
Abstract
Abstract
Introduction
T
Case
A 19 year-old female adolescent presented to the outpatient department of obstetrics and gynecology with complaints of abdominal distention and pain in her abdomen for 2 months. She stated that her menstrual cycles were regular. A physical examination and radiologic studies, including ultrasound and a computed tomograph scan, revealed the presence of ascites, omental thickening (Fig. 1), and bilateral enlarged ovaries. Biochemical examinations showed that she had an elevated serum CA-125 level at 450 U/mL (normal range: 0–35 U/L), while other tumor markers—including α-fetoprotein (AFP) and β–human chorionic gonadotropin (β-hCG)—were within normal ranges. An ascitic tap was negative for malignant cells and a Mantoux test was also negative. A provisional diagnosis of ovarian cancer with omental deposits was made. The patient underwent a laprotomy, which revealed the presence of multiple nodules, measuring ∼1–2 cm, located on her intestine, omentum, and parietal peritoneum. Both of her ovaries were multicystic. Biopsy samples from the parietal peritoneum and the left ovary were sent for pathologic examination with frozen section. Frozen-section evaluation of her left ovary showed no malignancy. No further surgery was performed. Histopathologic examination of the specimens revealed multiple granulomas with epithelioid cells and caseous necrosis as well as multinucleated giant cells. The Ziehl–Neelsen stain for AFB was negative in her ascitic fluid and peritoneal tissue. Cultures for Mycobacterium species in her ascitic fluid and peritoneal biopsy were not performed.
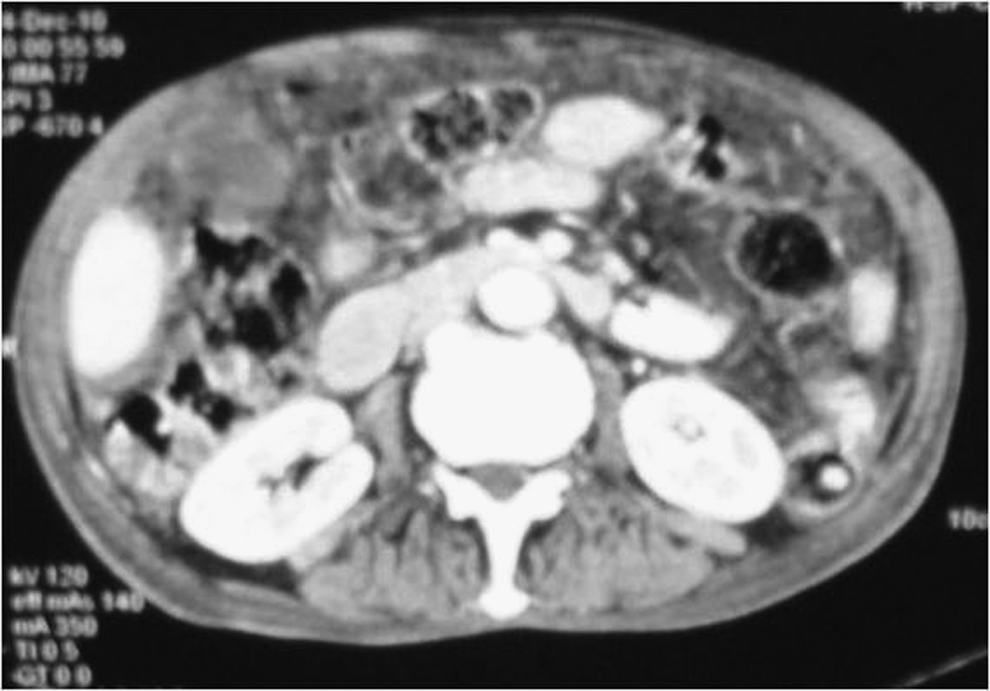
Abdominal computed tomography scan showing omental thickening.
Results
After assessing this patient's clinical features and histopathology results, and considering the high prevalence of TB in the Indian subcontinent, this patient was started on an antitubercular regimen (rifampicin, isoniazid, ethambutol, and pyrazinamide). These drugs were given to her three times per week. The patient's condition was reviewed after 2 months at a follow-up visit. She had improved dramatically. Her abdominal distension was reduced and radiologically only had minimal peritoneal ascites. Isoniazid and rifampicin were continued for an additional 4 months, 3 times per week, with pyridoxine given on an alternate day. On an additional follow-up 6 months later, this patient's CA-125 levels were within normal limits. When she visited the hospital after 8 months, she was asymptomatic and showed no signs of a recurrence.
