
Abstract
Abstract
Introduction
O
Case
A 30-year-old woman presented with complaints of pain and heaviness in the right iliac region. Abdominal examination revealed a pelvic mass, 18 weeks of gestation in size, with restricted mobility, palpable in the right iliac region. On vaginal examination, a mass was felt in the right fornix with restricted mobility and tenderness. Ultrasonography (USG) revealed a large mass of 14.3×13.2×12.5 cm, occupying whole of the pelvis just superficial to the fundus, but not arising from the uterus (Fig. 1).

Ultrasonography shows a large heterogeneous echoic mass occupying the whole of the pelvis, just superficial to the fundus, but not arising from the uterus.
Magnetic resonance imaging (MRI) revealed a large oval well- defined altered signal intensity mass of 14.7×14.6×10 cm in the right lower abdomen and pelvis, with a moderate amount of fluid signals in the abdomen and pelvis (Fig. 2). Her preoperative routine test results were normal except for mild anemia, with hemoglobin (Hb) 9.0 gm%. CA-125 value was 69.9 international units (IU)/mL.
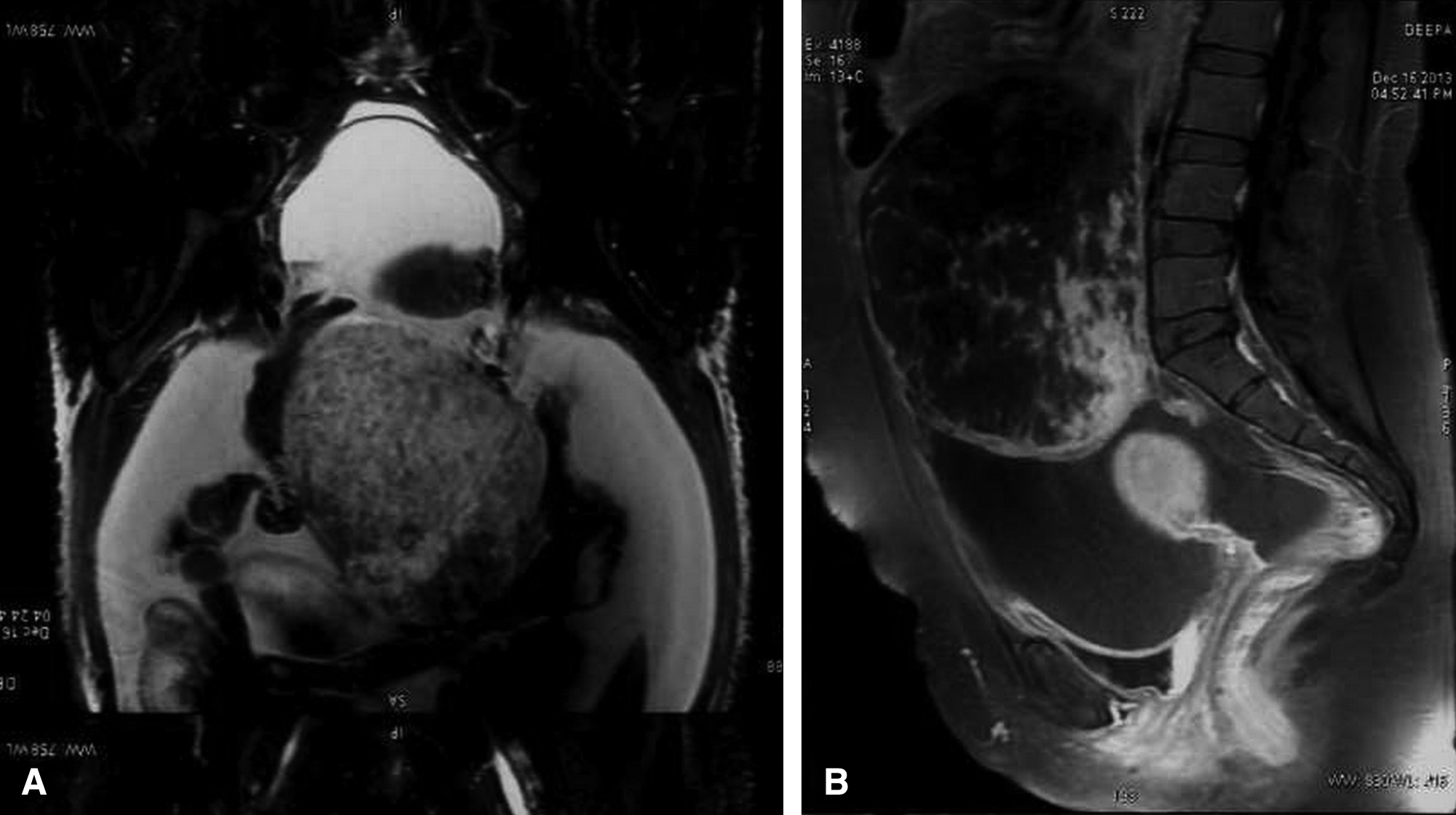
Magnetic resonance imaging shows a large well-defined altered signal intensity mass in the right lower abdomen and pelvis.
