
Abstract
Abstract
Introduction
V
The presentation can be rapid after injury and spontaneous rupture of an artery, or delayed secondary to pressure necrosis and subsequent vessel rupture. The vasculature may commonly develop varicosities during pregnancy, especially in parous women, because of increased venous pressure created by the increasing weight of the uterus. This article presents a case of spontaneous vulvar swelling of 15 weeks' duration during pregnancy with an unusual presentation as a vulvar hematoma. To the current authors' knowledge, this is the second case described in the literature.
Case
The patient was a 32-year-old Japanese woman, multigravida, with a spontaneous bilateral vulvar hematoma. Her gynecologic and medical histories were uneventful. The patient noticed that she had cystic swellings (3–4 cm) on the bilateral vulva, but had no preceding traumatic event at 10 weeks' gestation. She had no history of coagulopathy or athelosclerosis. The mass size seemed to increase slowly but this was uneventful until the 25th week of her pregnancy.
The patient came to us with pain and swelling in her bilateral labia region. On examination, she was noted to be hemodynamically stable. There was an obvious vulvar hematoma significantly distorting the anatomy, along with redness but no laceration. Magnetic resonance imaging of the pelvis showed a cystic region with lower signal intensity in the left vulvar area (5×5 cm) and a multicystic lesion with relatively higher signal intensity in the right vulvar area (4×5 cm; Fig. 1). These lesions were suspected to be hematomas without extravasation of blood and active bleeding. When the left hematoma capsule was opened, about 80 g of clotted blood was drained (Fig. 1). The vulvar hematoma was evacuated, and the dead space was obliterated with purse-string sutures with Vicryl 2-0, leaving a drain in situ to drain the dependent area. Her right vulvar hematoma similarly resolved after incision and drainage.
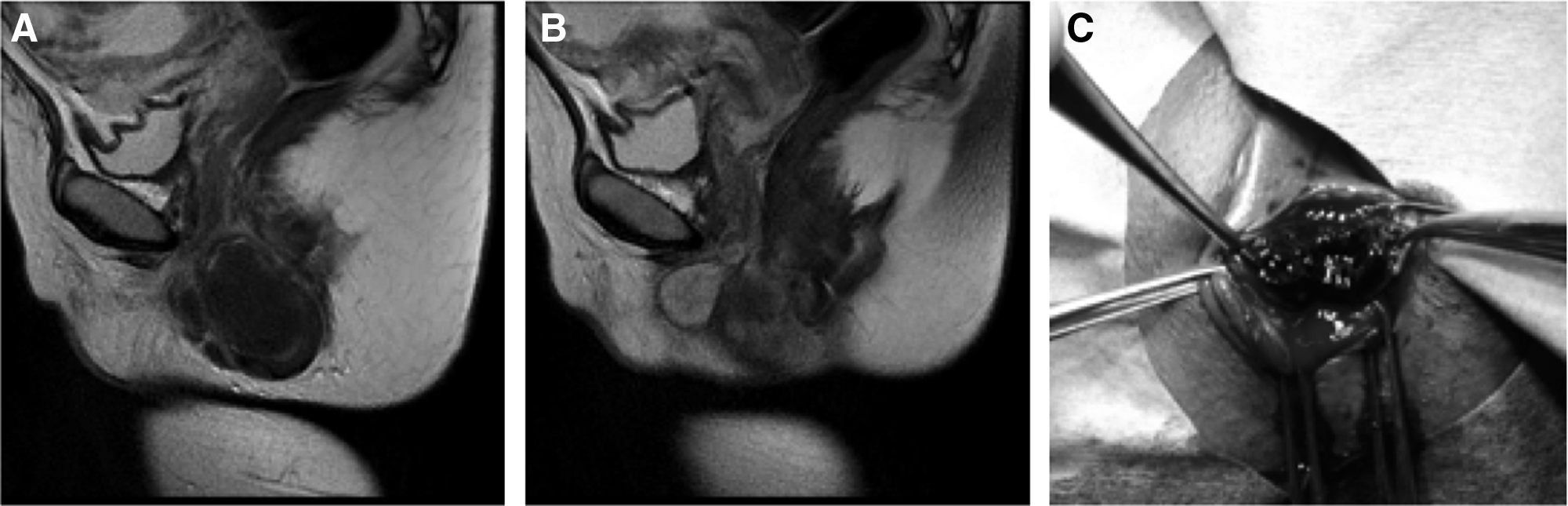
Sagittal T2-weighted magnetic resonance images show the hematomas on the left
Results
There was no indication of further vulvar swelling. The course of this patient's pregnancy and fetal growth, monitored with a 3–4-weekly obstetric examination, was uneventful, resulting in an uneventful vaginal delivery 13 weeks later.
Discussion
The vulva consists of elastin fibers, smooth-muscle fibers, and connective tissue with many vessels, and is primarily supplied by the pudendal artery, a branch of the anterior division of the internal iliac artery that divides into the inferior rectal artery, posterior labial artery, and transverse perineal branches. 5 Although trauma is the major preceding cause, spontaneous vessel rupture is considered in the absence of evidence at examination of a patient with such a hematoma. Spontaneous rupture of the pudendal artery can occur exclusively at the site of an aneurysm and is generally related to atherosclerosis.1,2 Infection or connective-tissue disease is rarely identified but can occasionally cause aneurysms. The vasculature may commonly develop varicosities during pregnancy, especially in parous women because of increased venous pressure created by the increasing weight of the uterus. The bleeding can be venous in origin and often develop slowly. 6
Nelson et al. 7 reported a case of a spontaneous 6-cm vulvar hematoma that presented as unexplained vulvar edema in a 35 weeks' pregnant woman. She presented to the obstetrics triage unit with rapid-onset unilateral vulvar swelling and no preceding traumatic event. After incision and drainage of the hematoma, her edema resolved and the patient went on to have an uneventful vaginal delivery 4 weeks later. The current case presented with bilateral vulvar swelling and rapid-onset pain. Fifteen weeks prior, she had found a 3–4-cm cystic mass on the bilateral labium. This patient was treated successfully with surgical evacuation of hematoma clots and went on to have an uneventful vaginal delivery 13 weeks later.
The management of a vulval hematoma during pregnancy is somewhat controversial. 8 The hematoma itself may be managed conservatively or surgically. Against postpartum bleeding or nonobstetric hematoma, advanced selective angiography embolization can be used as an effective alternative to surgery for hemorrhage.1,3 It is generally agreed that, if the hematoma is significantly larger or expanding, intervention is required.2,8 Surgery involves an incision and evacuation of the hematoma with ligation of any bleeding points. As the source of bleeding is often venous, ligation is not always possible. However, evacuation of the clot is important to prevent pressure necrosis and infection.2,8
Selective embolization has been used in obstetrics and gynecology to treat neoplastic disease of the genital tract, trauma to the pelvis, postpartum hemorrhage, and bleeding from unknown origins without causing complications.3,9
Conclusions
Incision and evacuation of the hematoma clot may be the best intervention option for pregnant patients. Blood-clot evacuation and ligation of bleeding points with surgery may be performed to prevent necrosis and infection.
Footnotes
Disclosure Statement
The authors have no potential conflict of interest to disclose.