
Abstract
Abstract
Introduction
E
Endometriosis may be suspected following clinical and gynecologic, and bimanual examination. Transvaginal sonography and the CA-125 tumor marker may be helpful for diagnosis, but a definitive diagnosis can be made only by histologic examination. 1 Laparoscopic visualization and biopsy of lesions are the “gold standard” for diagnosing this disease.1,5
The main goal of therapy involves elimination of symptoms, regression or removal of the existing endometriosis formations, and prevention of new formations. Pharmacologic therapy is prescribed to reduce endometriosis lesions and inflammation, and to prevent their dissemination. Therapy can be implemented alone or postoperatively, but there is no strong evidence to justify its implementation preoperatively. 4 The medications used most frequently for this type of treatment are oral contraceptives, progestogens, and gonadotropin-releasing hormone (GnRH) analogues. 6 All forms of pharmacologic therapy suppress ovarian activity and lead to atrophy of endometriosis implants, although the extent to which they succeed at this is varied. Postoperative pharmacologic treatment should prevent recurrence of symptoms significantly, 7 but the data in the literature are contradictory.
Surgical treatment is aimed to remove all visible endometriosis fields, to remove all adhesions, and to restore the internal genital organs to their appropriate anatomical relationships. 8 There are two surgical approaches currently in use: laparoscopy and conventional surgery (laparotomy).1,5 The surgical approach may be conservative, semiconservative, or radical, 5 and the type of surgery performed primarily depends on the extent of a patient's endometriosis, her age, and her desire for offspring. Conservative surgical treatment removes only the ectopic endometrium and semiconservative surgery removes the pelvic organs (hysterectomy, ovariectomy), whereas radical surgical treatment involves hysterectomy with bilateral salpingo-oophorectomy. 9 Conservative operative techniques used for superficial implants generally involve coagulation or vaporization of the lesions, 10 whereas the range of surgical techniques that can be performed to address endometriomas is considerable. In practice, cystectomy (complete excision of the cyst) is generally performed or—as an alternative —drainage of the cyst is followed by electrocoagulation of its wall (cystotomy).
In certain countries, conventional and laparoscopic approaches are used equally to treat endometriosis surgically. 11 However, according to many researchers, priority should be given to laparoscopy, regardless of the applied operative treatment and technique.1,2 The particular advantages of this method are shorter hospital stays and more-rapid and less-painful patient recovery. However, study data do not indicate that laparotomy cannot be used to treat endometriosis. This approach is indicated in the case of severe forms of the disease associated with strong adhesions, as in the case of large endometriomas and deep-infiltrating forms of the disease. 5
Despite the variety of methods for treating endometriosis and the great progress in its surgical treatment, the nature of the disease is such that the range of surgical techniques is actually limited, as reflected in the frequent recurrence of endometriosis following surgery. Depending how one defines recurrence (just a subjective feeling of pain recurrence or by use of accurate clinical methods), endometriosis stage, implementation techniques, and use of adjuvant drug therapy, the percentage of recurrence in a 2-year period ranges from 6% 12 to 30.4%, 13 and according to some studies, up to 67%. 14 Preventing endometriosis recurrence is an elusive goal for doctors.
The aim of this study was to determine if surgical approach, operative technique, and postoperative pharmacologic treatment influenced the frequency of endometriosis recurrence.
Materials and Methods
This was a cohort study that was performed in the University Clinic of Gynecology and Obstetrics of Narodni Front, in Belgrade, Serbia. During a 1-year period, 204 women received surgical treatment for endometriosis (70 patients underwent conventional surgery and 134 underwent laparoscopy). Of those subjects, the study included 111 women with whom it was possible to make contact, given that data on recurrence of endometriosis and postoperative pharmaceutical treatment were collected 2 years following the surgery. The age of the patients ranged from 21 to 61, with the average age being 33.65 years. The main criterion for entry into the study was a histopathologic or surgically confirmed diagnosis of endometriosis, which was determined based on clinical, gynecologic, and ultrasound examinations. The study included only patients with peritoneal endometriosis and ovarian endometriomas with a diameter >3 cm.
