
Abstract
Abstract
Introduction
P
Surgical treatment is an effective option for such patients. Various surgical techniques have been proposed to correct POP. Sacrospinous ligament fixation (SSLF) with or without uterine preservation is a safe and effective procedure for treating uterovaginal prolapse.1,2 Known complications of sacrospinous fixation with or without uterine preservation for treating POP or vaginal-vault prolapse are hemorrhage; cystitis; perforation of the bladder, rectum, or small bowel; rectovaginal fistulae; postoperative pain of the gluteal region; and nerve injury.3–5 General or regional anesthesia complications may also occur.
The following case illustrates the current authors' experience in performing SSLF with uterine preservation under local anaesthesia at a regional hospital (Dar El Hanan) in Djibouti, Africa by voluntary action.
Case
A 70-year-old woman was referred with total uterine prolapse. She had pain because of rubbing. She had 8 children, all of whom were delivered vaginally. She was 160 cm tall and weighed 80 kg. She had smoked cigarettes for 45 years. An examination showed that she had a stage 4 uterovaginal prolapse but not urinary incontinence. The patient was counseled about treatment options. A preoperative anesthesia consultation was arranged. She had chronic obstructive pulmonary disease (COPD) and cardiac failure. Because of these conditions, the anesthesist deemed it unsafe to proceed with general or regional anesthesia (an American Society of Anesthesiologists [ASA] level 3 contraindication). She was offered various options, including colpocleises, SSLF under local anesthesia, or a vaginal pessary. However, pessary application was not appropriate for this patient because of difficulties with follow-up for this in Turkey. In addition, the patient wished to retain her vaginal orifice. Thus, there was only one option left—performing the operation under local anesthesia. The obstetrics and gynecology department of the regional hospital in Djibouti explained the operation exactly in their own language to the patient and the patient agreed to undergo this procedure.
She was placed in a litotomy position, cleaned, and draped, and a Foley catheter was inserted into the bladder. Infiltration was performed with 10 mL of %1 lidocaine diluted in 10 mL of saline. No intravenous sedation or oxygen mask was used. The patient was conscious during the operation. Her pain was assessed every 2 minutes with a visual analogue scale.6,7 Her pain level was a 2 maximum score. Infiltrative anesthesia was performed in the posterior vaginal wall and in the right side of the vaginal wall at an ∼ 1-cm depth through the spina ischiadica. Infiltration (0.5 mL) was also applied through the spina ischiadica into each part of the dissection area.
A vertical incision was made from the apex of the posterior vaginal-wall prolapse to the fourchette. The pararectal space was entered easily by a finger on the right side of vagina. The sacrospinous ligament was visualized clearly. The fixation was performed with a # 1 propylene suture between the sacrospinous ligament and ½ of the distal part of the sacrouterin ligament and cervix (Fig. 1). The vagina was closed with a # 2 absorbable suture before tying the sacrospinous ligament fixation (Fig. 2). The operation lasted 20 minutes and her total blood loss was estimated to be 40 mL. Her urine was clear so the Foley sonda was removed.
