
Abstract
Abstract
Introduction
H
The aims of this report are (1) to illustrate the intrafascial technique for TAH as performed at the Faculty of Medicine, Chiang Mai University, in Chang Mai, Thailand, and (2) to describe clinical and operative outcomes of patients with benign gynecologic conditions who underwent TAH including this technique.
Materials and Methods
The clinical, operative, and pathologic data of all patients who underwent total abdominal hysterectomy using the intrafascial technique for benign gynecologic conditions from January 2003 to December 2012 were reviewed retrospectively. Descriptive statistics were used to elucidate surgical outcomes. The study was approved by the research ethics committee of Faculty of Medicine of Chiang Mai University.
Surgical procedure
After general anesthesia is induced and the patient is placed in a supine or dorsal lithotomy position, abdominal hysterectomy is started. The procedure can be performed through various types of incisions: vertical midline; Pfannenstiel; Maylard; or Cherney. In the initial phase of the operation, the surgical steps are the same as those performed during extrafascial hysterectomy. The lateral attachments—including round ligaments, ovarian or infundibulopelvic ligaments, and broad ligaments—are transected on both sides. Then the vesicouterine peritoneal fold is exposed and incised. The urinary bladder is dissected sharply away from the lower segment of the uterus and the cervix. The uterine arteries are clamped, cut, and suture-ligated on both sides.
At this point, the endopelvic fascia (pubovesicocervical fascia)—which is a dense, thin layer of connective tissue that surrounds the lower uterine segment, the cervix, and the upper vagina—can be seen on the anterior surface of the lower uterine segment. To be able to identify the upper edge of the fascia more clearly, an additional piece of the upper cardinal ligament is transected on each side (a “bite” is taken).
Subsequently, the “intrafascial plane” can be created by dissecting the fascia sharply away from the underlying uterine and cervical wall between the two points at which the upper cardinal ligaments are ligated. The fascial dissection can be initiated from its exposed upper edge by using the tips of Mayo scissors in a sweeping movement from one side to the other (Fig. 1). On the posterior surface of the uterus, the fascia is covered by a layer of peritoneum. There is no need to separate this peritoneum from the fascia. The intrafascial plane on the posterior surface is exposed in the same fashion as performed on the anterior surface by taking the fascia together with the overlying peritoneum (Fig. 2).

Next, the fascia can be identified as a dense connective tissue cuff surrounding the cervix and the upper vagina. Subsequent transection of the uterine supporting structures, including the remaining cardinal ligaments and the uterosacral ligaments, is continued in the intrafascial plane inside the fascial cuff, which provides natural protection for adjacent organs (Fig. 3). Note that in order to avoid accidental injury to the adjacent structures, especially the ureter, each suture ligation is placed inside the exposed fascial cuff without incorporating the fascia.

Then, the uterus and both adnexa are removed. The vaginal cuff is closed by using the continuous double-layer technique. The first layer approximates the vaginal wall including the vaginal mucosa. The second layer brings together the anterior and posterior edges of the endopelvic fascial cuff. Note that this layer also incorporates the top part of the vaginal vault from the first layer into each bite (Fig. 4). As the endopelvic fascia is one of the most important supporting structures for pelvic organs, this procedure provides strong support for the vaginal vault. The technique also obliterates dead spaces and facilitates hemostasis. Video 1 demonstrates the basic technique (see Supplementary Data available online at www.liebertpub.com/gyn).

Figures 5–7 show the application of the intrafascial technique for abdominal hysterectomy in a patient with severe pelvic endometriosis obliterating the posterior cul-de-sac. Video 2 demonstrates the application of the technique in this case (see Supplementary Data available online at www.liebertpub.com/gyn).