Discussion
The annual incidence of TB is nearly 8 million people, with 2 million deaths worldwide. 1 The total disease burden in India is enormous, and it is estimated that >40% of the population is infected. The abdomen is a major extrapulmonary site for TB. It may involve the gastrointestinal tract, peritoneum, lymph nodes, or solid viscera, and constitutes up to 12% of extrapulmonary TB and 1%–3% of the total TB cases. 2 Yet, the protean clinical manifestations of abdominal TB continue to challenge the physician with respect to arriving at a correct diagnosis.
Differentiation between abdominal TB and malignancy may be even more difficult. Abdominal distension, abdominal pain, abdominal mass, and weight loss are common symptoms. Abdominal TB is associated with omental thickening, mesenteric lymphadenopathy, pelvic or tubo-ovarian masses, ascites, and elevation of CA-125 levels in serum and ascitic fluid. Ascitic fluid examination reveals an exudate with lymphocyte predominance. Yields from TB smears and cultures remain very low. Tuberculin skin testing has limited usefulness in high-prevalence areas, and a negative skin test may be seen in many patients with histologically confirmed abdominal TB. 3
Differential diagnoses of granulomatous disease include sarcoidosis, Wegner's granulomatosis, Churg-Strauss granulomatosis, histoplasmosis, and Crohn's disease. Patients with histoplasmosis, Churg-Strauss granulomatosis, and sarcoidosis present mainly with pulmonary symptoms. However, the differential diagnosis of intestinal TB with Crohn's disease is difficult. Crohn's disease involves the intestinal wall with formation of ulceration and fistulae and rarely involves the peritoneum.
Although culturing for Mycobacterium species in ascitic fluid and peritoneal biopsy is the “gold standard” for diagnosis, results are not obtained until 4–6 weeks later, which may increase the mortality rate of whatever disease is present. Chow et al. reviewed 60 patients with TB peritonitis within 12 years and reported a mortality rate of 53%, and 84% of those patients had died within 6 weeks of presentation, often before the results of the mycobacterial culture were available. 4
The cancer antigen–125 (usually written as CA-125) is a high molecular–mass glycoprotein produced both by ovarian cancer cells as also by normal cells of tissues derived from the coelomic epithelium. Serum CA-125 levels are used as a marker of tumor activity in patients known to have ovarian carcinoma. In women with histologically proven ovarian carcinoma, levels of serum CA-125 are elevated >35 U/mL in >80% of cases. 5
However, elevation of CA-125 levels may occur in malignant conditions other than ovarian cancer, in benign diseases, and in 1%–2% of normal healthy individuals.
Kalantri et al. studied CA-125 levels in pleural effusion and ascitic fluid. In that study, all patients with ascites and 70% of patients with pleural effusion had elevation of this tumor marker in their body fluids, when the etiology was tuberculous or pyogenic. 6
Elevation of CA125 in peritoneal TB has been reported and misinterpreted as disseminated ovarian malignancy. 7 Although sensitivity of CA125 is high, its specificity is poor. 8 Elevated levels in a clinical situation involving ovarian carcinoma must be considered with caution to avoid unnecessary laparotomies and even extensive surgical resection of pelvic masses. Thus, it is evident from the current case that an elevated CA-125 level can be useful when considering the presence of a nonmalignant condition such as TB, especially in the Indian subcontinent—and this marker can also be used to assess response to treatment and as an indicator of the activity of a disease such as TB.
A decline of CA-125 with antitubercular drug therapy has paralleled clinical improvement and has been advocated as a marker in the follow-up of response to treatment.9,10
Conclusions
TB peritonitis should be considered in the differential diagnosis of patients with ascites and elevated serum CA-125. This marker may be useful for monitoring treatment response. This observation should help clinicians to entertain a possible diagnosis of abdominopelvic tuberculosis and undertake diagnostic laparoscopy, thus avoiding laparotomy where possible. It is suggested that all women who present with adnexal or abdominopelvic mass and/or ascites be tested for CA 125; raised levels may not be caused by ovarian malignancy but could be the result of TB.
Footnotes
Disclosure Statement
No competing financial conflicts exist.