
Abstract
Abstract
Introduction
E
Case
A 40-year-old woman presented with a 3-day history of nausea, vomiting, and constipation. She had been evaluated on an outpatient basis because of intermittent digestive discomfort over the previous year, and, as a part of this assessment, she had undergone gastrointestinal endoscopy, revealing no findings of interest. The patient reported symptoms indicative of previous intestinal obstruction resembling the current episode, although the earlier episode was less severe and had resolved spontaneously 3 months before the patient presented to the Fundacion Jiménez emergency department. When she arrived at the emergency department she was in stable condition and afebrile, presenting with abdominal distension and a tympanic abdomen, but there were no signs of peritoneal irritation. An abdominal ultrasound revealed distension of the small bowel and increased peristalsis and intra-abdominal fluid. Based on these findings, a computed tomography (CT) scan was obtained, revealing a mass of 34×32 mm in the terminal ileum adjacent to the ileocecal valve as well as the locoregional lymph nodes, and substantial proximal dilatation of the small bowel (Fig. 1).

Abdominal computed tomography scan showing the patient's tumor and dilated intestine.
Given that there was suspicion of an inflammatory mass contrasting with a tumoral mass in the cecal pole, emergency surgery was performed on this patient. An exploratory laparotomy revealed an inflammatory mass in the right iliac fossa. The center of the growth contained what appeared to be a tumor of the cecum, measuring ∼5 cm in diameter, located very near the ileocecal valve as well as apparently pathologic lymph nodes along the ileocecal artery chain. The clinical impression suggested a malignant mass formation in the right colon. This indication, coupled with oncologic criteria, led to a decision to perform a right hemicolectomy.
Results
Following surgery, the course of the patient was favorable, and, on the sixth day following surgery, the patient's symptoms were in remission and she was discharged to go home.
Histopathologic examination showed multiple foci of the endometrial tissue primarily on the muscle layer and serous layer of the colon, and a few submucosal nodes (Fig. 2). The lymph nodes showed reactive changes; 2 of these nodes had miscroscopic subcapsular foci of endometriosis (Fig. 3).
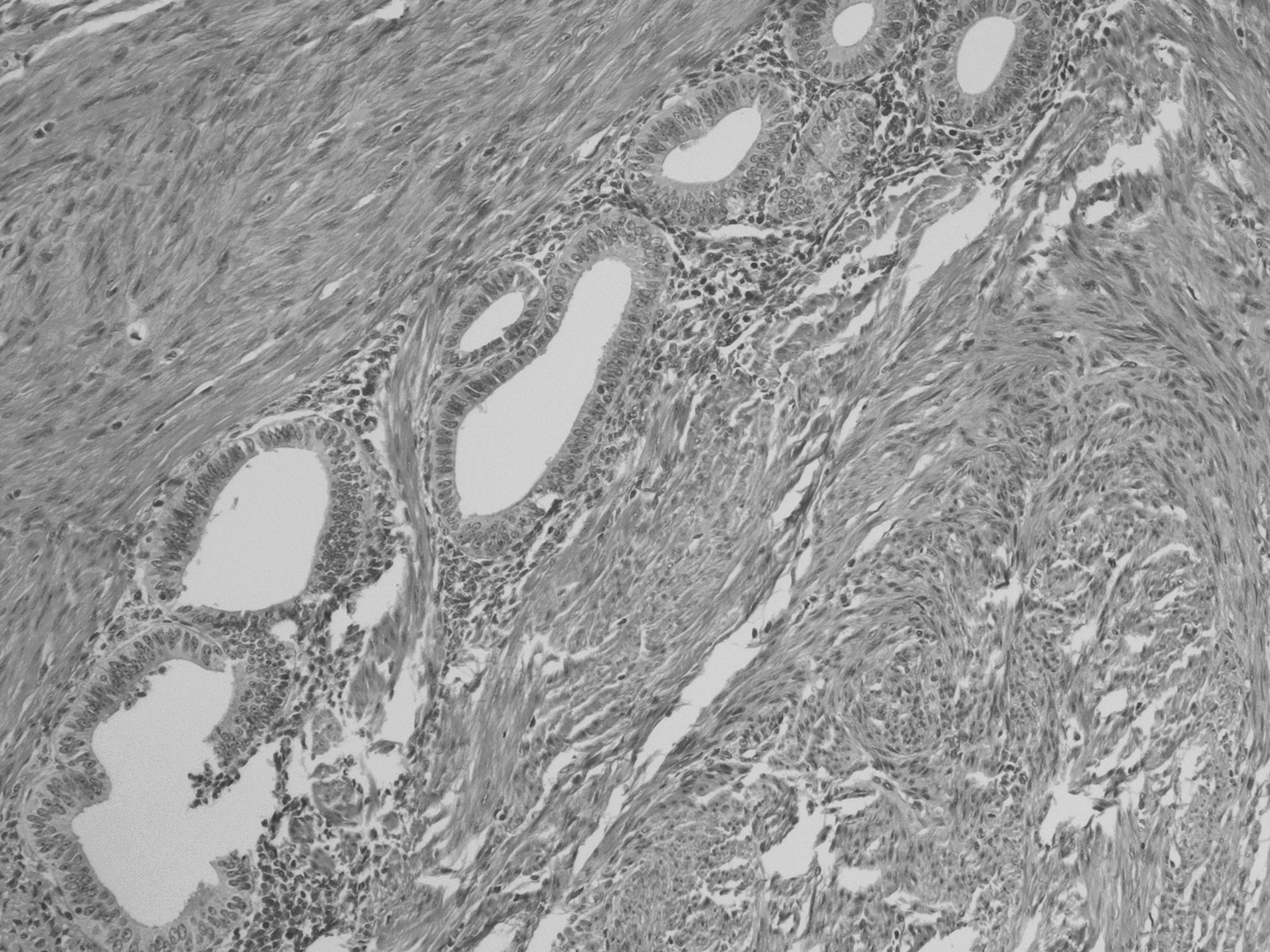
Endometriosis tissue on the intestine.