Operative protocols, data on the age of patients when the surgical procedures were performed, surgical approaches used (laparotomy, laparoscopy), pathologic forms of endometriosis (nodes, endometrioma), operative treatments (conservative, semiconservative, radical) and techniques performed to treat ovarian endometriomas (cystectomy, cystotomy) were evaluated. Data were evaluated on postoperative pharmaceutical therapy, length of treatments, whether or not they were regularly controlled following surgery, and recurrences in the first 2 years after surgery. Recurrence was defined as a new formation of endometriosis detected by ultrasound examination with or without symptoms.
For statistical analysis of the data, descriptive and analytical statistics methods were used as follows: a t-test for numerical parameters and a χX2 test for descriptive parameters. The level of statistical significance was defined as p<0.05.
Results
Comparison was performed according to the percent of recurrences with respect to surgical approach (45 patients underwent conventional surgery and 66 patients underwent laparoscopic surgery); surgical technique for laparoscopy when treating ovarian endometriomas (31 patients had cystectomies, whereas cystotomy was performed in 30 patients); and use of postoperative pharmaceutical therapy (71 patients were treated with medications, whereas 40 patients were not).
Table 1 shows the recurrence of endometriosis in patients who underwent laparoscopic surgery and those treated with the classical surgical approach. Analyzing these data, the χ2 test revealed a statistically significant difference between the two groups, with a higher percentage of recurrences in the group of laparoscopic-operated patients (χ2=4.66, p<0.05). The results are presented graphically in Figure 1. Figure 2 shows the structure of the groups according to the applied surgical procedures and techniques. Table 2. shows the age structure of the analyzed groups. A Student's t-test revealed that there was a significant difference between the groups. The patients were, on average, older in the conventional surgery group (t=–3.9, p<0.01). The results are presented graphically in Figure 3. Table 3 shows the recurrence in the group who received cystectomy in the framework of the classical surgical approach and in the