
Abstract
Abstract
Introduction
F
The reason for such extensive elimination of oocytes is not known, but this ensures that only the healthiest follicles and oocytes are available for reproduction. The process of follicular atresia is highly orchestrated and finely controlled by various prosurvival and antisurvival intrinsic and extrinsic factors, most of which are unclear and are considered to be areas of ongoing research at present. Interference or suboptimal functioning of any of the ill-understood etiologic factors of this complex mechanism has physical, psychologic, endocrine and reproductive implications for affected individuals. This article presents the clinical case of a 17-year-old girl with this rare disorder and reviews the available literature.
Case
A 17-year-old girl presented to an outpatient department with a history of primary amenorrhea. She also had a history of taking a progestational agent for 5 days 4 months prior to presentation, but this approach failed to work. An examination of this patient showed that she was 5′ tall, weighted 45 kg, and had a body mass index of 20. Her breasts were in Tanner stage 2. There was no hirsuitism and this patient's abdomen was soft and scaphoid. Pubic and axillary hair was sparse and her external genitalia were infantile, with normally located external urinary meatus and introitus. A rectal examination showed that she had a nulliparous-size uterus anteriorly.
Various hematologic, endocrine, and radiologic investigations were requested, which revealed a 46 XX chromosomal pattern and the following serum levels: follicle-stimulating hormone (FSH), 6.2 mIU/mL; leuteinizing hormone (LH), 2.1 mIU/mL; thyroid-stimulating hormone, 2.5 U/mL; prolactin, 5 ng/mL; testosterone, 106 pg/mL; estradiol, 2.5 pg/mL; progesterone, 0.8 ng/mL; and dehydroepiandrosterone sulfate, 145 mg/dL. A transabdominal ultrasonic scan revealed a normal-size uterus (6×4.3×3 cm) and small ovaries (the right ovary was 2.1×1.5 cm and the left ovary was 2×1.3 cm), with no evidence of follicles in them. Intravenous pyelography and echocardiography test results were were normal.
The girl underwent a diagnostic laparoscopy, which revealed a normal-size uterus and bilateral Fallopian tubes. Both of the pearly white ovaries were located normally but were small (the right ovary was 2.5×1.5 cm and the left ovary was 2.4×1.3 cm) and shiny, with smooth surfaces (Fig. 1). A biopsy from the ovaries was performed. Histology testing revealed follicular atresia in an abundant stroma in the biopsy specimen (Fig. 2).
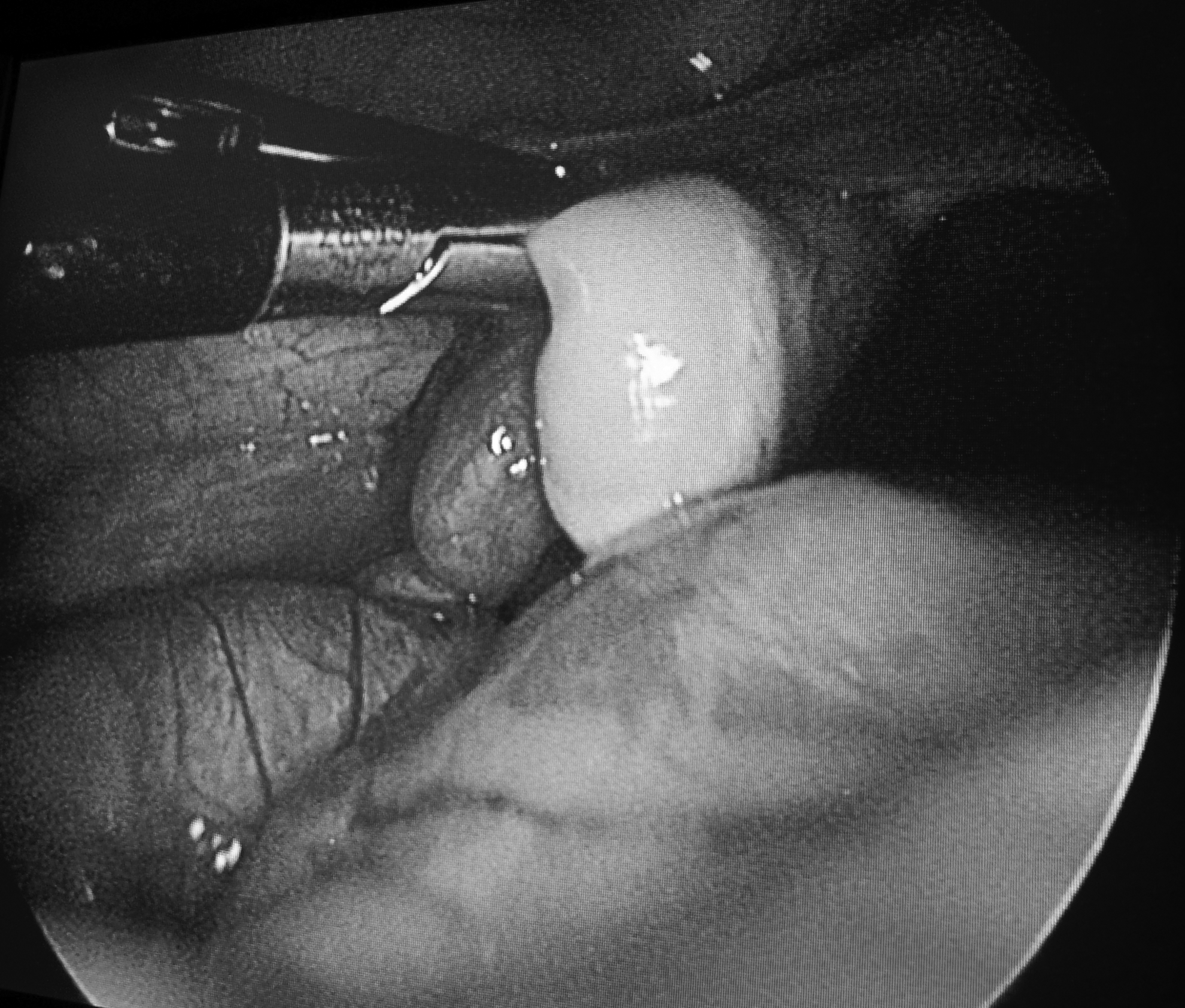
Laparoscopic view of the smooth-surfaced, small, pearly white right ovary.
