
Abstract
Abstract
Introduction
A
Preoperative suspicion of various reasons for inadequate visibility and accessibility to ovaries after vaginal hysterectomy by conventional methods, using sutures for hemostasis, often requires the surgeon to change the route of hysterectomy from a vaginally feasible hysterectomy to a more-invasive abdominal or expensive laparoscopic hysterectomy. Vaginal hysterectomy and adnexectomy may sometimes be difficult and challenging, using the suture method of inducing hemostasis.
Ovaries are visible in most patients after vaginal hysterectomy, 2 and a visible ovary may be accessible for a salpingo-oophorectomy attempt during vaginal hysterectomy in indicated cases. Factors such as increased uterine size, obesity, decreased vaginal access, and tubo-ovarian disease might not influence the feasibility of salpingo-oophorectomy significantly during vaginal hysterectomy. 3
Application of coagulation techniques to achieve hemostasis of lateral pedicles (instead of using sutures), use of a fiberoptic light source to improve visibility in a narrow operating field, and transvaginal mobilization of adhered adnexa may allow a gynecologic surgeon to perform many more salpingo-oophorectomies after vaginal hysterectomies for benign indications.
Materials and Methods
The current authors conducted an observational study from May 2010 through April 2014 in their urban private hospital. Consecutive candidates for vaginal hysterectomy for benign nonprolapsed indications with adnexectomy (unilateral or bilateral) were included for this study.
Included patients signed informed written consent forms for vaginal hysterectomy and adnexectomy (unilateral or bilateral). The institutional ethics committee granted approval for the study in April 2010.
During the study period, 2 of the current authors performed vaginal hysterectomy and indicated adnexectomy (unilateral or bilateral) according to the procedures described below.
Patient characteristics, indications for adnexectomy, surgical procedures needed to complete adnexectomy, success and failure, and perioperative outcomes were studied. The outcome of interest was the success of adnexectomy during vaginal hysterectomy.
General surgical procedures
In all cases, vaginal hysterectomy was performed using the Purohit technique for vaginal hysterectomy.4,5 After vaginal hysterectomy, salpingo-oophorectomy was attempted in all indicated cases using the procedures described for salpingo-oophorectomy for the Purohit technique for vaginal hysterectomy. 4
The round ligament stump was separated from the ovarian and tubal stumps by a split in broadligament. The split was progressed laterally and upward to reach the infundibulopelvic ligament. The skeletonized infundibulopelvic ligament was “hooked” by the bend of a right-angle forceps applied from the posterior aspect 4 (Fig. 1). The prongs of the right-angle forceps were opened to stretch ∼ 1–1.5 cm of the infundibulopelvic ligament between the prongs. The stretched infundibulopelvic ligament close to the ovary was coagulated by a bipolar current (45–50 watts), using a bipolar forceps (22-cm long, 2-mm wide tip) and divided by scissors, step by step, between the prongs of the right-angle forceps 4 (Fig. 1). Traction on the round ligament made it possible to visualize the infundibulopelvic ligament stump. Hemostasis was checked and lavaged with Ringer's solutions, which was sprayed from a 20-mL syringe.

Coagulation of the infundibulopelvic ligament. After separating the round ligament, Allis forceps (AF) are used to pull the ovarian ligament (O) and tubal stumps of the left side in a medially downward direction. The bipolar forceps (BF) is coagulating the skeletonized infundibulopelvic ligament (∼ 1 cm) between prongs of a right-angle forceps (RF).
Before attempting salpingo-oophorectomy, large ovarian cysts were occasionally aspirated via suction aspiration and decompressed 6 to improve visibility and accessibility of these cysts. To aspirate a cyst, a 3–mm bore long Veress needle was inserted above the ovarian ligament. The decompressed cyst was gradually pulled down to the operation field.
Adnexa adhered high in lateral pelvic wall were mobilized by the transvaginal adnexal mobilization maneuver described below to bring the ovary down to the operating field and to increase visibility before attempting salpingo-oophorectomy.
Deaver retractors and a fiberoptic light source, precisely directed through a pelvic illuminator 5 instead of a rigid telescope, 4 were used when poor visibility obstructed the progress of an adnexectomy in a deeper operating field.
Failed cases of vaginally attempted salpingo-oophorectomy were completed laparoscopically to avoid laparotomy. Laparoscopic adnexectomy was started from the stump side rather than from the infundibulopelvic ligament side, similar to that of vaginal adnexectomy according to the Purohit technique. 4 The skeletonized infundibulopelvic ligament of ∼ 1–1.5 cm was then coagulated close to the ovary and divided with scissors. The specimen was removed vaginally.