group who underwent laparoscopic cystectomy. Statistical analysis of the data showed no significant difference between the groups (χ2=0.27, p>0.05). The data are presented graphically in Figure 4. Table 4 shows the occurrence of relapses in the groups of patients who underwent cystectomy and cystotomy under laparoscopy. Statistical analysis of the data indicated that there was no significant difference between the groups (χ2=1.33, p>0.05). The data are presented graphically in Figure 5. Table 5 shows the recurrence of endometriosis in relation to postoperative pharmaceutical treatment. Statistical analysis of the data indicated no significant difference between the groups (χ2=3.33, p>0.05). The data are presented graphically in Figure 6. Table 6 shows the types of postoperative medications used.
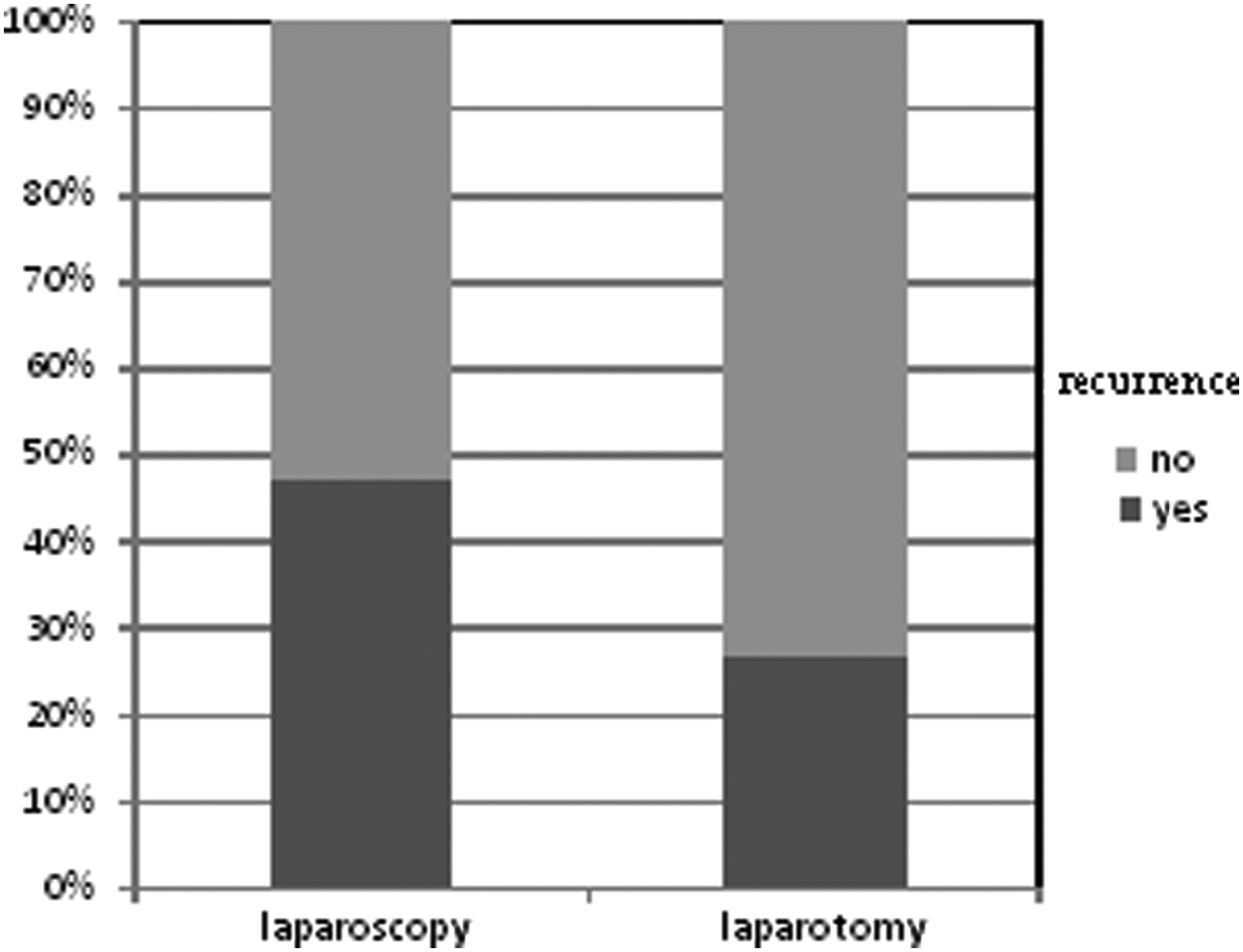
Percentages of recurrence in patients who underwent surgery with conventional and laparoscopic approaches.
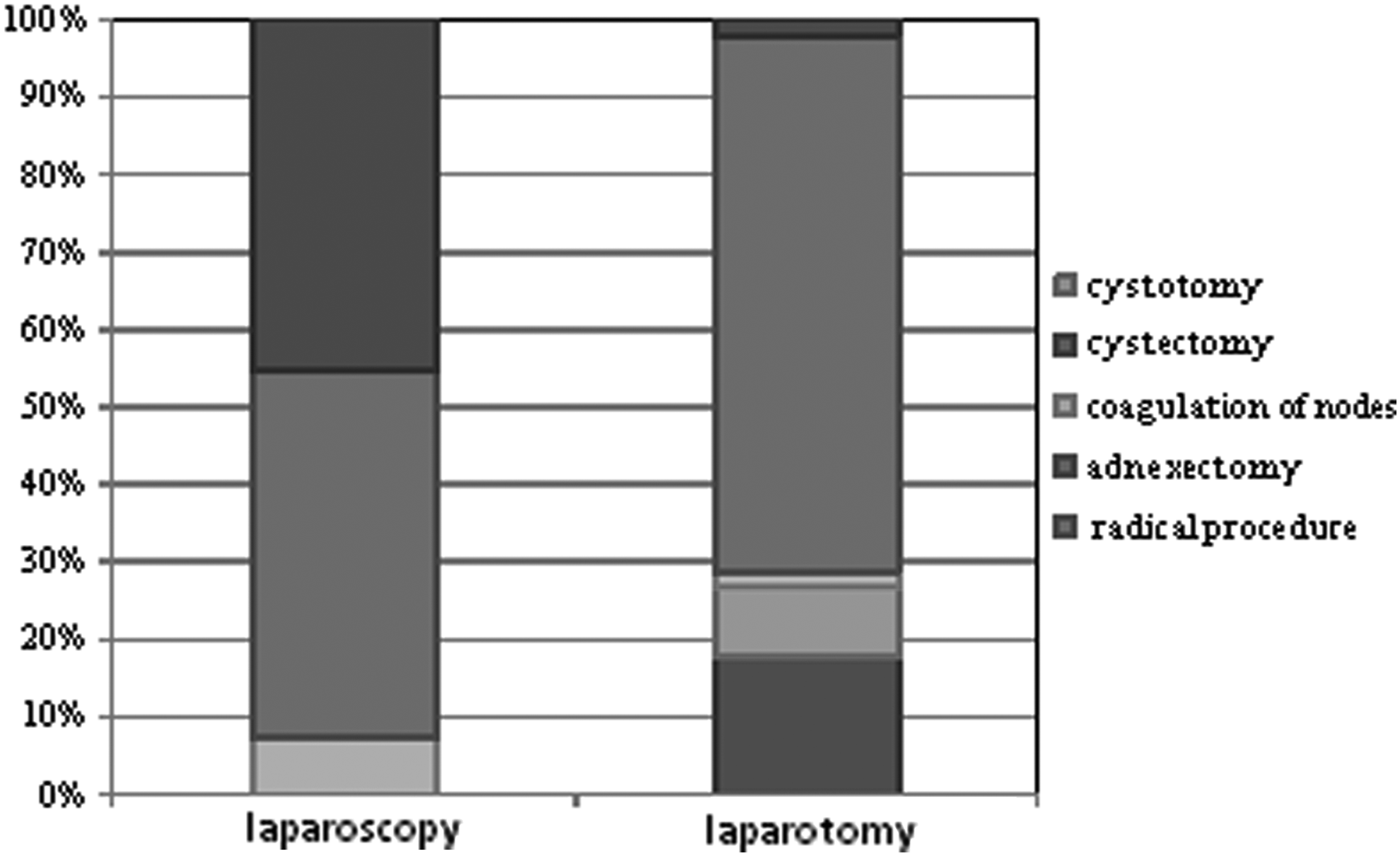
Surgical procedures and techniques used during surgery.
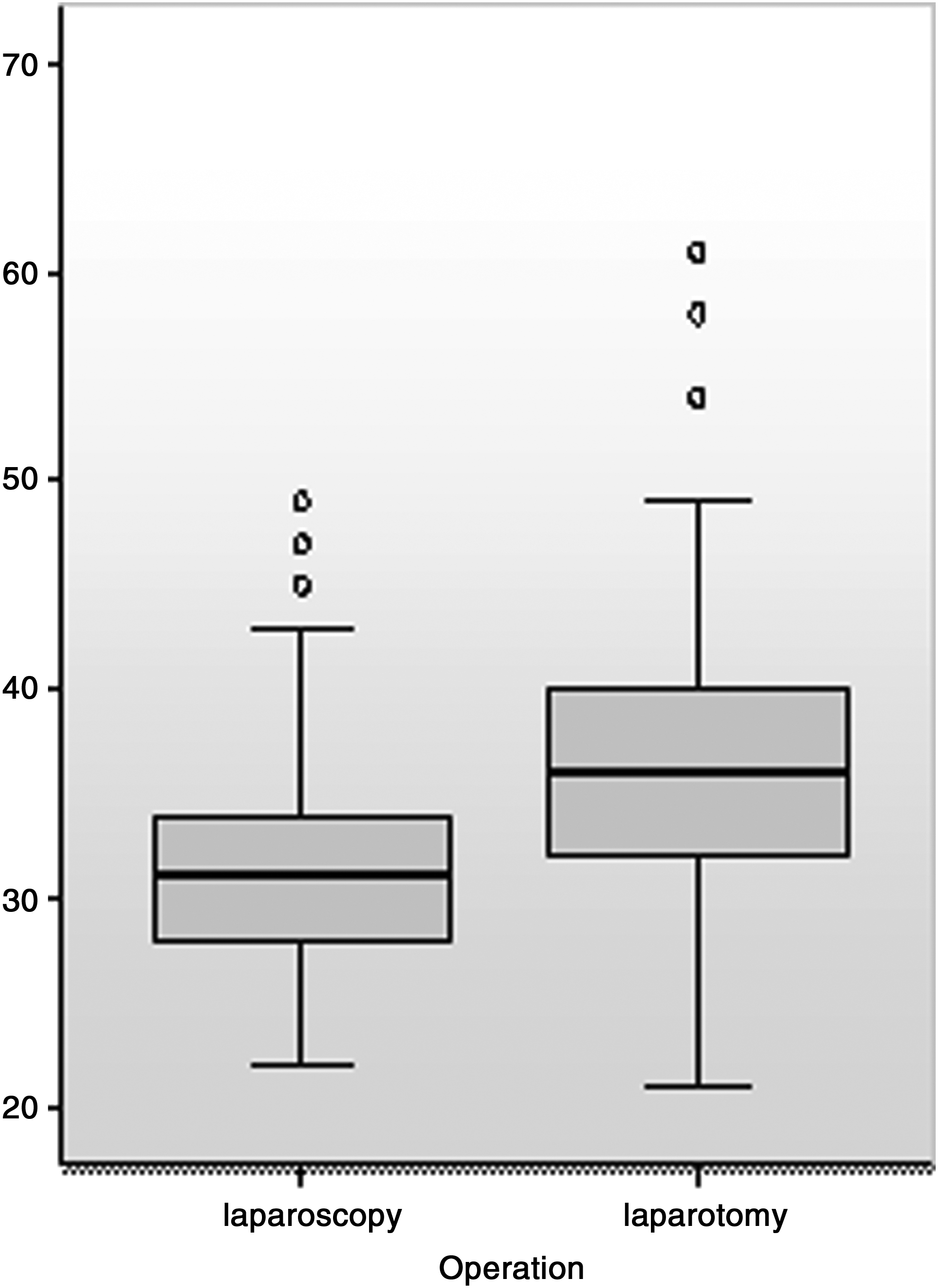
Ages of the patients.

Percentages of recurrences after cystectomy in the laparotomy and laparoscopy patient groups.