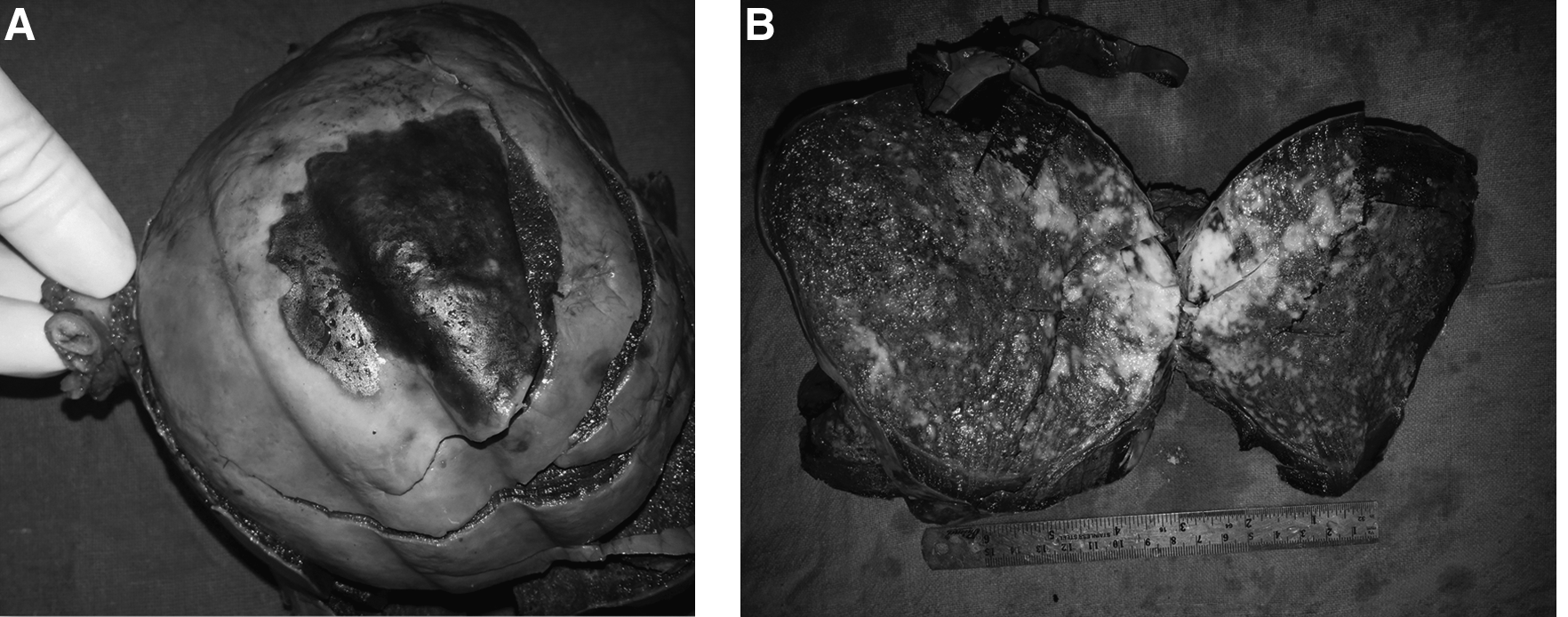
An excised right ovarian mass measuring 15×12×11 cm was sent for histopathologic examination along with an attached Fallopian tube measuring 3.5×0.6 cm. An omental biopsy was also sent, to rule out metastatic deposits. The cut surface of the mass was variegated, with areas of hemorrhage and necrosis (Fig. 3). Histopathologic examination showed a tumor composed of oval to spindle shaped cells revealing mild-to- moderate nuclear pleomorphism, which was mitotically active with >10 mitoses per 10 high-power fields (HPF) (Fig. 4). The structure of a normal ovary was identified in sections taken from the periphery of the mass. On immunohistochemistry, the tumor cells were noted to be positive for desmin, vimentin, and smooth muscle actin, and negative for inhibin (Fig. 5). The result of an omental biopsy was found to be negative for metastatic tumor deposits.
