
Abstract
Abstract
Introduction
H
Review of Literature
Heterotopic cartilage in the uterus was first described by Neumann in 1925 when he found small focus of cartilage within the endometrium of a 27-year-old lady who underwent hysterectomy for pelvic inflammatory disease. He theorized that the cartilage had originated by differentiation of sclerotome germ carried along by the migrating Wolffian duct during embryonic development. A similar theory was proposed by Meyer in 1901 when he found a piece of bone contiguous with the Wolffian duct in the lateral wall of the cervix of a 14-cm fetus. 2 Table 1 demonstrates the history of patients that we find in the literature.1–3 As the table depicts, the whole story establishes three possible methods of development of this heterotopic cartilage, that is, retained fetal tissue, heteroplasia, and metaplasia. Retained fetal tissue is considered as a cause of osseous metaplasia,4,5 and fetal cartilage is also known to have persisted within the endometrium for months and over years following an abortion. 2 The review of literature also reports cases where a retained fetal tissue was labeled behind the presence of heterotopic cartilage (21st and 26th case of Table 1).
Case Report
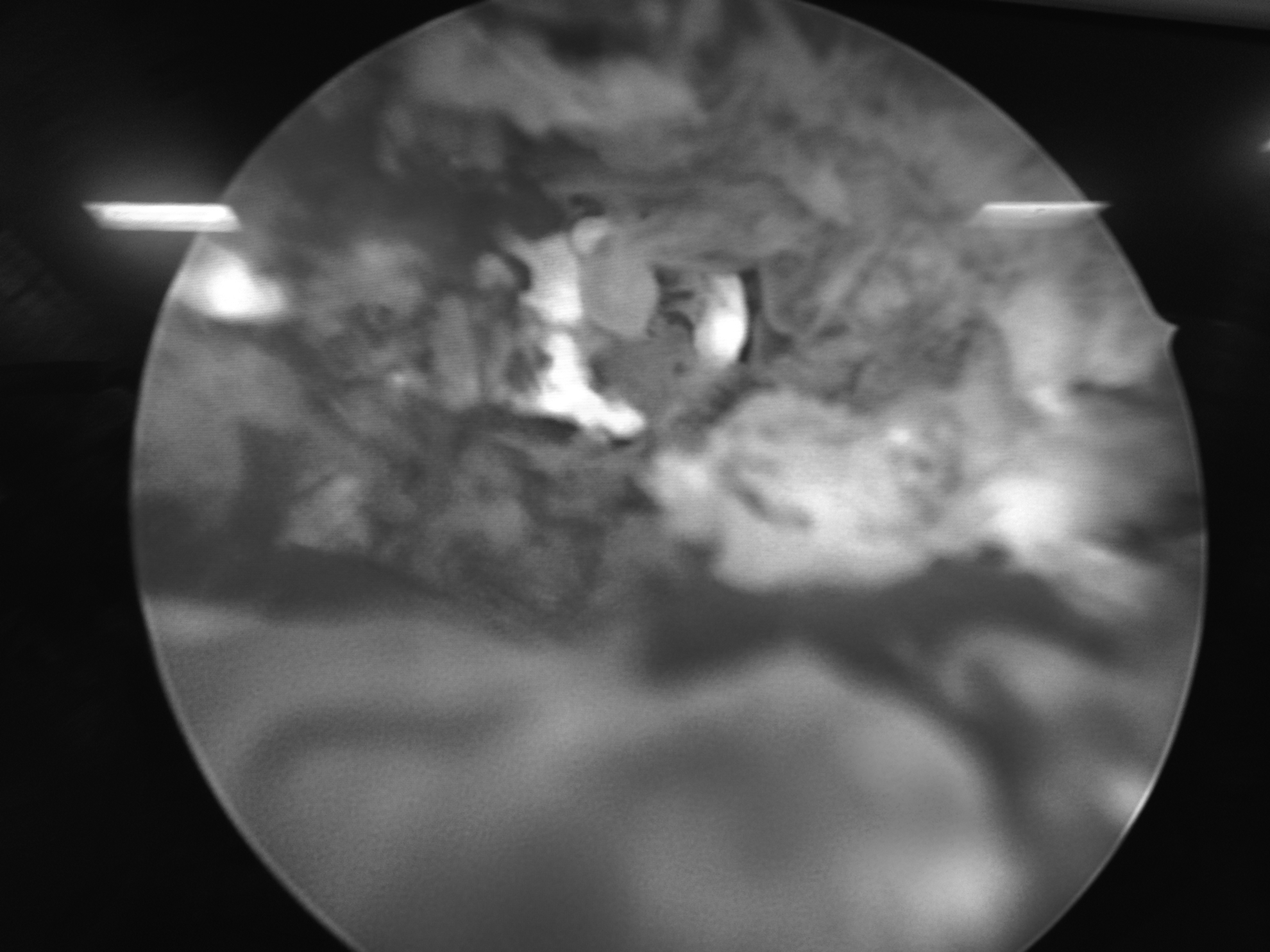
A 21-year-old female reported in the gynecology outpatient department of a tertiary healthcare center with complaints of irregular cycles and primary infertility. She was married for 2 years and cohabiting with her husband for 8 months. She attained menarche at the age of 13 and had regular cycles at the interval of 24–30 days for 4–5 days. However, since 1 year, her cycles were prolonged and the flow was decreased. She menstruates for 1–2 days at the interval of 2–3 months and the amount of flow was significantly decreased. On vaginal examination, she had a normal cervix and vagina, as well as a normal-size uterus, with no associated tenderness or adnexal mass. Considering genital tuberculosis and polycystic ovarian disease as differentials, she was investigated. On investigation, her complete blood count, erythrocyte sedimentation rate, thyroid profile, serum prolactin, follicle-stimulating hormone, and luteinizing hormone were normal. Ultrasonography revealed a normal uterus with multiple thin echogenic foci of 2.3–0.5 cm size in the endometrium having no flow on color Doppler. Her bilateral ovaries were studded with cysts in the periphery and ovarian volume on the right side was 13.5 cc and left side was 11.5 cc. In view of these findings, the differentials suspected include calcified focus or tubercular endometritis with the possibility of polycystic ovaries. A premenstrual diagnostic hysteroscopy and, simultaneously, an endometrial biopsy were planned for confirmation of diagnosis. On hysteroscopy, the endometrial cavity was full with stone-like calcified tissue along with the normal endometrium in between (Fig. 1). This calcified tissue was removed hysteroscopically and endometrial tissue sent for histopathological examination. Figure 2 demonstrates the uterine cavity after evacuation. Histopathological examination revealed a secretory endometrium with cartilaginous metaplasia of the endometrium (Fig. 3).

