
Abstract
Abstract
Introduction
M
Case
A 23-year-old caucasian female, gravida 0, para 0, was referred to the gynecology oncology unit with fever, malaise, lower abdominal pain, and distension. During a physical examination a palpable mass was found in the lower abdomen. Ultrasound (US) examination revealed a solid mass with a few cystic areas, 12×8 cm in size, that was located on the left side of the uterus, arising from the left ovary. The patient's medical and family history was unremarkable. Laboratory tests showed that the initial value of AFP was 1210 mcg/L, lactate dehydrogenase (LDH) was 503 U/mL, CA-125 was 48 U/mL, and β–human chorionic gonadotropin was negative. A laparatomy revealed a mass with a smooth surface originating from the left ovary, measuring 10 cm in diameter. The right adnexa were normal. A left salpingo-oophorectomy was performed with an omentectomy and multiple biopsies of the pelvic and abdominal peritoneum. A routine biopsy of the right ovary was also conducted. Malignant signs were found on frozen sections of the mass that was excised during this surgery. Abdominal lavage fluid submitted for cytologic examination was negative for malignancy. Gross examination of what was suspected to be one tumor in the ovary revealed that there were actually two tumors. The smaller one, measuring 5 cm in diameter, showed histologic features of a mature teratoma (Fig. 1). The larger tumor, measuring 10 cm in diameter, was partly necrotic, with hemorrhage and pseudocystic areas. Histologically, this tumor was composed of atypical polymorphic cells arranged in microcystic patern with “hobnail” formations as well as a solid pattern with numerous Periodic Acid-Schiff–positive, diastase-resistant globules. An endodermal sinus pattern and numerous glomeruloid bodies were also found (Fig. 2). In the resected part of the omentum, a small focus of this tumor was present, measuring 1 cm in diameter.
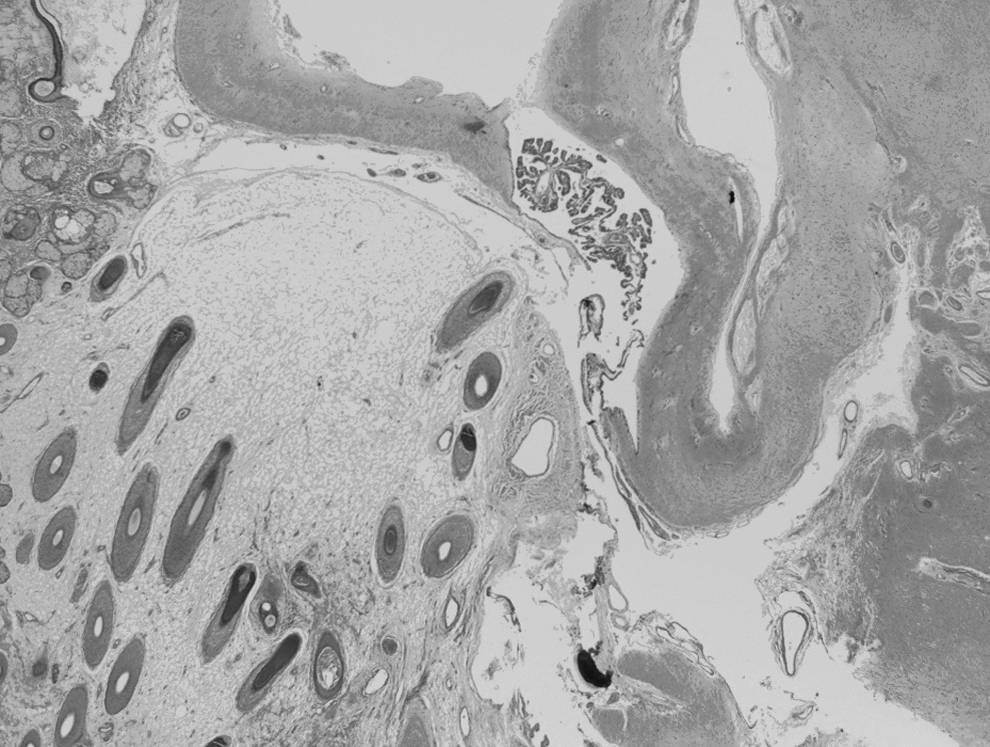
Mature cystic teratoma with appendages of dermis and mature glial tissue. (H&E×200).

