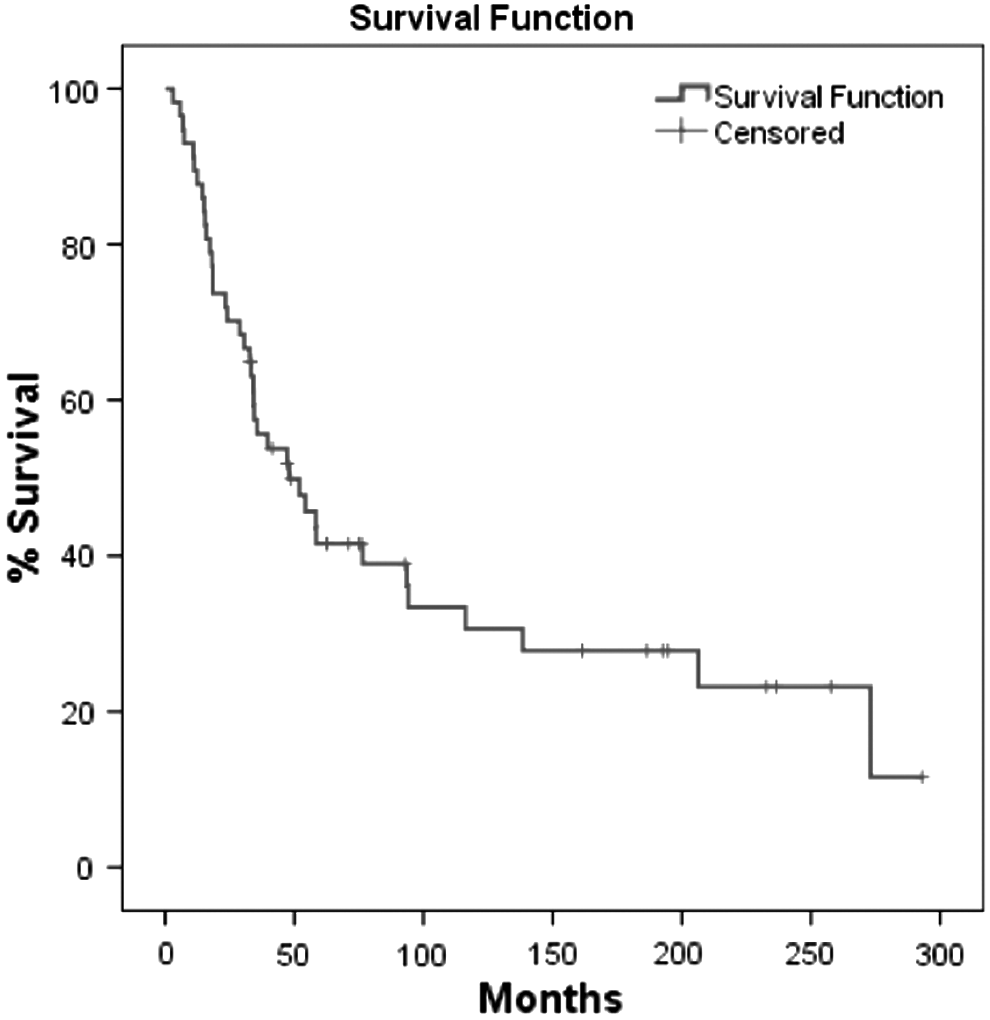
Overall survival of the study group.

Survival in patients with partial and total exenteration.
Discussion
Over the past few decades, pelvic exenteration has been increasingly adopted for patients with advanced or recurrent gynecologic malignancies.2–5 Five-year survival rates ranging from 30% to 60% have been achieved. The current series supports the increasing literature regarding the role of pelvic exenteration for selected patients with locally advanced primary or recurrent gynecologic malignancies, with a 5-year survival rate of 41.6% reported. The current authors postulated that the lower 5-year survival rates in the patients who underwent total exenteration was likely to be caused by the greater underlying pathology that necessitated total exenteration than the technique per se.