Hysteroscopic view of uterine cavity.

Cartilaginous tissue removed from the uterus.

Histopathological view of secretory endometrium with cartilage on the left side.
Discussion
The presence of cartilage in the uterine cavity is termed as heterotopic cartilage 2 and is a rare entity in cases of primary infertility. A review of literature shows that only two cases are there where heterotopic cartilage is reported in nulligravida females. 2 Literature is still searching for a definitive uniquobiaus process of its origin in the uterus. Heteroplasia is the development of embryonically displaced mesodermal cell rest already predestined to form cartilage and is described as a pathological process for heterotopic cartilage. Why heteroplasia occurs only in the reproductive age group or are there some hormonal levels that stimulate this process is yet to be cleared. Analysis of all the case reports suggests that all the patients were of reproductive age group, including the present patient. Retention of fetal cartilage is rejected as an explanation in our patient as she is nulligravida. Metaplasia is still a matter of investigation and the role of hormones could not be denied. Metaplasia is a physiologic process in response to infection, genital tuberculosis, and foreign body reaction. The endometrial gland and stroma are subjected to a variety of metaplastic changes like squamous metaplasia, ciliated metaplasia, papillary metaplasia, intestinal metaplasia, and sometimes stromal metaplasia. This includes the formation within the endometrial stroma of islands of smooth muscle, cartilage, and bone. The review of literature revealed metaplasia as the prime culprit. In view of low socioeconomic status, poor availability of health facilities, and high incidence of neglected genital infections, chances of metaplasia are high in our population and seems to be the most logical explanation for this patient. Menstrual irregularity, bleeding, infertility, and subfertility are common symptoms evident in the literature, but it can be an incidental finding as reported in many cases shown in Table 1. In view of its noninvasive nature and easy availability, ultrasonography is usually the first investigation modality a female is subjected to for genital pathology, the same for this patient also. After ultrasonography, hysteroscopic visualization and guided excision is the treatment of choice and no case of recurrence is reported till date.6,7 Prognosis is good after treatment as there are no cases of recurrence, and case reports of successful pregnancy are there. The present patient is on follow-up.
Conclusion
Heterotopic cartilage of uterus is a rare finding. Strong clinical suspicion and a vigilant radiologist are the key to diagnose it. Hysteroscopy is a wonder tool for the confirmation and excision of lesions (Fig. 4).
Postresection hysteroscopic view of uterine cavity.
Footnotes
Disclosure Statement
No competing financial interests exist.