Purohit technique: Transvaginal mobilization of adhered adnexa from the lateral pelvic wall using tactile feel
After vaginal hysterectomy, downward and outward traction was achieved together with three Allis forceps holding stumps of the round ligament, the ovarian ligament, and the right Fallopean tube to keep them in tension. All the retractors and and the speculum were then removed. Then, the surgeon inserted the index and middle fingers of the right hand deeply through the open vaginal vault (as in bimanual pelvic examination) to the right side and guided the fingers over the stretched ovarian ligament and ovary (Figs. 2 and 3). By a series of gentle scratching (flexion–extension) movements by the tip of a finger, the ovary and Fallopean tube were lifted and mobilized down according to the tactile feel from the lateral pelvic wall. Release of the ovary and tube from lateral pelvic-wall adhesions was indicated by a gradual increase in downward descent of Allis forceps holding the ovarian and tubal stumps toward the surgeon (Fig. 3). These maneuvers brought down the adnexa from its high location to the operation field and made them visible and accessible. Similarly, the surgeon's left hand fingers were used to mobilize the left ovary and Fallopian tube from the left lateral pelvic wall. Then, the speculum and retractors were reinserted. Salpingo-oophorectomy was attempted in indicated cases by these procedures.
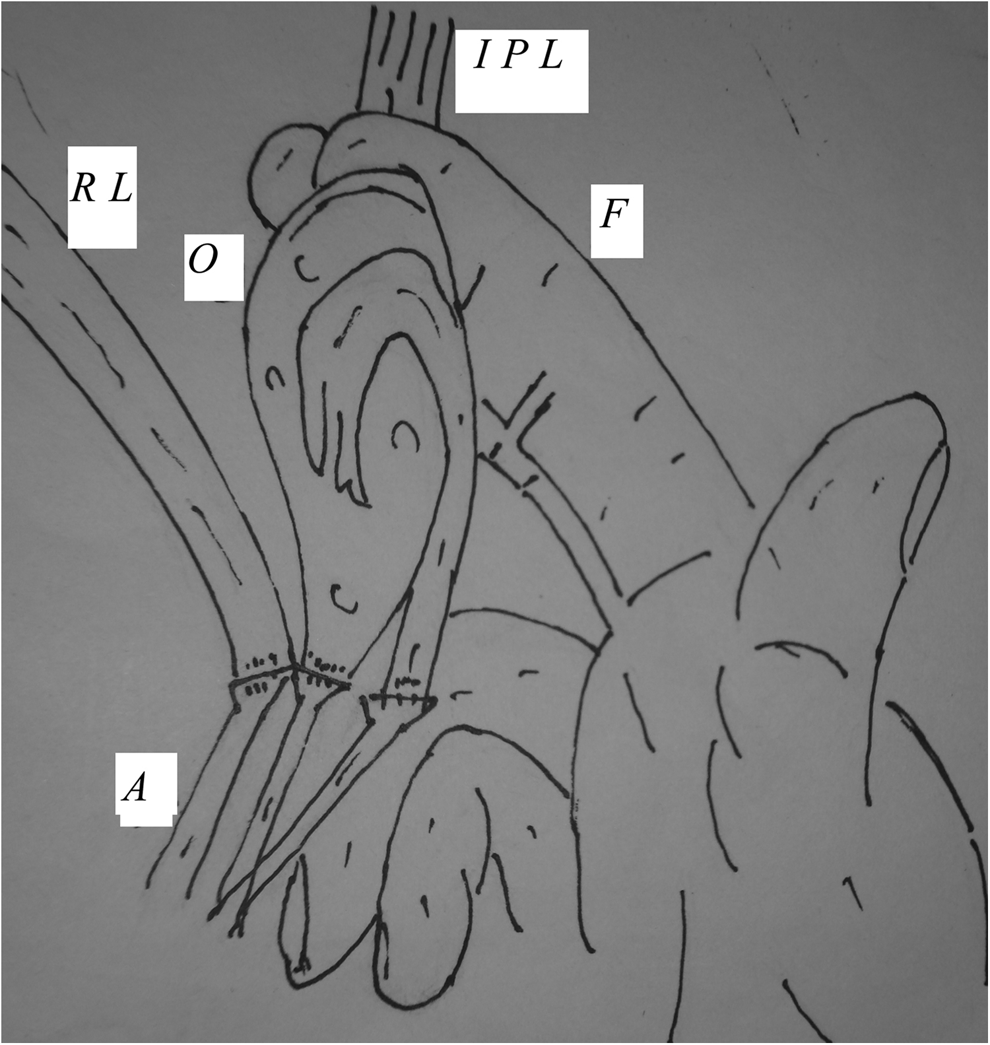
Diagram of adnexa mobilization. Allis forceps (A) are pulling the round ligament (RL), ovarian ligament, and tubal stumps in downward and outward directions. Fingers (F) are mobilizing the ovary (O) and Fallopian tube from the lateral pelvic wall. IPL, infundibulopelvic ligament.