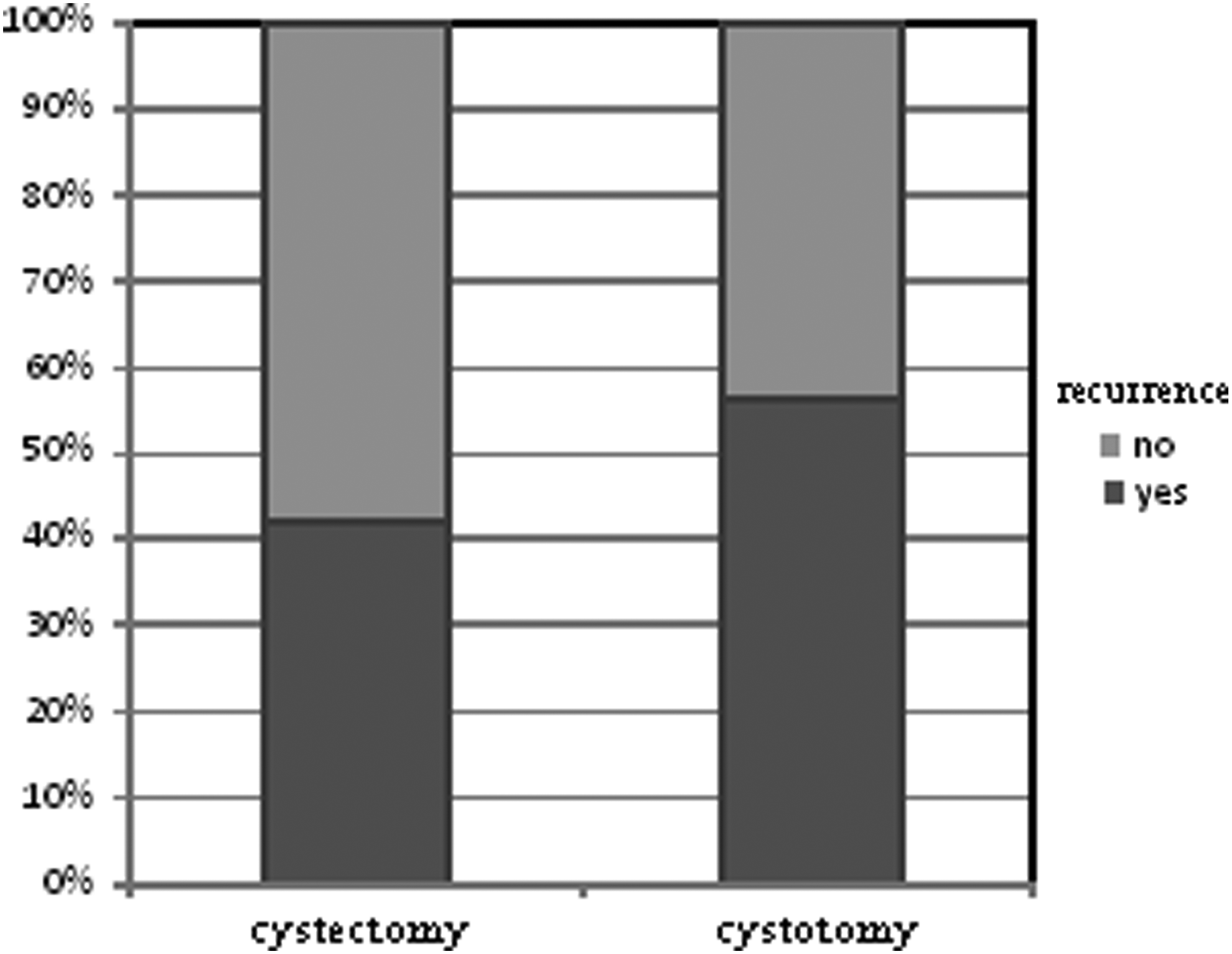
Percentages of recurrence of endometriosis, according to the surgical technique used.

Percentages of recurrence of endometriosis according to postoperative medical treatment.
χ2=4.66, p<0.05.
χ2=0.27, p>0.05.
χ2=1.33, p>0.05.
χ2=3.33, p>0.05.
GnRH, gonadotropin-releasing hormone.
Discussion
One of the main characteristics of endometriosis is the high degree of recurrence of the disease regardless of the type of therapy implemented. Depending on the size of the study, the stage of endometriosis, how recurrence is defined (in terms of recurrence of symptoms, clinically detectable endometriosis formations, or histopathologic analysis–confirmed relapse), the recurrence rates in the literature range from 6% 12 to 67% 14 for a 2-year period. In the present study, for this period, relapse occurred, on average, in 38.7% of the patients. Although this percentage may appear to be high, compared with the results of some studies, an analysis of the relevant studies has shown that smaller studies, such as the current study, tend to record higher recurrence rates. 14
The laparoscopic approach is associated with a significantly shorter hospital stay, reduced costs, and more-rapid recovery of patients, and—in the opinion of many researchers—the same efficiency for treating endometriosis, whereas the classical surgical approach is advisable only for large endometriomas and endometriosis stages associated with strong adhesions, as in the case of deep-infiltrating forms of the disease. 5 Despite these recommendations, the results of certain studies have indicated that the classical surgical approach is still used in practice nearly as frequently as the laparoscopic approach in many countries, 11 including Serbia. 15 To perform another efficiency evaluation of the two surgical approaches for addressing endometriosis, a comparison was made of the percent of recurrence of endometriosis in patients who underwent conventional surgery versus patients who were operated on via the laparoscopic approach. Among the patients who underwent laparoscopic surgery, relapse occurred in 31%/47.0% of patients, which was significantly higher than in the patients who underwent classical surgery, among whome relapse was noted in 12 (26.7%) patients.