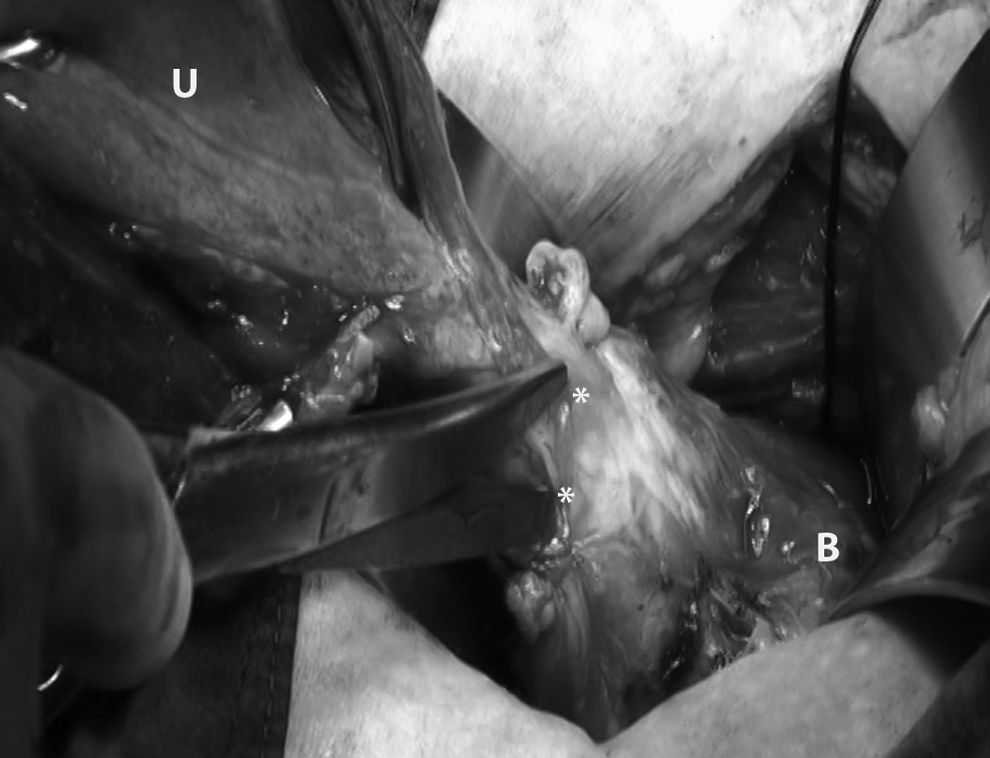
The posterior cul-de-sac is obliterated by a loop of rectosigmoid, which adheres densely to the posterior wall of the uterus. Application of the intrafascial technique for abdominal hysterectomy in a patient with severe pelvic endometriosis obliterating the posterior cul-de-sac (together with Figs. 6 and 7). U, uterus; R, rectosigmoid.
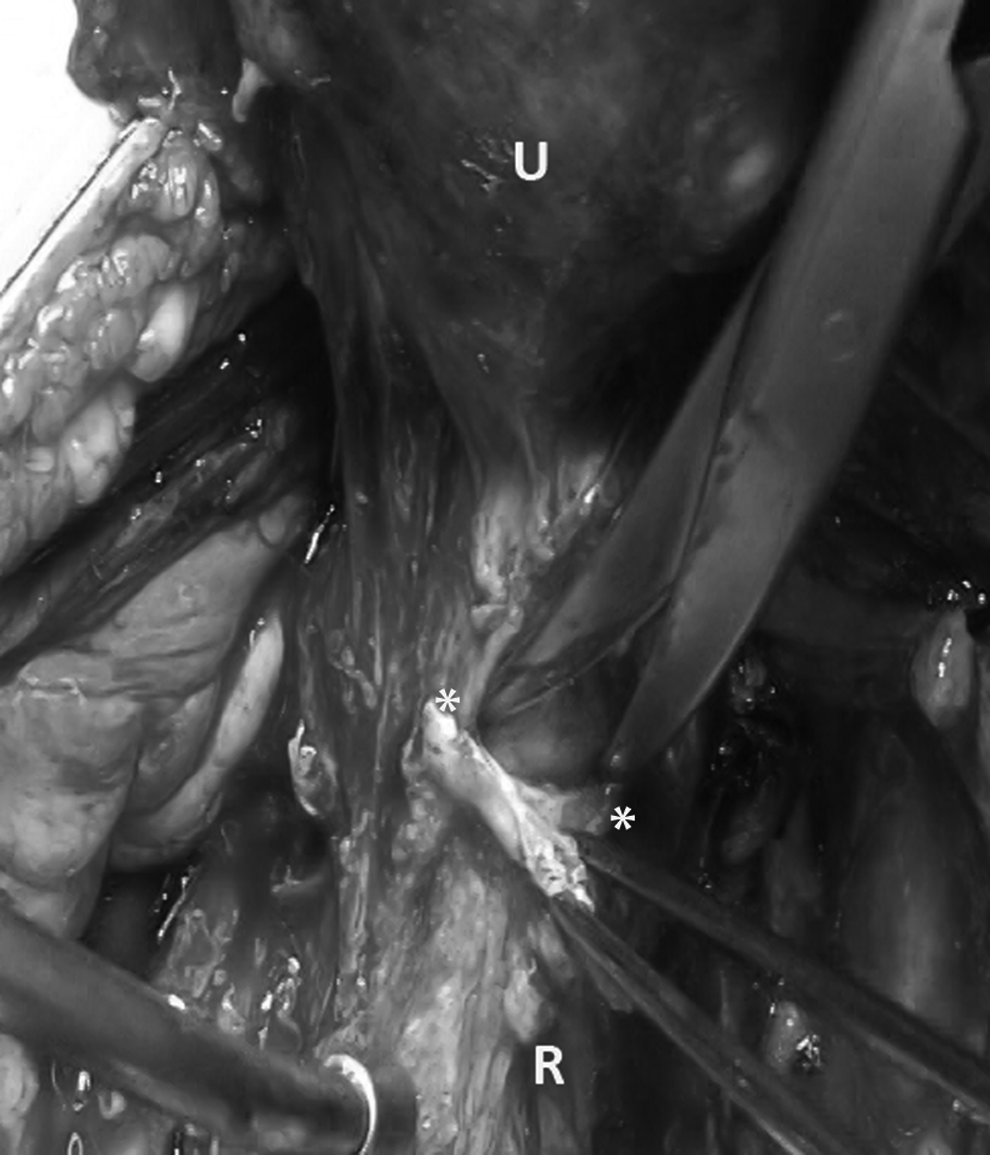
The intrafascial plane on the posterior uterine surface is exposed by gradually dissecting the endopelvic fascia away from the underlying uterine wall down to the level of the uterosacral ligaments. Application of the intrafascial technique for abdominal hysterectomy in a patient with severe pelvic endometriosis obliterating the posterior cul-de-sac (together with Figs. 5 and 7). U, uterus; *, upper edge of the posterior endopelvic fascia; R, rectosigmoid.

Exposure of the intrafascial plane on the posterior uterine surface can be accomplished by sharp dissection. Application of the intrafascial technique for abdominal hysterectomy in a patient with severe pelvic endometriosis obliterating the posterior cul-de-sac (together with Figs. 5 and 6). US, uterosacral ligament; IF, the intrafascial plane, *, upper edge of the posterior endopelvic fascia.
Results
From January 2003 to December 2012, 161 patients underwent TAH including the intrafascial technique as treatment for benign gynecologic conditions. The current author was the primary surgeon for all of these operations. The median age of the patients was 47 (range: 25–79). Twenty-one patients (13%) were menopausal. The median parity was 1 (range: 0–7). The median body mass index was 23.3 kg/m2 (range: 17.2–34.4 kg/m2). Forty-three patients (26.7%) had had previous abdominal surgery. The most common operative indication was uterine fibroid growths; this was seen in 126 patients (78.3%). Abdominal incisions included Pfannenstiel (102 patients; 63.4%), vertical midline (53 patients; 32.9%), Cherney (five patients; 3.1%), or Maylard (1 patient; 0.6%). Bilateral salpingo-oophorectomy and unilateral salpingo-oophorectomy were performed in 100 patients (62.1%) and 22 patients (13.7%), respectively. Thirty-five patients (21.7%) had incidental appendectomy. In 64 patients (39.8%), marked pelvic adhesions (from endometriosis, infections, or previous surgery) and/or limited exposure and mobility of the uterus (from multiple or intraligamentary fibroid growths) were noted. The median operative time was 142 minutes (range 91–293 minutes). The median operative blood loss was 200 mL (range: 50–4,000 mL). Ten patients (6.2%) had intraoperative complications involving >1000 mL blood loss.