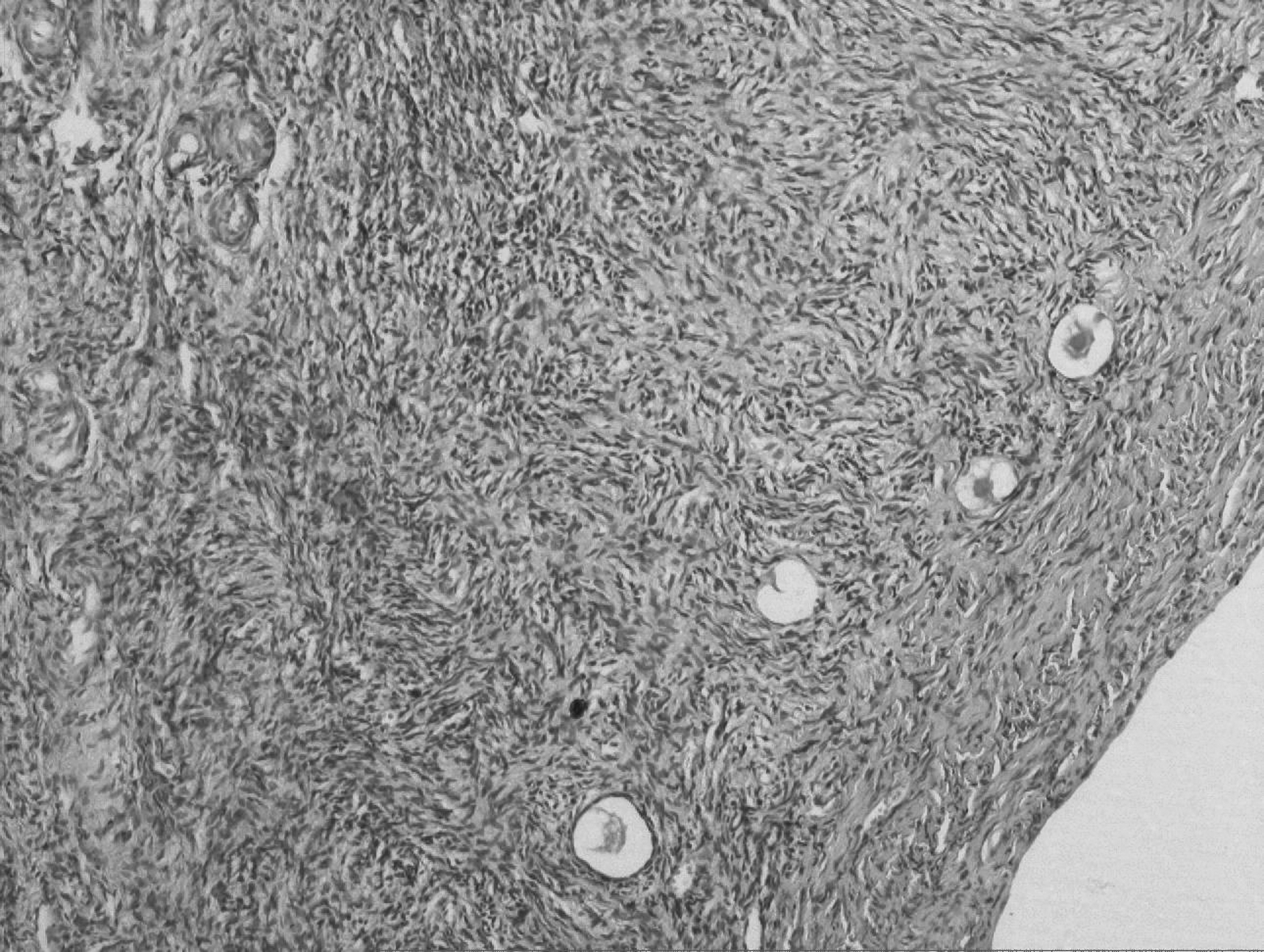
Microphotograph of the ovarian biopsy specimen showing atretic follicles in dense abundant stroma (H&E×100).
