
Abstract
Abstract
Introduction
A
Unfortunately, AM is infrequently considered by gynecologists when a patient presents with right lower quadrant abdominal pain. It often mimics adnexal cysts at preoperative imaging, and the definitive diagnosis is usually made intraoperatively. 4
A case of a right adnexal mass, wrongfully diagnosed by ultrasound scan to be of ovarian origin, is presented. A brief review of AM follows, and the importance of preoperative diagnosis, as well as the need to exclude associated ovarian pathology, is highlighted.
Case
A 66-year-old woman, gravida 4, para 4, was admitted to our clinic with a history of right lower quadrant abdominal pain of 1 year's duration. Her past medical and surgical histories were unremarkable and she had been postmenopausal for 18 years. Her abdomen was soft and nondistended. Bimanual pelvic examination revealed a mass 6 cm in diameter in the right adnexal area. It was slightly mobile, nontender, and solitary, and had smooth walls. Other findings were consistent with menopause. Transvaginal ultrasonography showed a semisolid mass of 65×40 mm, in the right adnexal area, with smooth borders and a thick capsule. This mass was interpreted sonographically as originating from the right ovary. The uterus was atrophic, and the endometrial thickness was 3 mm. There were no inflammatory changes or free fluid in the abdominal cavity. Endometrial biopsy revealed an atrophic endometrium. Routine laboratory tests including tumor markers were within normal limits.
An exploratory laparotomy was performed, with a preoperative diagnosis of solid adnexal mass, suggesting ovarian malignancy, given the age of the patient and the solid nature of the mass. During laparotomy, both ovaries were atrophic and there was no ovarian cyst. The Fallopian tubes and uterus were also atrophic. There was a mass, measuring 6×4 cm, arising from only the tip of the appendix. Surprisingly, a proximal 8 cm from the lesion to the base of the appendix looked absolutely normal (Fig. 1). There was no evidence of mesenteric lymphadenopathy and no free fluid. Also, the exploration of the entire abdomen was free of additional abnormalities. An open appendectomy without rupturing the wall of the appendix and without peritoneal cytology was performed (Fig. 2). Frozen-section diagnosis was an appendix with features consistent with benign mucocele.