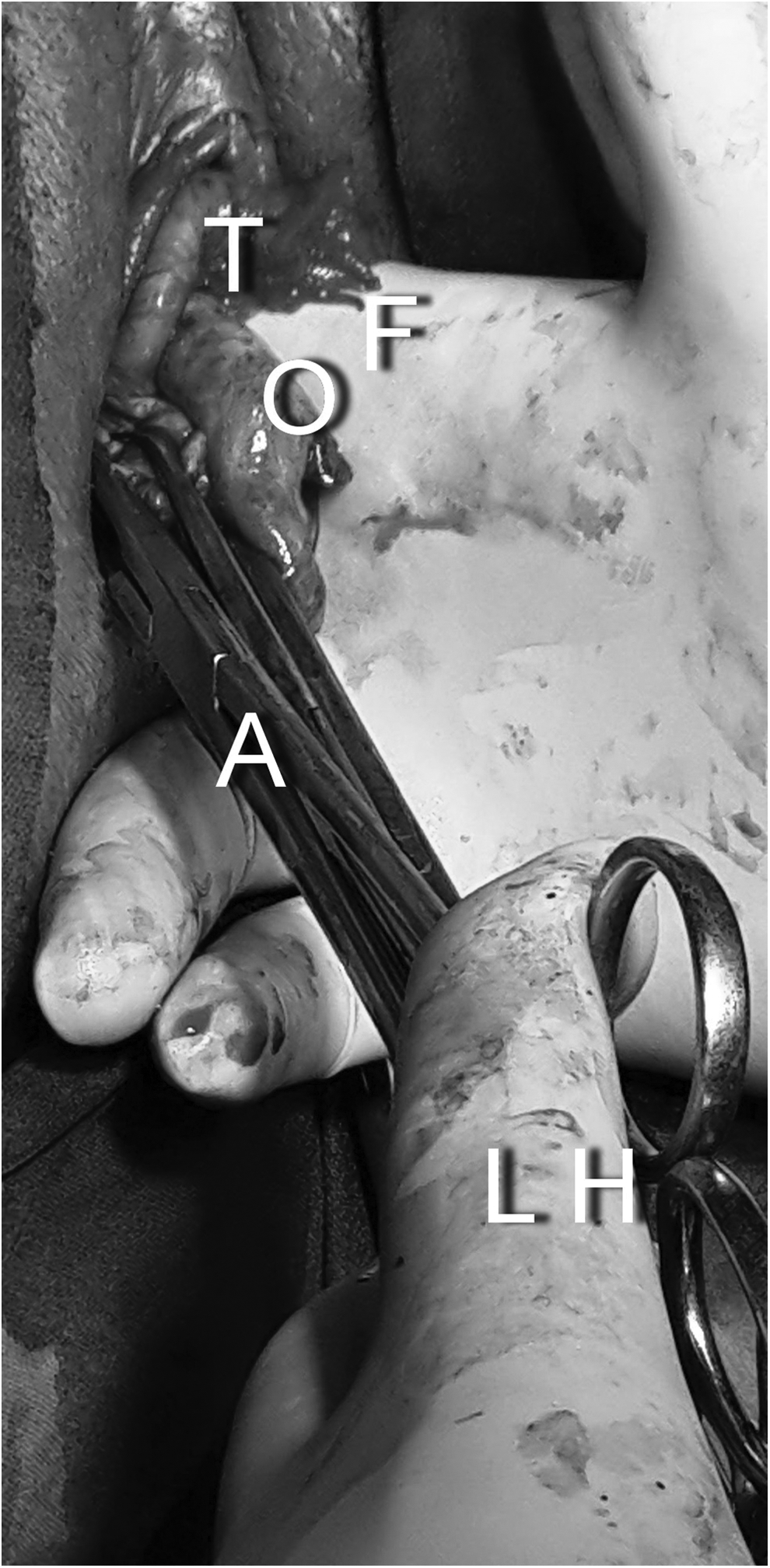
Adnexa mobilization. The left hand (LH) is holding stumps of the round ligament, ovarian ligament, and Fallopian tube (T), using Allis forceps (A). The right hand's index and middle fingers (F) are inserted through the vaginal vault. The ovary (O) and Fallopian tube of the right side are accessible following mobilization.