After the laparoscopy and all testing was completed, the patient was prescribed a combination of oral contraceptive pills (50 μg ethinyl estradiol in each tablet), vitamin D, and calcium.
Results
The patient had an uneventful postoperative course and started having monthly menses, 3 months after initiation of therapy.
Discussion
The term follicular atresia (Greek: a=not and tresia=perforated) in the literal sense refers to failure of a follicle to rupture (i.e., ovulate). The primordial germ cells that number around 7 million in the ovaries during the intrauterine life of a 20 week-old fetus continue to decline in number as a consequence of follicular atresia to reach a count of 1 million at birth and 4 lacs of oocytes at puberty. This massive loss of germ cells in the prenatal period is termed oocyte attrition, whereas the postnatal depletion of oocytes occurs via follicle atresia. 1
The regulation of follicular atresia is a complex issue and most of the available studies in this area pertain to bovine ovaries, in which antral and basal follicular atresia have been described. 2 Antral atresia refers to the elimination of granulosa cells proximal to the antrum. However, basal atresia entails the destruction of basal follicular layer, while the antral layers remain intact and healthy. Atresia occurs via apoptosis of the somatic cells of the follicle and oocyte. 3
Follicular recruitment, selection, and atresia are highly orchestrated processes, encompassing roles of the ovarian milieu and various proapoptotic and antiapoptotic mechanisms. 4 Many intrinsic (stress-provoking factors, such as nutrition deprivation, oxidative damage, and genetic impairment) and extrinsic factors (such as cytokines, γ interferons, and growth factors) have been postulated to have roles in controlling granulose cells and hence follicular fates. Members of the tumor–necrosis factor (TNF) superfamily and the Fas ligand–Fas system (a cell-surface receptor protein expressed on granulosa cells) are among the most readily identified proapoptotic molecules in human and bovine ovarian follicular atresia.5,6 However, various extracellular (such as gonadotropins, steroids, and some cytokines and growth factors) and intracellular (such as cyclins and cyclin-dependent kinases, Akt, cellular FLICE inhibitory protein, cFLIP, and Bcl-2, an apoptosis-regulator protein) antiapoptotic or prosurvival molecules promote growth and proliferation of cells within the follicle. 7
Among the gonadotropins, FSH suppresses the apoptosis of granulosa cells in large follicles whereas LH suppresses apoptosis of granulosa cells in large follicles only.8,9 Increasing estradiol synthesis is an important sign of a healthy follicle with viable granulosa cells. Estradiol protects the granulosa cells from apoptosis by increasing cyclin D2 expression and stimulating the cells to progress from the G1 to the S phase of the cell cycle. 10 As the granulosa cells become luetinized consequent upon the LH surge in midcycle, their responsiveness to progesterone is increased, thus triggering their withdrawal from the cell cycle. 11 A high androgen-to-estradiol ratio within the follicles is also reported to indicate follicular atresia as androgen inhibits the FSH-stimulated LH-receptor expression in the later stages of folliculogenesis, thus enhancing granulosa-cell apoptosis. 12
Follicular atresia is necessary for a woman to maintain a healthy reproductive system. The inability to regulate granulosa-cell apoptosis and undergo follicular atresia has been linked to the development of granulosa-cell tumors and chemoresistance. 13
However, an overly rapid rate of follicular atresia has immense reproductive, physical and psychologic implications for the affected individual. An important question for the definitive management of this disorder would be whether or not the atretic follicles can be brought into the normal cell cycle again. In a normal ovarian cycle, estrogen stimulates the normal granulosa cells to progress from the G1 to the S phase of the cell cycle in a normal ovarian cycle. An LH surge luteinizes the granulose cells, which then become more responsive to progesterone than to estradiol, and progesterone withdraws them from the cell cycle. As the outgoing granulosa cells are not responsive even to high levels of estrogens, the salvagibility of these follicles is questionable and a remote possibility as of now. Currently, management consists of induction of cyclical menstruation by combined estrogen and progestin preparation. Supplementation with vitamin D and calcium would help ward off the adverse effects of long-term hypoestrogenism on bone-mineral density.
Conclusions
Ovarian follicular atresia in humans is a complex process that is not yet fully understood. Given the far-reaching physical and psychologic impact of this disorder, current management modalities aim to restore menstrual function and prevent the long-term bone and cardiovascular effects of estrogen deprivation.
Footnotes
Disclosure Statement
No competing financial conflicts exist.