
Abstract
Abstract
Introduction
A
Case
A 32-year-old primigravida female was referred to the Postgraduate Institute of Medical Sciences, in Haryana, India, at 36 weeks of gestation with polyhydramnios and intrauterine growth restriction. Her blood pressure and other routine obstetric testing results, including urine protein and sugar levels, were normal. Ultrasound imaging revealed a singleton fetus with subcutaneous edema, moderate pericardial effusion, ascites, polyhydramnios, and a bulky placenta with a placental tumor showing a hypoechoic image with increased Doppler flow. At 37 weeks of gestation, there was a premature rupture of the membrane and preterm labor resulting in severe fetal distress and intrauterine death of the fetus.
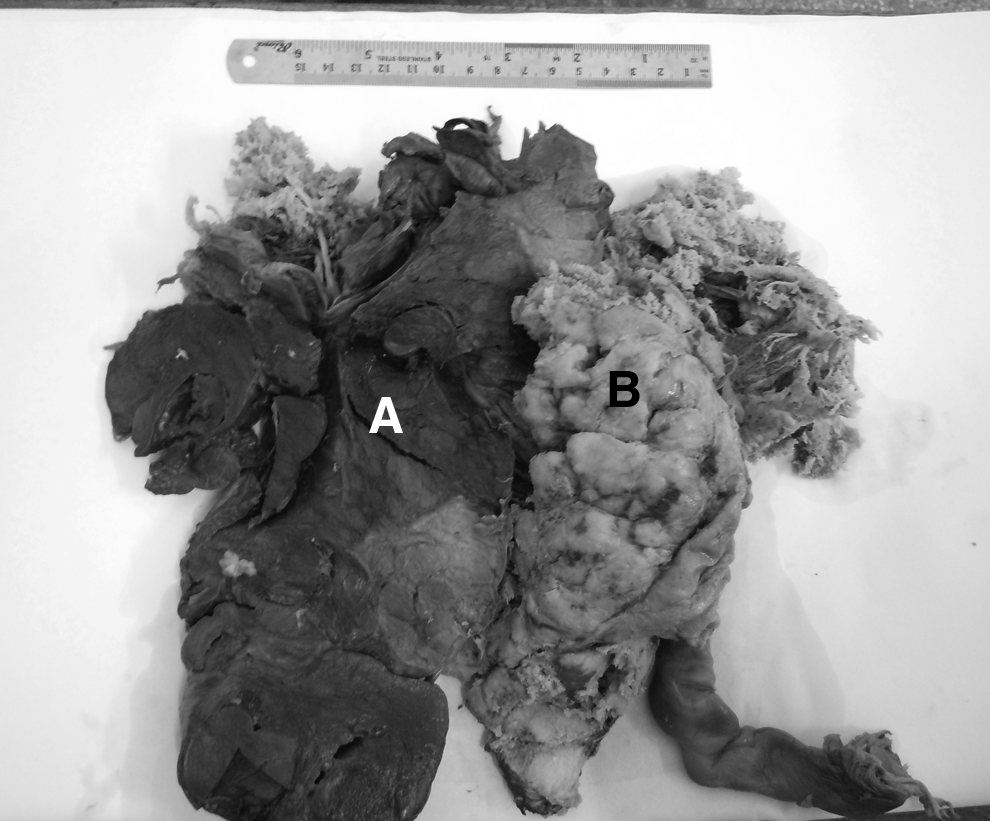
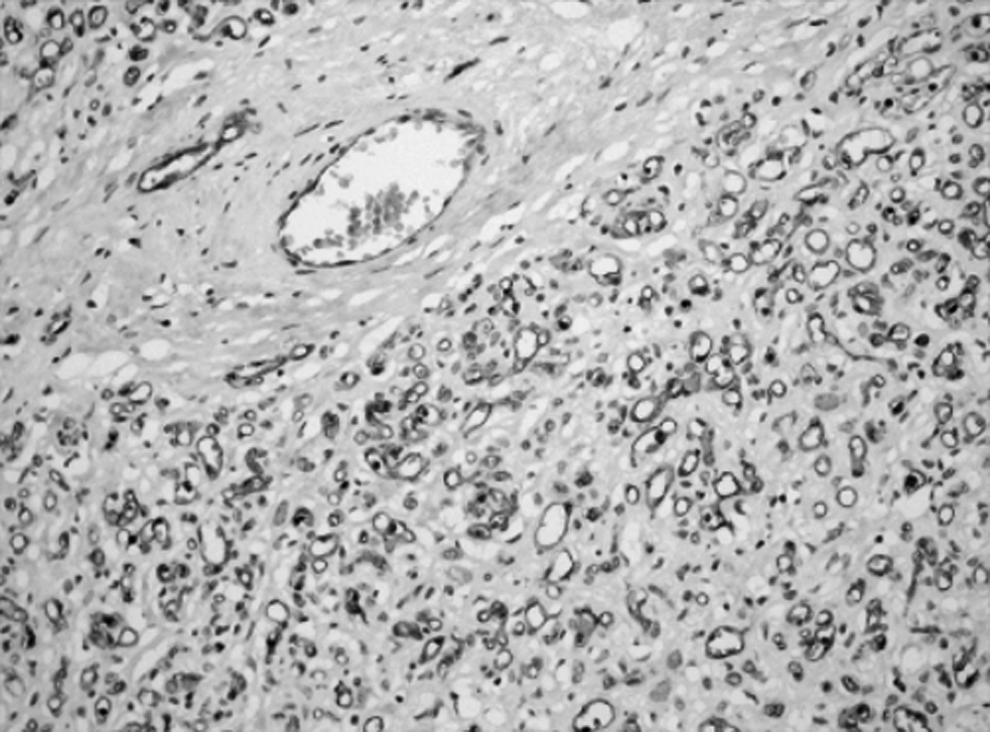
Grossly, the placenta weighed 760 g and measured 22×20×6 cm with a centrally attached umbilical cord 25 cm long. A large solitary lobular mass was noted on the fetal side of the placenta, measuring 15×10×7 cm. The cut surface was fleshy, congested, dark red–tan in color, and firm in consistency (Fig. 1AB). Microscopically, the chorionic villi were regular in shape, with fibrovascular stroma and the presence of syncytiocapillary membranes in terminal villi, which were lined with a single layer of trophoblastic tissue. On gross examination, as well as microscopically, the umbilical cord and amniotic membranes were unremarkable. Microscopically, the chorangioma was shown to have numerous proliferative blood vessels in various stages of differentiation, including endotheliomatous, capillary, and cavernous in hyalinized and fibrous stroma (Fig. 2A, B). These histologic features were consistent with a chorangioma.