There was no intraoperative injuries to urologic or GI organs. Postoperative complications were noted in 4 patients (2.5%): postoperative ileus in 3 patients and a vaginal stump abscess in 1 patient. There was no need for reoperations. At 6-week postoperative visits, all patients had recovered well without complications.
Discussion
The leading complications associated with abdominal hysterectomy reported in comprehensive reviews of hysterectomy complications over the last few decades included infection, hemorrhage, and injuries to adjacent organs.8,9 The rates of these complications varied widely among studies, depending mostly on underlying pelvic pathology, previous surgeries, and body habitus. Of note, according to the current clinical guideline on route of hysterectomy for benign conditions, the candidates for abdominal hysterectomy would consist of patients with large uteri for which the size reduction procedures are not possible and patients with severe extrauterine diseases obliterating the cul-de-sac resulting from severe adhesions or severe endometriosis. Patients with milder pelvic pathology would be surgically managed by vaginal or laparoscopic hysterectomy. 10 Therefore, it is reasonable to expect that the abdominal hysterectomies performed currently based on this guideline would be selectively more difficult operations with increased risks of complications. The need for a safe technique for abdominal hysterectomy is more apparent than ever. The intrafascial technique is safe, effective, and readily available but is largely neglected by the gynecologic community. It is also important to emphasize the difference between this procedure and the classic intrafascial supracervical hysterectomy (CISH technique), the subtotal hysterectomy with transuterine mucosal resection and coring of the cervicouterine cylinder. 11
The most obvious benefit of the intrafascial technique is the maximal protection to adjacent structures, specifically the ureter, bladder, and rectosigmoid colon. During hysterectomy for benign conditions, the risk of injury to these structures is increased if severe endometriosis, dense adhesions, large lower-segment or cervical fibroid growths, and/or large adnexal masses are encountered. The most dangerous part of the procedure is the removal of the cervix.