Exenteration is a serious undertaking, and the morbidity rate of 44% in the current series affirms the numerous possible complications faced by these patients and the surgeons.2,4–6,8,9,11–28 Fortunately, the continual improvements in operative techniques and critical care ensured no patient in the current series died as a direct consequence of the operation. While urologic complications are commonly seen in these patients, a better understanding of the operation and its progress has enabled the creation of guidelines for the early detection and management of the thorny problem of conduit leak, typically at the uretero–intestinal anastomosis. 10 Although a myocutaneous flap may be necessary in certain situations to cover the perineal defect, complications such as flap necrosis are not seen infrequently.
It is imperative to have a close working relationship with the plastic surgeons involved to choose the correct patients for this procedure. Some of the recommendations for a myocutaneous flap include two of the following factors: the presence of previous radiotherapy; previous abdomino–perineal resection; need for total exenteration; and need for sacrectomy. 29
In light of the associated morbidities, the aim of any exenterative surgery must be to attempt to achieve a R0 margin. Previously, total hysterectomy with possible proctectomy and/or cystectomy was perhaps the limit of resection in patients with locally advanced gynecologic malignancies. Patients with bony involvement were deemed to be inoperable. This no longer holds true. In carefully selected patients, sacrectomy to obtain a wider posterior margin, dissection of the lateral compartment to achieve wider lateral margins, and even resection of the pubic bone anteriorly can be performed safely to achieve an R0 margin.30,31 Using data from pelvic exenteration for rectal cancers, an R0 rate of >50% can be achieved in selected patients with disease involve the lateral compartment or sacrum. However, as we continue to adopt more-aggressive approaches to treating patients with locally advanced pelvic malignancies, the impact on their quality of life (QoL) must be taken into account. The current authors' institution previously demonstrated acceptable long-term QoL in patients who underwent pelvic exenteration for rectal cancers. 32
As seen in the current series, the 5-year survival rates varied from 28% to 83% for ovarian, cervical, vulvar, and endometrial cancers. These statistics are consistent with those published in the literature.2,4–6,8,9,11–28 Patients with recurrent cervical and vaginal cancers after maximal radiation therapy are suitable candidates for pelvic exenterative surgery. Careful patient selection, meticulous operative technique, and intensive postoperative management remain the cornerstones for maximizing the success of such surgery.2–6 There is still ongoing controversy with regard to the performance of pelvic exenterative surgery for recurrent endometrial cancer, because this disease tends to recur outside the pelvic radiation field. The current study, however, demonstrated a 5-year survival rate of 83.3% in 6 patients, which may support the indication of pelvic exenteration in a small carefully selected group of patients with endometrial cancers.
As with any operative technique, a learning curve is evident. With respect to pelvic exenteration, minimal data on this technique are available as this remains a very technically challenging procedure that should perhaps be performed only in specialized units. It would not be surprising to note that the majority of the patients that the current authors operated from 2001 to 2011 were for recurrent disease. This observation is not surprising, as surgeons are likely venture into more technically challenging cases when the surgeons are more comfortable with the operative technicalities involved.
The major limitations in this study included a retrospective collection of data that, invariably, are associated with selection bias. The small number of patients with varying durations of follow-up are also considerable drawbacks. The long study period reflects the rarity of this condition that requires such radical operations, which then results in the loss of certain patient records. Despite these limitations, the current study demonstrated that pelvic exenteration is a feasible surgical option for selected patients with locally advanced gynecologic malignancies with acceptable short- and long-term outcomes. It is imperative to adopt a multidisciplinary approach when performing such technically demanding operations to achieve better outcomes for the patients.
Conclusions
Pelvic exenteration for locally advanced gynecologic malignancies is associated with acceptable short- and long-term outcomes. Careful patient selection and preoperative counseling are essential in view of the considerable complication rates associated with this operative technique.
Footnotes
Disclosure Statement
The authors state that they have no conflicts of interest to report.