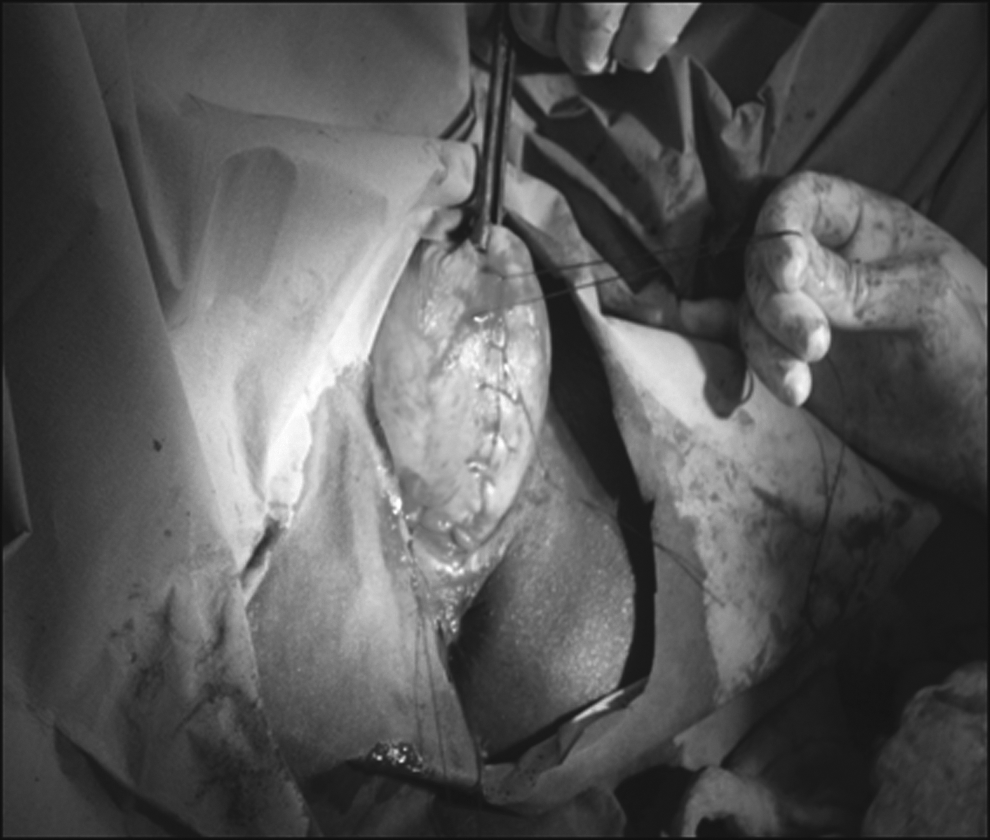
The suturation of cervix and 1/2 distal part of the sacrouterin ligament before sacrouterine ligament fixation.

The appearence of the perineum after surgery.
Results
This patient was fully mobile after undergoing the procedure and was discharged to go home on the same day. She recovered well and was delighted with the outcome.
Discussion
Prolapse operations in postmenopausal women who have comorbidities force surgeons to use minimally invasive procedures. In addition, local anesthesia is a comfortable approach for such patients, as it avoids the complications of general or regional anesthesia and may allow surgeons to perform operations these patients. Because prolapse surgery is a condition that occurs mostly in postmenopausal women, systemic conditions may frequently be present. Operations under local anesthesia have been performed, including locals, paracervical blocks, or pudendal nerve blocks. Light sedation has also been used when performing anterior or posterior vaginal-wall repairs, enterocele repairs, Le Fort colpocleises, and cervical amputations.8–10
One report described this method for SSLF for the first time in the literature. 11 For that procedure, infiltration was performed with 30 mL of bupivacaine, and 0.5% adrenaline (1 in 200,000) diluted in 30 mL of saline. Intravenous sedation was also initiated with 4 mg of midazolam, 8 mg of morphine, and 20 mg of propofol. This sedation was maintained with an infusion of propofol at a rate of 200 mg/hour, and a 70% oxygen mask was also used.
In the current case neither an oxygen mask or nor intravenous sedation was used. Thus the current case was the first case in which the procedure was performed under only local anaesthesia.
Colpocleisis is a minimally invasive surgery that is indicated for repairing apical prolapse, either posthysterectomy or with the uterus in situ. However, this procedure is not appropriate for women who wish to engage in vaginal intercourse. 12 In the current, case the patient was reluctant to undego colpocleisis surgery for that reason. Thus, SSLF under local anaesthesia was chosen as the remaining option.
SSLF shortened the hospital stay as colpocleisis would have done. The patient recovered well, and she was conscious during all the operation. Thus, there was no reason to observe the patient any longer to check her recovery. She had no pain or complications, such as hemorrhage, after the operation.
Conclusions
Because performing SSLF under local anesthesia was so successful in the current case, this procedure is being considered for future patients. Awareness of this possibility will increase the range of procedures that can be offered to these patients. SSLF generates lower costs because these operations are performed as outpatient surgery.
Footnotes
Disclosure Statement
There are no financial or other relationships that might lead to a conflict of interest for this article.