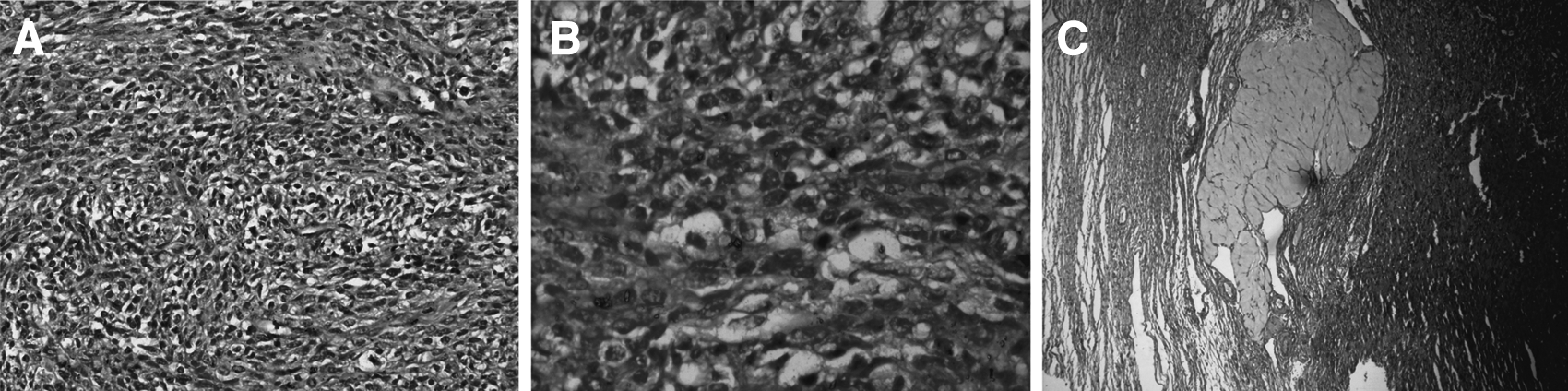
Oval-to–spindle-shaped cells revealing mild-to-moderate nuclear pleomorphism and high mitotic activity.
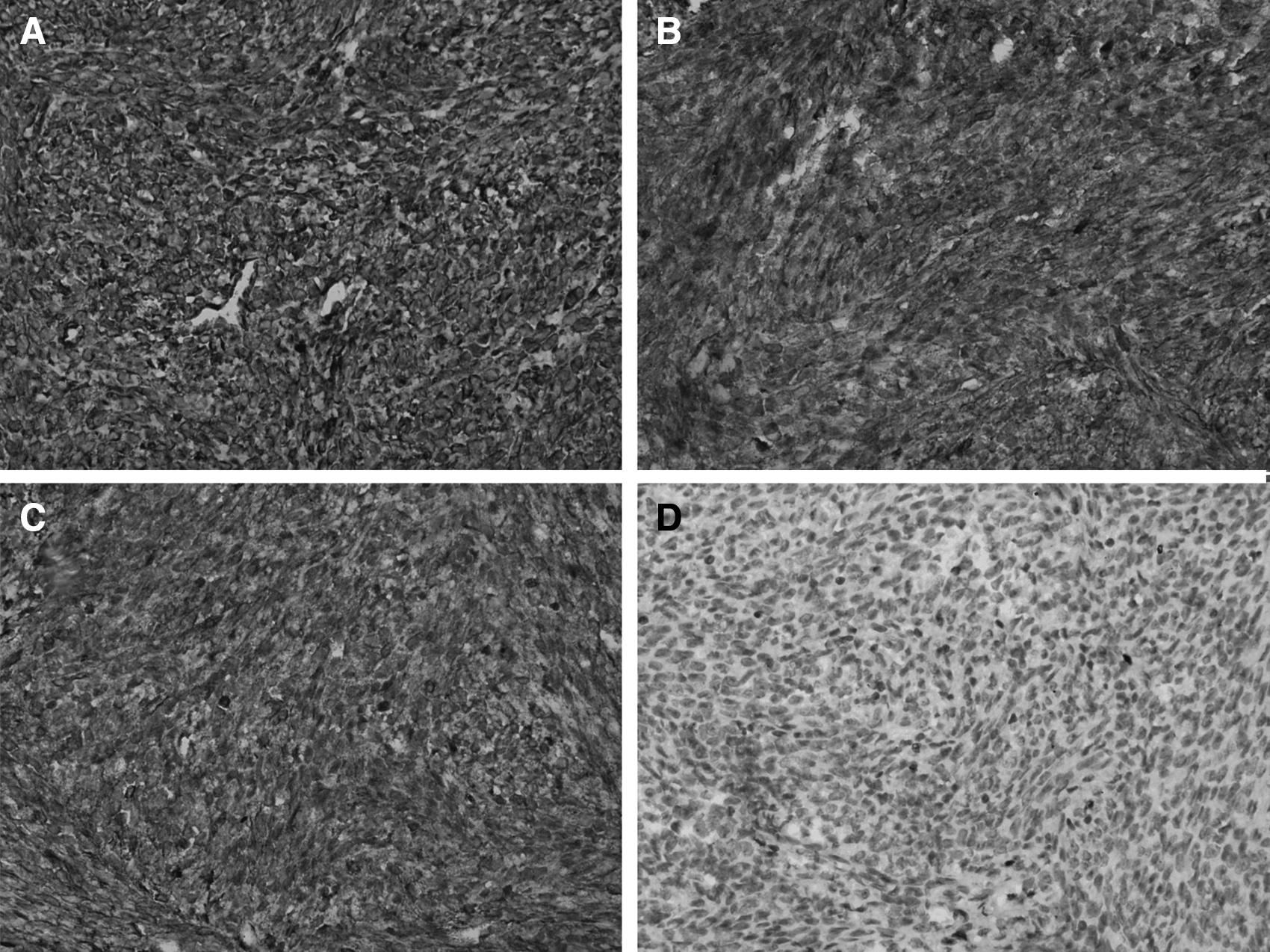
Photomicrograph showing immunohistochemical expression of tumor cells. The tumor cells show intense cytoplasmic positivity for vimentin
Results
Taking into account morphology and immunohistochemistry, a diagnosis of ovarian leiomyosarcoma was made. Subsequently, the patient was given chemotherapy, and has been on follow-up for 4 months, which have been uneventful to date.
Discussion
Primary smooth muscle ovarian tumors are rare, and account for <3% of ovarian tumors. The most common smooth muscle tumors are rhabdomyosarcoma, fibrosarcoma, and leiomyosarcoma, which is the rarest, and accounts for <1% of all cases. Only 55 cases have been reported so far. The majority of cases occur in women in the peri- and postmenopausal age group: between 45 and 65 years of age. There is little information on their origin, etiology, histologic features, clinical behavior, and treatment. 3
Pathogenesis is uncertain, with many theories, including: malignant degeneration of an ovarian leiomyoma, or of the smooth muscle present in the wall of the blood vessels in the cortical stroma and corpus luteum; muscular attachments of the ovarian ligament; Wolffian duct remnants; or totipotential ovarian mesenchyme, or arising in a teratoma. 4 These tumors are usually well-circumscribed and have a tendency to reach a very large size. These sarcomas also tend to have features of necrosis, hemorrhage, and cystic degeneration.