Results
The total number of hysterectomies for benign nonprolapsed uterus by different routes during the study period was 1868. Of them, 1811 (96.94%) patients underwent vaginal hysterectomy. Adnexectomy (bilateral/unilateral) during vaginal hysterectomy was indicated in 226 (12.47%) of 1811 cases. The patients' mean age was 47.61±7.86 years. There were 8 nulliparus patients, 18 patients with histories of previous caesarean sections, and 5 patients with previous laparotomy and myomectomy.
Benign indications for hysterectomy were fibroid uterus, adenomyosis uterus, dysfunctional uterine bleeding, chronic pelvic inflammatory disease (PID), endometriosis, postmenopausal uterine bleeding ascribed to a benign cause, benign tubo-ovarian mass, and hydrosalpinx.
The maximum size of the uterus among the cases was 18 weeks of gestation. The maxium body mass index of a patient was 51.75.
Table 1 shows indications for adnexectomy among 226 patients. The commonest benign indication among others was adnexal cysts. Cysts included ovarian cysts, paraovarian cysts, paratubal cysts, chocolate cysts of the ovaries, dermoid cysts of the ovaries, and twisted ovarian cysts. The largest ovarian cyst was 13 cm. Benign tubo-ovarian adhesions were caused by chronic PID in 20 (8.84%), endometriosis in 11 (4.86%), and postoperative pelvic adhesions in 13 (5.75%) cases.
A few cases had more than one indication.
Table 2 shows the procedures utilized for adnexectomy during vaginal hysterectomy for the 226 patients. In 170 (75.22%) cases of indicated salpingo-oophorectomy (unilateral/bilateral), the ovaries were free of adhesions, and a routine procedure 4 was used to complete the adnexectomy. In 6 (2.65%) cases of indicated salpingo-oophorectomy, large ovarian cysts needed cyst decompression before salpingo-oophorectomy. Not all ovarian cysts needed decompression for removal through a stretchable vaginal vault opening of 6–7 cm. In 44 (19.46%) cases of indicated salpingo-oophorectomy, adnexa was adhered high in the lateral pelvic wall and needed transvaginal manual mobilization before salpingo-oophorectomy could be performed. In 6 (2.65%) cases of indicated salpingo-oophorectomy, vaginal attempts at salpingo-oophorectomy failed and needed laparoscopic procedures to complete the salpingo-oophorectomy. Unilateral salpingo-oophrectomy was performed in 148 (65.48%) and bilateral salpingo-oophorectomy was performed in 78 (34.51%) cases. A bipolar forceps was used to achieve bipolar coagulation hemostasis in 206 (91.15%) cases. A bi-clamp was used in 20 (8.84%) cases. No suture was used for hemostasis in any case of adnexectomy. No patients required conversion to laparotomy and needed conversion for uncontrolled bleeding from the ovarian vessels.
Table 3 shows pre- and intraoperative patients' characteristics of cases with failed vaginal salpingo-oophorectomy. The ovaries in all 6 cases were invisible and inaccessible after vaginal hysterectomy even after sufficient retraction of the vault and use of a fiberoptic light source.
Table 4 shows the outcomes of adnexectomy during vaginal hysterectomy. Adnexectomy during vaginal hysterectomy was successful in 97.34% and failed in 2.65% of indicated cases. The mean operation time for vaginal hysterectomy with adnexectomy was 72.15±26.48 minutes). One cystostomy was performed during hysterectomy and not during adnexectomy. No intraoperative or postoperative bleeding was seen from the ovarian stumps in any case. There were no ureteric injuries. No patients had thermal injury to neighboring structures because of the adnexectomy.
Discussion
Preoperative apprehension of unpredictable difficulty with salpingo-oophorectomy still exists in the mind of the surgeon choosing vaginal hysterectomy for a benign nonprolapsed uterus. 7 This concern regarding unsuccessful attempts during vaginal hysterectomy has led many surgeons to prefer more-visible laparoscopic-assisted hysterectomy 8 to avoid laparotomy or abdominal hysterectomy. However, similar to other researchers' observations, salpingo-oophorectomy could be accomplished in the majority cases and need for salpingo-oophorectomy should not always be a contraindication to vaginal hysterectomy. 9
Good visualization for successful adnexectomy during vaginal hysterectomy has always been emphasized in many studies.2,6,10 Stretchibility of the infundibulopelvic ligament had also been emphasized as a preferred factor for successful adnexectomy using many conventional techniques,2,3 using suture for hemostasis.