The two treatment groups had a significant difference in age. The average age of women operated on by the conventional approach was 36.73 years (16.6% of patients >age 40), whereas, in the group of women who were operated on via laparoscopy, the average age was 31.55 years (7.5% of women age >40). According to the results of certain studies, endometriosis relapses occur frequently in younger women,12,16 and the uneven age structure of the group might be one explanation for the differences in recurrence rates.
There was also a difference between the groups with respect to surgical procedures and techniques used (Fig. 2). In the women who were operated on with laparoscopy-only, conservative procedures were performed (electrocoagulation of nodes, cystectomy
The current study was conducted in a tertiary health care center, and a large percentage of patients were women from the interior of the Serbian republic; further monitoring of these patients, upon completion of surgery, was continued in other health centers. Therefore, the data on disease recurrence were collected by conducting telephone surveys and interviewing patients but only if they had transvaginal ultrasound checkups between 1 and 2 months before the telephone calls.
The varying levels of education of the large number of gynecologists involved and their ability to differentiate endometriosis formation, as well as varying levels of patient awareness and familiarity with the illness, might also be among the factors that influenced the current results.
To homogenize the data maximally, the effects of age and surgical procedure were eliminated, and, after creating predefined homogeneous groups with respect to age distribution (t=1.47, p>0.05), patients who had cystectomy with a conventional surgical approach were compared to patients who received laparoscopic cystectomy. An analysis of the percentages showed that the χ2 test revealed no significant difference between the groups (χ2=0.27, p>0.05). As in the current study, another group of researchers compared the outcomes of laparoscopic cystectomy and microsurgery using laparotomy in a retrospective study involving women <40 years with ovarian endometriomas with a diameter >3 cm and concluded that the two surgical approaches were equally effective for treating endometriosis. 17
Furthermore, a group of Canadian researchers who compared laparoscopic ovarian cystectomy to cystectomy performed by laparotomy to treat endometriomas with a diameter >3 cm reported no significant difference between the two groups in the percent of recurrence in a 3-year period. 18
The most common form of endometriosis is ovarian endometrioma and, according to existing studies, this accounts for up to 55% of all forms of the disease. 13 According to the recommendations of the European Society of Human Reproduction and Embryology, surgical treatment of endometrioma is recommended only when the diameter of the lesion is >3 cm.13,19
To evaluate the two most commonly performed surgical procedures for preventing endometriosis recurrence, the percent of recurrence in women who had laparoscopic cystectomy (31 patients) was compared with patients who had laparoscopic cystotomy (30 patients). Cystectomy, according to the results of the current study, was followed by a relapse in 41.9% of cases in a 2-year period, whereas the recurrence rate in patients who had cystotomy was 56.7%. Although these differences were clinically significant, statistical analysis indicated that there was a significant difference between the groups, which, according to the current study's results, made cystotomy equally effective for treating endometriosis.
Although most researchers recommend cystectomy as the method of choice for treating ovarian endometriomas,5,14 one of the first randomized trials that compared the two techniques produced the conclusion that cystectomy was followed by better symptom control and that the procedure delayed time to recurrence. However, when comparing the percent of clinically detectable recurrence between the groups, no significant difference was observed. 20 In the group of 32 women who underwent cystectomy, researchers detected relapse in 6.2% of women, compared with 18.8% of women who underwent cystotomy, but this clinically significant difference, as in the present study, was not confirmed by statistical analysis.
Researchers who conducted another prospective study comparing various surgical techniques for treating ovarian endometrioma concluded that laparoscopic treatment should not include excision but rather drainage of the cyst followed by wall coagulation. 21 Similar to the current study, Canadian researchers compared the percent of recurrence in 80 patients who had cystotomy with 23 patients who underwent cystectomy via a laparoscopic approach. The researchers reported that cystotomy of ovarian endometriomas with a diameter >3 cm was as successful as cystectomy, and the recurrence rate of endometriosis between the groups in the three-year period did not differ. 18
According to the results of some studies, postoperative pharmaceutical therapy should be included in the treatment protocol for addressing endometriosis, given that this type of treatment prevents recurrence of disease and delays recurrence of symptoms. 22 In the current study, the percent of recurrence among patients who were only surgically treated and patients who had postoperative, adjuvant pharmaceutical therapy was not significantly different (X2=3.33, p>0.05).