Intraoperative image of appendiceal mucocele, right ovary, and uterus. Left arrow, appendix; middle arrow, mucocele, right arrow, right ovary located very closed to the uterus. The clamp is grasping the right tuba uterina. The uterus and right ovary are both atrophic.
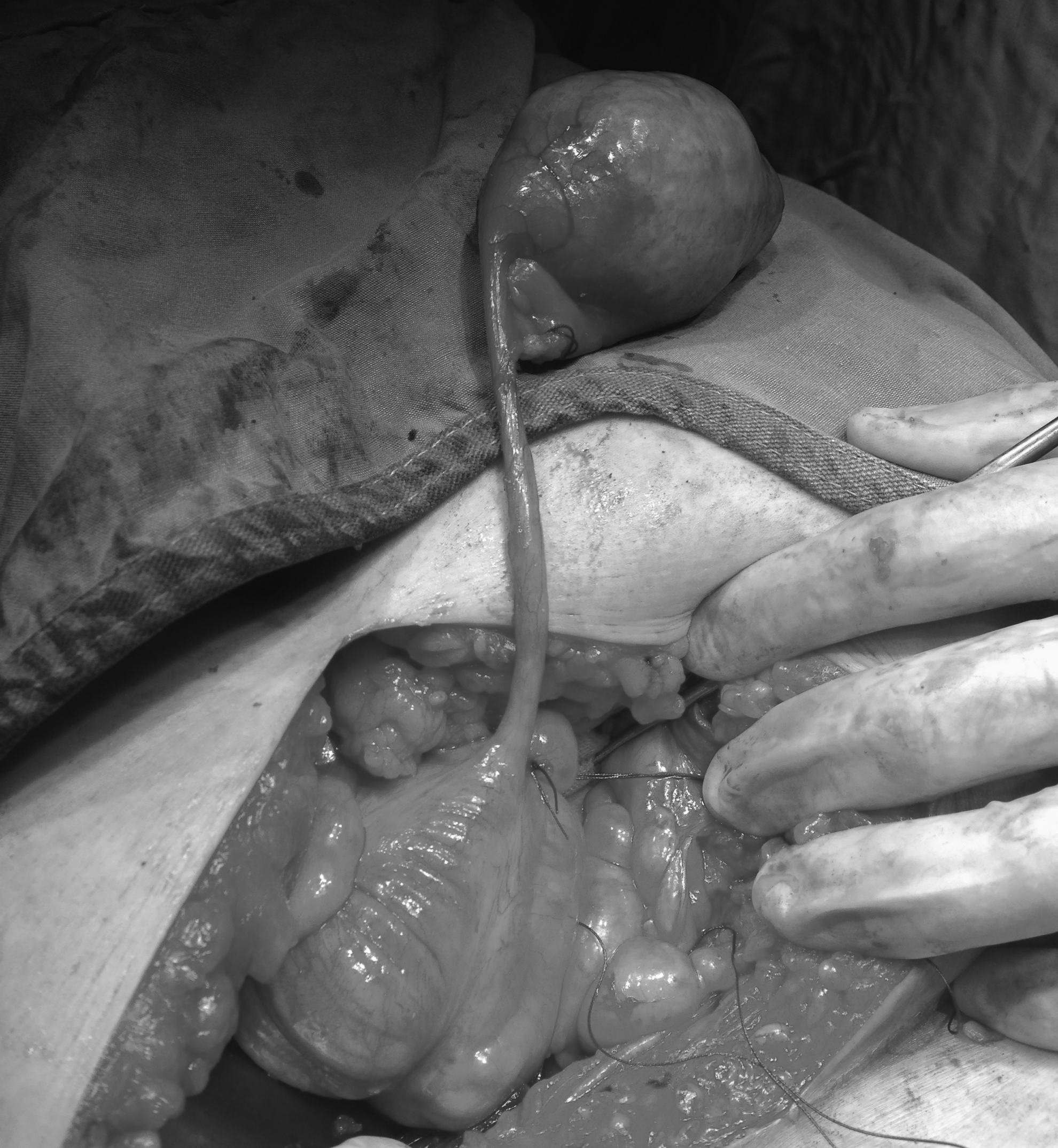
Image of mucocele at the tip of appendix during appendectomy.
Results
The final histopathologic diagnosis of the surgical specimen was mucinous cystadenoma with associated mucocele and there was no evidence of obstruction, inflamation, fibrosis, or fecolith in the appendix lumen (Fig. 3). The patient was discharged home 2 days after surgery following an uneventful postoperative course, and she is asymptomatic clinically 1 month after the surgery.
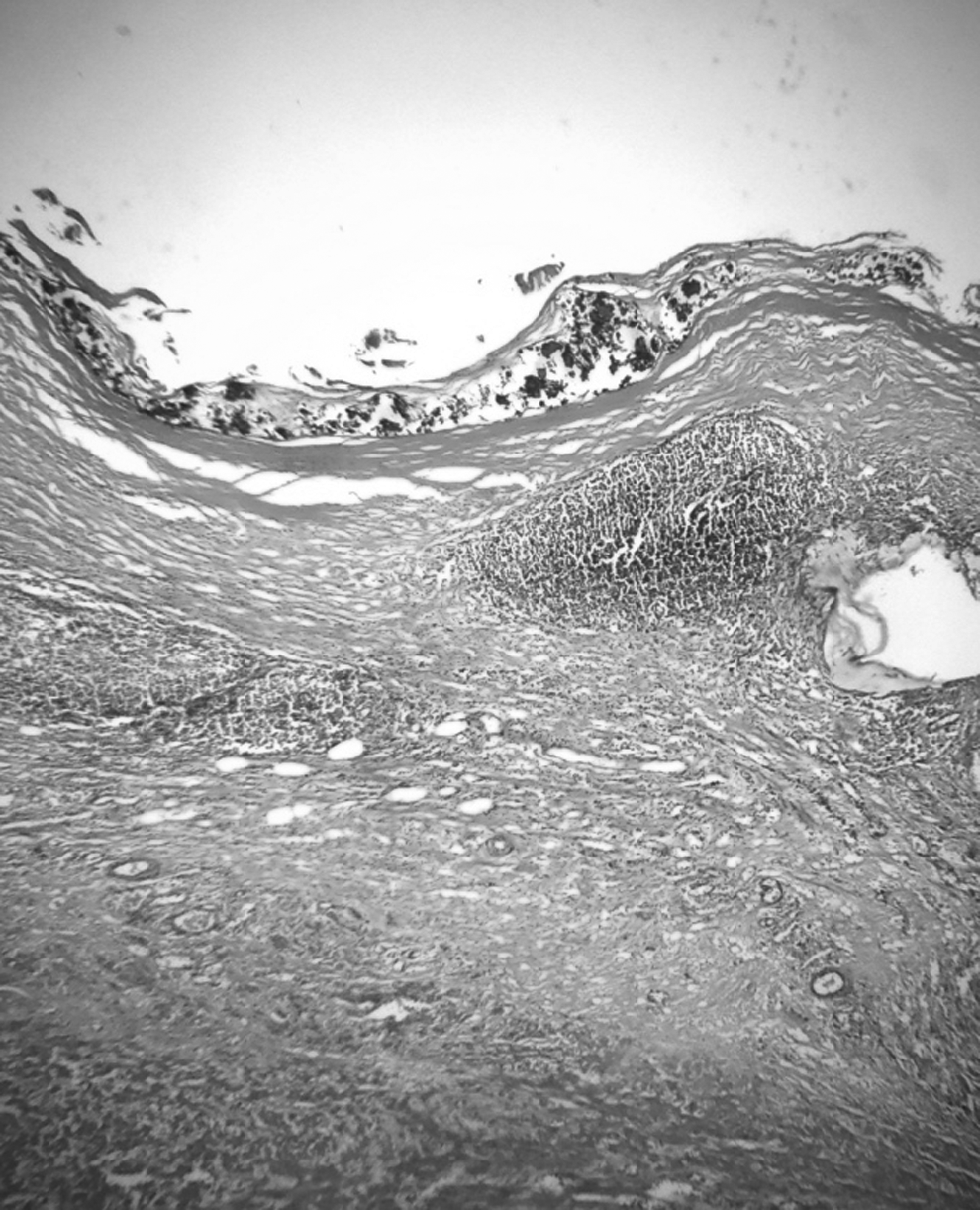
Microscopic view of benign appendiceal mucocele showing a dilated appendiceal wall lined with flattened epithelial cells. There is no evidence of stromal invasion or nuclear atypia in the appendix epithelium (hematoxylin and eosin ×100).
Discussion
AM is a rare cystic dilatation of the appendix lumen by abnormal accumulation of mucous. The pathogenesis could be neoplastic or non-neoplastic. The non-neoplastic (simple) mucoceles are usually the result of obstruction of the proximal appendiceal lumen by post-inflammatory fibrosis or fecolith. The neoplastic origins, which are the result of mucous secretion by an appendiceal cystadenoma or cystadenocarcinoma, comprise the majority of cases. 4
In the literature, the majority of AM cases present mucoceles involving the entire length of the appendix. There are few case reports of AM sparing the base. However, the exact incidence of mucocele confined only to the tip is not known, even with an extensive literature search. In this case, the mucocele involved only the tip, sparing a significant length of the proximal appendix, both grossly and microscopically, which is a peculiar entity.
Appendiceal mucocele does not have a typical clinical presentation. Approximately 23%–50% of patients are asymptomatic, with lesions being discovered incidentally during surgery. Sometimes, it can manifest with acute or chronic abdominal pain, which is the most common clinical finding, altered bowel habits, rectal bleeding, or a palpable mass. 5 Our patient presented with a history of right lower abdominal pain, and a palpable mass in the right adnexal area was detected. Our clinical diagnosis was ovarian mass rather than appendicular lesion.