In this series, adhesions free in-pelvis adnexa of all indicated cases, including postmenopausal women, had been removed irrespective of the stretchibility of the infundibulopelvic ligament. The stretchibility of the infundibulopelvic ligament did not affect completion of adnexectomy in this study, when the ovaries were either visible or made visible using a fiberoptic light source transmitted by a pelvic illuminator. 5
Adhered adnexa have been identified as risk factors for unsuccessful adnexectomy by conventional methods6,11 using sutures. In-pelvis adhered adnexa had been removed in all cases in this study after transvaginal manual mobilization maneuvers. The accessibility was enhanced further by use of a long and narrow-tipped bipolar forceps for hemostasis in place of a suture. Bipolar forceps was preferred to a wide-jaw bi-clamp in narrow operation fields close to the pelvic wall. Narrow-tipped bipolar forceps also helped to reduce the spread of heat to neighboring structures.
The technique for transvaginal adnexal mobilization of adhered adnexa in this study was simple, easily available, quick, and bloodless after vaginal hysterectomy but was different from the conventional ones described by Ballard and Walters 10 and by Sheth, 6 although the purpose of bringing down the adnexa to the operation field remained the same. Conventionally, patients who have this risk 6 would need laparoscopic mobilization of adnexa during laparoscopic-assisted vaginal hysterectomy (LAVH), total laparoscopic hysterectomy, 1 or abdominal hysterectomy. The surgeons in the current study did not need laparoscopic mobilization before vaginal hysterectomy in any case. Instead of LAVH, a vaginal adnexectomy by current visualization methods was attempted in such cases, and laparoscopy was reserved for rare cases of failed vaginal salpingo-oophorectomy to avoid laparotomy.
Using a conventional procedure, Sizzi et al. 11 failed in 9.3% cases of indicated adnexectomy because of thick adhesions in pelvis caused by endometriosis and chronic PID. The surgeons in the current study, after transvaginal mobilization, observed that adnexal adhesions in the pelvis resulting from endometriosis and inflammation were soft and mobilized more easily by tactile feel than those of postoperative adhesions following myomectomy. These stronger postoperative adhesion bands only needed coagulation and division by scissors. However, gentle tissue handling and careful adhesiolysis had been emphasized in the current study, similar to those of earlier studies6,10 to avoid tearing during dissection. No injury to neighboring structures or uncontrolled bleeding from the pelvic sidewall was seen in this study because of the transvaginal adnexal mobilization that was performed after removal of the uterus.
Adnexectomy failed in 2.65% cases in the current series. In all of the failed cases, the ovaries were situated above the pelvic cavity. Five of six ovaries were adhered to different sites in the abdominal cavity following chronic inflammation. One large dermoid cyst, 7 cm in size, although not adhered to any abdominal organ was quite heavy with a very long ovarian ligament, and its distended portion could not be visualized for needle aspiration and decompression vaginally. Thus, all ovaries were invisible and not reached vaginally despite use of improved illumination with pelvic illuminator and could not be mobilized down manually. These patients needed laparoscopy to complete adnexectomy in the current study.
Initiation of laparoscopic adnexectomy from the stump side after vaginal hysterectomy in the current study made it easier to find almost a bloodless cleavage up to the infundibulopelvic ligament. Using a safe distance 10 of 1–1.5 cm between the lateral pelvic wall and the upper pole of the ovary for bipolar forceps coagulation and use of scissors in the current series helped avoid ureteric injury during both vaginal and laparoscopic adnexectomy.
Failed attempted vaginal salpingo-oophorectomy and subsequent laparoscopic procedures did not increase postoperative morbidity in any case in this study. The mean operation time for vaginal hysterectomy with adnexectomy was more than that of only vaginal hysterectomy 4 because many patients in the current series needed additional procedures such as decompression of large adnexal cysts and adnexa mobilization of adhered adnexa. However, the operation time was similar to vaginal hysterectomy in cases associated with previous caesarean section. 5
Conclusions
Most of salpingo-oophorectomies for benign indications could be completed during vaginal hysterectomy using bipolar coagulation for hemostasis, a fiberoptic light source to improve visibility, and transvaginal mobilization of adhered adnexa in the pelvis. The remaining few cases of failed adnexectomy during vaginal hysterectomy could be completed laparoscopically to avoid laparotomy.
Footnotes
Disclosure Statement
The authors have no conflicts of interest associated with publication of this article.