The general principle for preventing ureteral injury is for the surgeon to have knowledge of its location and course at all times, either by direct visualization or palpation. However, this is not always possible with the presence of a large distorted uterus or in severe extrauterine disease, especially for the part of the ureter that courses between the uterine artery and the bladder. Similarly, for prevention of rectosigmoid injury, sharp dissection close to the uterus has been recommended. However, this method cannot guarantee bowel safety.
The intrafascial technique, as illustrated in this report, consistently permits safe removal of the cervix together with the uterus during TAH. During the intrafascial hysterectomy, the well-developed fascial cuff becomes a natural wall that separates the path of parametrial resection from surrounding structures. This is particularly important in patients with severe pelvic adhesions from endometriosis, infection, or previous surgery, which distorts pelvic anatomy. Merely dissecting and clamping “close to the uterus” are not enough to ensure safe resection in these situations. The clamping, cutting, and suturing have to be performed strictly in the intrafascial plane. Given that the patients in this study were operated on in the largest tertiary care hospital in the northern region of Thailand, a significant proportion of the patients in this series were referred from other hospitals with diagnoses of complex pelvic pathologies. However, after these patients were operated on, using the intrafascial technique, there was no incidence of intraoperative injury to surrounding urologic and GI structures. Supracervical or subtotal procedures, which are performed mainly to prevent injury to the ureter, bladder, or rectum during cervical removal, were not needed in this series.
Operative-site infection, which includes pelvic cellulitis, vaginal cuff abscess, pelvic abscess, and wound infection, is the most common complication following abdominal hysterectomy with an incidence of 6.6%–24.7%. 9 With prophylactic antibiotics, the reported rates of operative-site infection were ∼9%. 8 The rate of operative-site infection in the present series was very low. This is consistent with the rates reported in other series examining intrafascial abdominal hysterectomy, 4% in the Conde-Agudelo study 6 and 4.8% in the Kaya et al. study. 12 Apart from the use of antibiotics, the low incidence of operative-site infection associated with intrafascial hysterectomy could be related to the effective hemostasis and obliteration of the dead space at the vaginal vault.
Intraoperative hemorrhage, defined as requiring blood transfusion or losing more than 1000 mL of blood intraoperatively, was encountered in 0.2%–3.7% of the patients during abdominal hysterectomy. 9 The rate of intraoperative blood loss of >1000 mL was 6.2% in the current study, which was higher than those previously mentioned. In the prospective cohort study of intrafascial hysterectomy by Conde-Agudelo, 6 blood loss was 286±112 mL and that was comparable to the median blood loss of 200 mL in the present study, but the rate of intraoperative blood loss or blood transfusion of 0.2% was much lower. The higher rate of intraoperative blood loss in the current series of patients could be explained by the fact that a significant proportion (40%) of the cases involved severe adhesions or large/distorted uteri.
Experienced surgeons who are familiar with the intrafascial technique for hysterectomy would agree that intrafascial plane development would be unlikely to contribute to excessive bleeding. With the use of the tip of Mayo scissors in a sweeping movement to enter the endopelvic fascial plane, starting at its exposed upper edge from one side to the other, the associated blood loss was generally minimal. This is clearly different from the bleeding that may be encountered when dissecting through myometrium during myomectomy.
Conclusions
When TAH is performed for benign pelvic diseases, especially in patients with large distorting uteri and/or severe pelvic adhesions, the intrafascial technique should be the procedure of choice. This is particularly the case when the additional advantages of the procedure are taken into account. These include its simplicity, obliteration of the dead space around the vaginal vault, effective vault hemostasis, and strong vaginal-vault support. In the current author's experience, many potential urologic and GI injuries were avoided by using this technique. It is true that, in patients with mild uterine pathology without other apparent pelvic diseases, the extrafascial technique could be performed safely. However, abdominal hysterectomy would be less indicated in that situation, according to the current guideline regarding route of hysterectomy. For modern gynecologists to be able to perform safe hysterectomies for any benign conditions, knowledge of the intrafascial technique for TAH and adequate hands-on experience with the procedure are crucial.
Footnotes
Acknowledgments
The Faculty of Medicine of Chiang Mai University and the National Research University Project under Thailand's Office of the Higher Education Commission supported this project.
Disclosure Statement
The author reports no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.