Ovarian leiomyosarcomas generally are highly malignant and present with local, hematogenous, or lymphatic spread. Distant metastasis has been seen, mainly in the lungs and liver in the cases diagnosed so far. On histopathologic examination, markedly pleomorphic spindle-shaped cells intersecting each other at wide angles are seen. Nuclei of the cells are vesicular and ovoid or cigar shaped. The tumors show immunoreactivity for smooth-muscle actin, desmin, and caldesmon. Often, these tumors present with brisk mitotic activity. Generally, malignant potential behavior of smooth-muscle tumors is associated with any two of the following features: coagulative necrosis; cellular atypia; and a mitotic index >10/10 HPF. 5
The majority of cases have a poor prognosis, with death ensuing within 1 year of diagnosis. The International Federation of Gynecology & Obstetrics (FIGO) staging and treatment of ovarian leiomyosarcoma have been the same as those for ovarian carcinoma. 6 Prognosis depends upon the tumor stage, tumor size, and mitotic index.
Conclusions
There is no established treatment for these sarcomas other than surgery. 7 Most of these tumors are radioresistant. Dixit et al. have suggested postoperative radiotherapy and chemotherapy in large tumor volumes, to control local disease and avoid metastatic recurrence. 8
Footnotes
Disclosure Statement
No financial conflicts of interest exist.