Preoperative diagnosis of an AM is very difficult. Vaginal and abdominal ultrasonography, computed tomography, magnetic resonance imaging, barium enema, and colonoscopy have all been used to visualize these tumors. Unfortunately, none of these is entirely conclusive. 6 On ultrasound, mucocele can be seen as concentric echogenic layers within a cystic mass in the right lower quadrant of the abdomen in the presence of a normal ovary, which is known as “the onion skin sign.” 7 Computed tomography scan features showing cystic dilatation of the appendix, mural calcification, and a luminal diameter >1.3 cm. are suggestive of AM.8,9 Fine needle aspiration should be avoided in suspected cases of mucocele in order to cause rupture and spread of neoplasm and localized or diffuse pseudomyxoma peritonei. 4
AM should be surgically treated. The surgery depends upon the size of the mass, the integrity of the appendiceal wall, histopathologic findings, and lymph node involvement. AM should be treated with complete excision with careful inspection of the entire peritoneal surface for mucus deposits. In non-neoplastic AM and simple cystadenomas, appendectomy alone is curative. However, in widespread cystadenomas and cystadenocarcinomas, more extended surgery, such as right hemicolectomy, is required. 10 Careful removal of the appendix must be ensured to avoid spillage and prevent peritoneal seeding with subsequent development of pseudomyxoma peritonei. 11 Although the surgical evaluation and removal of an AM, even a right hemicolectomy, is technically possible with laparoscopy, because of the potential of rupture and spillage of mucus from the appendix, these operations should be performed by experienced laparoscopic surgeons. If the surgeon determines that it is not safe to proceed laparoscopically, laparotomy is appropriate. 11
Conclusions
In conclusion, the diagnosis of AM as well as other appendiceal neoplasms, should be considered as a differential diagnosis by the gynecologist in women who present with right adnexal mass. Though no definitive diagnostic tool exists, early diagnosis of mucocele could be beneficial to avoid iatrogenic rupture as well as to plan surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.