Yolk-sac tumor with endodermal (Schiller-Duval) sinuses. (H&E×400).
Results
This patient's postoperative course was uneventful. She received three courses of a bleomycin–etoposide–cisplatin (BEP) regimen, given at 21-day intervals as adjuvant chemotherapy.
During the first 6 months of follow-up, her AFP levels were checked every 2 weeks and had declined from an initial 1210 mcg/L to 3.4 mcg/L. Computed tomography scanning was performed 3 months after her initial surgery and the results were unremarkable. Four months after chemotherapy the patient had regular menstrual cycles. She conceived 2 years after surgery and delivered a 3040-g, 48-cm long, healthy male neonate, by vaginal delivery at 38 weeks of gestation. Prenatal diagnostics were not performed during her pregnancy. Eleven years after surgery and polychemotherapy, with regular clinical and laboratory testing (CA-125, AFP), no signs or symptoms of primary malignant disease had been found.
Discussion
YSTs of the ovary are relatively uncommon neoplasms, occurring in the prime of life, that are characterized by a high potential for malignancy but also by high chemosensitivity. 4 The principal goal in surgical management of a YST is to achieve appropriate cytoreduction with adequate surgical staging because surgical residue is an independent prognostic factor. 5 A unilateral salpingo-oophorectomy with preservation of the contralateral ovary and the uterus is now considered to be the appropriate surgical treatment for a patient with a YST during the reproductive years. Even in patients with advanced disease, preservation of reproductive function is possible, particularly, if the contralateral ovary is normal. 6 Peritoneal washing, omentectomy, and multiple peritoneal and abdominal biopsies should be performed as part of the surgical staging procedure. Sampling of retroperitoneal lymph nodes is unnecessary because this does not have an effect on 5-year survival rates.
In the current case, pathologic examination revealed the presence of metastatic foci of YST in the resected part of the omentum. In accordance with that finding, the disease was classified as International Federation of Gynecology and Obstetrics (FIGO) stage III. Given the high sensitivity of YSTs to chemotherapy, even in cases of advanced disease, fertility-sparing surgery can be carried out safely. Nawa et al. showed, in a study based on 47 patients who had surgery for YST, that there was no significant difference in 5-year survival rates between the patients with conservative and those with radical treatment. 7
Pathologic examination of biopsies taken from the current patient's contralateral ovary showed healthy ovarian tissue. However, bilateral involment in case of YST is rare; therefore, routine biopsy of the contralateral ovary should be avoided to prevent secondary infertility related to adhesions or ovarian failure. 8 The current patient responded well to adjuvant chemotherapy, making further surgical treatment unnecessary. Regardless of the stage of disease, conservative surgery with adequate cytoreduction is recommended for patients of reproductive age. This approach should be followed by a minimum of three courses of BEP chemotherapy. As far back as 2008, a study showed that a cumulative high-dose of the BEP regimen has little effect on menstrual cycles and does not cause significant impairment of ovarian function. 9 de La Motte Rouge et al. showed that 40 of 41 women who underwent fertility-sparing surgery for YSTs and received adjuvant BEP remained potentially fertile, and pregnancy was achieved in 12 of 16 (75%) women who attempted conception. 10
An important parameter for diagnosis and long-run follow-up includes regular measurement of serum AFP levels. The patient, in the current case, concieved 24 months after completion of treatment. During pregnancy, her AFP levels were within normal range and she was able to go through her pregnancy with no complications. Clinical and laboratory testing during the follow-up period showed that there was no relapse of the primary disease.
Conclusions
YST, as described in this case, occurs rarely and has high malignant potential. Because of this tumor's characteristics, the current authors recommend a multidisciplinary treatment approach, bearing in mind the importance of preservation of the patient's reproductive ability.
Footnotes
Disclosure Statement
No competing financial conflicts exist.