Endometriosis tissue on a lymphatic node.
Discussion
Endometriosis is a common gynecologic finding that is chronic, benign, estrogen-dependent, and associated with infertility. The primary clinical manifestations of the disease are pelvic pain, dysmenorrhea, and dyspareunia. 2 Other symptoms that have been described in this disease include diffuse abdominal pain, rectal pain, nausea, vomiting, diarrhea, tenesmus, bleeding of the lower digestive tract, and constipation. 3 The appearance of endometriosis in extragenital sites is not rare, representing between 3% and 37% of all cases. 4 Of these nongenital sites, the intestines are the most common (3%–12% of women with endometriosis), with the rectosigmoid colon representing the most common site (70%–90% of all cases affecting the digestive system), followed by the ileocecal area, the appendix, and, more rarely, other segments of the intestines. 5
Diagnosis is relatively straightforward, especially in the case of florid endometriosis of the pelvis; however, diagnosis is quite complicated when the patient presents with acute intestinal obstruction, because the comparative rarity of the manifestation may initially cause clinicians to overlook the presence of this pathology. 3 Diagnosis is primarily clinical, although additional examinations are necessary for confirmation. Gynecologic ultrasonography contributes little to definitive and causal diagnosis of abdominal obstruction secondary to endometriosis. 6 Magnetic resonance imaging (MRI) provides greater specificity and sensitivity than CT, although not all emergency departments have access to MRI technology, in which case, CT—which is much more commonly available—may be used. Laparoscopy, the “gold standard” for diagnosis of the disease, may be used to confirm the diagnosis by obtaining samples for histopathologic study and to determine the degree of severity and disease extension. 7 In cases of suspected endometriosis with involvement of the ileocecal valve and the small intestine, diagnostic laparoscopy must cover the entire intestinal tract.
Many emergency situations—often caused by acute obstruction—call for greater use of contrast-enhanced CT and, if the availability of technical means and the state of the patient permit, colonoscopy is beneficial. 8 The most common causes of small-intestine obstruction in the presence of endometriosis are stenosis of the affected segment, intussusception, and intestinal volvulus secondary to adhesions. 9 Therefore, surgical exploration—if possible, using laparoscopy—should play a substantial role when diagnosing and treating the disease.
While theories attempting to explain the spread of endometriosis are varied and range from causes, such as retrograde menstruation, haematogenous spread, to spread through the lymph system, the latter is a classical, rare finding, and to the current authors' knowledge—compared with the total incidence of extragenital endometriosis—the published cases of lymphatic involvement are the exception rather than the rule.1,10–14 For this reason, the current authors believe that the case of the current patient might be of extraordinary interest.
However, this perception of a this occurrence being benign lesion is changing in more recent years because of the findings of genetic and molecular proofs of endometrial tissue dissemination through lymph nodes.15,16 Some researchers have found an 11%–42.3% lymph-node involvement in patients with pelvic endometriosis, when these researchers performed laparoscopic resections. 17 Moreover, there is evidence of differences in immune responses and the presence of endometrial stromal cells in the pelvic lymph nodes between healthy and endometriosis-affected women. 18
Conclusions
Although the physiopathology of the spread of endometriotic foci has yet to be clarified in the literature, spread through the lymph system cannot be ruled out as one of the mechanisms contributing to this long-distance dissemination. Although this has been the exception rather than the rule, cases have been described in which viable endometrial tissue has been found in the lymph nodes of affected areas and, in more recent years, increasing evidence of the lymph nodes involvement is being published.
Footnotes
Acknowledgments
All the authors made significant contributions to the treatment of the patient and contributed in preparing this article. Drs. Vasquez, Fidalgo, and Vorwald participated in the surgical treatment of the patient, and conducted postoperative evaluations. Dr. Arambarri was the pathologist in charge of evaluated the surgical specimen.
Disclosure Statement
All the authors declare no conflict of interest in the present publication, including any commercial relation with the present article.