Large solitary lobular chorangioma

Immunohistochemistry testing revealed variable reactivity of endothelial cells to CD34 (Fig. 3). The capillary angioblastoma showed no reactivity to CD34, while weak reactivity was observed in capillary buds and immature capillaries. The endothelial cells of well-formed mature capillaries showed strong reactivity for CD 34. The Ki-67 proliferation index was 8%.
Variable reactivity of endothelial cells to CD34 (200 ×, IHC).
Results
The patient herself delivered a placenta and deceased fetus without surgical intervention. The patient responded well after treatment.
Discussion
The chorangioma has been referred to as a hamartomalike, or hyperplastic capillary lesion, rather than a true neoplasm. 5 The occurrence of a chorangioma is high in patients at high altitudes. 6 These tumors are often found in primipara and twin pregnancies. Risk factors associated with the occurrence of chorangioma include women >30 years' old, women with diabetes, and women who have hypertension. 7 The chorangioma is most frequently observed in the third—and less frequently in the second—trimester of pregnancy as a solitary nodule or, less frequently, as multiple nodules. This tumor is most frequently found on the fetal surface of the placenta, often in the vicinity of the umbilical cord insertion into the placenta, with larger tumors being usually attached to the chorion.
Given that the chorangioma is classified as a hemangioma, its histologic appearance is pleomorphic. The tumor could be divided into endotheliomatous, capillarious, cavernous, and fibromatous forms, among which the capillarious form is the most common of all chorangiomas. Chorangiomas probably arise as malformations of the primitive angioblastic tissue of the early placenta. 8
This tumor's differentials include chorangiosis, localized chorangiomatosis, diffuse multifocal chorangiomatosis and subamniotic hematoma, subchorial thrombohematoma, partial mole, fibroid tumor, and teratoma. Chorangiosis includes a diffuse increase in terminal villi capillaries that is associated with diabetes and placental overgrowth syndromes. Chorangiomatosis shows permeated normal villi instead of an expansile lesion. Localized chorangiomatosis is associated with hypoxia and ischemia, and the tumors are found concurrently with preeclampsia, and multiple gestations. Diffuse chorangiomatosis is associated with extreme prematurity (<32 weeks), congenital malformations, avascular villi, and placentomegaly. 9
Chorangiomas can be detected prenatally by simple noninvasive investigation techniques. Ultrasound imagine can be used to detect the presence of a tumor as a hypoechoic mass near the chorionic plate or umbilical cord insertion. Degenerative changes will appear as heterogenous areas on the scan. Vascularization in the tumor can be detected by color Doppler imaging, thereby differentiating a vascular tumor from ahematoma. 10 There is also significant role for magnetic resonance imaging (MRI) in the detection of chorangioma. 11
The clinical significance of chorangioma is size-dependent; small chorangioma have no clinical significance. A chorangioma >5 cm or multiple chorangiomas are associated with polyhydramnios, hemorrhage, premature delivery, premature placental separation, or placenta previa. This tumor may result in severe fetal distress, intrauterine death, or nonimmune hydrops fetalis. Anemia, thrombocytopenia, or congestive cardiac failure may be seen in a neonate. 8
Large chorangiomas can result in fetal mortality in 30% of cases, while occurrence of polyhydramnios has a variable frequency of 14%–28%. 5 A chorangioma presents as physiologic “dead space,” thereby compromising the fetus' blood supply, leading to chronic hypoxia, and finally resulting in fetal growth restriction and the intrauterine death of the fetus. 5 This explains the fetal distress and the intrauterine death of the fetus in the current case.
Therefore, chorangiomas cannot be overlooked, as they have a significant impact on the outcome, which can include serious problems for the developing fetus and the mother. Appropriate management should be implemented as soon as possible. If the fetus is mature, delivery should be planned and performed. An intrauterine transfusion can relieve fetal anemia, but this is temporary and repeated transfusions are required. Amniodrainage can provide relief from polyhydramnios. All of these procedures only alleviate the symptoms; the primary pathology should be taken care of simultaneously, although small chorangiomas may not need treatment. Large chorangioma can be treated in several ways, including endoscopic devascularization, alcoholic ablation, and interstitial laser coagulation. 8
Conclusions
Examination of the placenta is crucial in complicated pregnancies for identifying chorangiomas. The pathophysiology and pathogenesis of various feto–maternal complications can be accounted by this biologically indolent entity. Antenatal diagnosis and treatment can reduce fetal morbidity and mortality. Ultrasound and colour Doppler imaging can play pivotal roles in diagnosis of chorangiomas.
Footnotes
Disclosure Statement
No financial conflicts of interest exist.