Postoperative therapy in the current study was given to 64% of the women (71/111). With respect to postoperative pharmacological treatment, there was a significant difference between patients who were operated on using laparoscopy and laparotomy. In women who underwent classical surgery, this type of treatment was administered to 20 patients (44.4%), whereas, in women who underwent laparoscopic surgery, postoperative therapy was administered to 51 patients (77.3%, χ2=12.52, p<0.01).
After laparotomy and postoperative pharmacologic treatment during the reporting period, recurrence was recorded in 45% of patients (9/20), which was surprising considering that there were 3 recurrences (12%) observed for women who were operated upon with the same surgical approach and who did not receive postoperative therapy. Among the patients who received medication after laparotomy, the conservative surgical treatment was performed in 90% of cases, whereas the radical surgical approach, which is associated with low recurrence, 18 was performed in 32% (8/25) of women who did not receive therapy after laparotomy. These data might have affected the results of the current study.
In patients who underwent laparoscopic surgery, recurrence was recorded in 23 patients (45.1%) who received drug therapy, whereas, in the 15 women who did not receive drug treatment in this group, relapse was noted in 8 (53.3%). The most common type of therapies administered were GnRH-analogues (Table 6). The length of implementation of pharmaceutical treatments differed, with 17.57% of patients receiving treatment for 3 months, 29.72% of patients receiving treatment for 4 months, and 51.35% of patients receiving the therapy for 6 months following surgery; postoperative treatment lasted 1 year in only 1 patient (13.51%).
Similar to the current study, Japanese researchers analyzed factors that might influence endometrioma recurrence after laparoscopic excision of endometrioma and reported that postoperative pharmacologic treatment did not lead to a lower percent of endometrioma recurrence. 12
In one randomized study comparing patients who had relapses after conservative surgery and who postoperatively received GnRH analogues in a 3-month period, and those who were not subjected to this treatment, the recurrence rates were similar. 23 Another prospective randomized study indicated that postoperative administration of GnRH analogues had no effect on preventing endometriosis recurrence. 24 The researchers concluded that this treatment does not even delay the time to recurrence of symptoms, which had been previously observed in other studies. 25 A randomized study on the impact of postoperative use of oral contraceptives, conducted in a group of 70 women with advanced and severe forms of endometriosis, indicated that, in a 2-year period, there was no significant difference between the 6% recurrence rate in patients who received postoperative contraceptives, compared to 3% in those who did not receive drug treatment. 26
Similarly, a randomized controlled study on the 3-month use of danazol in patients with a moderate and severe form of endometriosis was not accompanied by a significantly lower percent of recurrence over a 1-year period. The researchers noted a relapse in 26% of women receiving danazol and in 34% of patients who did not receive postoperative pharmaceutical treatment, which was not sufficient for significance. 27
In contrast to the abovementioned research and the current study, several other studies support the use of postoperative drug therapy. These differences may be the result of variability of studies in relation to sample sizes, patient age distributions, drug doses used, and durations of postoperative therapy, as well as the lengths of patient follow-up. In most studies, as in the current study, the implementation period of postoperative pharmacologic treatment lasted for <1 a year, and the follow-up period of patients rarely exceeded 3 years. A longer implementation period of postoperative pharmacologic treatment and a longer follow-up of patients might have led to some new insights. We are in need of new, controlled randomized studies to confirm the effectiveness of this treatment modality.
Conclusions
Classic and laparoscopic surgical approaches are equally effective for surgical treatment of endometriosis. Cystotomy and cystectomy are equally successful techniques for surgical treatment of ovarian endometriomas, and a final treatment decision should be made depending on the individual patient's needs. There were no differences in disease recurrence based on operative technique. Therefore, the only goal should be to apply the most appropriate technique for the patient (situation), and then, priority should be given to laparoscopy because of the incomparably rapid and less-painful patient recovery conferred by laparoscopy.
Postoperative drug therapy does not reduce the risk of endometriosis recurrence.
Footnotes
Disclosure Statement
The authors state that they do not have any commercial, proprietary, or financial competing interests in the products or companies described in this article.