
Abstract
Abstract
Introduction
L
Single-incision laparoscopic surgery (SILS) was developed with the aim of reducing the invasiveness of conventional laparoscopy (ranging from 3–5 incisions). As an effort to promote further advances in minimally invasive techniques, SIL is a promising alternative to multiple-port surgery. Such an approach is used with the goal of mitigating patient's postoperative pain, reducing hospital stays, promoting earlier recovery from diseases, and producing better cosmetic results.1,3,4
The first description of SILS in gynecology was published in 1969, when Wheeless reported tubal ligation through one port, using a 12-mm optic. 5 Since the 1990s, a range of gynecologic procedures has been described using SILS. These procedures include oophorectomy, salpingectomy, tubal sterilization, ovarian cystectomy, assessment of ectopic pregnancy, and even hysterectomy.6,7
The objective of the present study was to explore the results of 64 patients with benign adnexal masses that were treated with SILS.
Materials and Methods
Study design
In a tertiary center in Brazil, 64 patients with presurgery diagnoses of benign adnexal mass underwent laparoscopic surgery, using the SILS technique. The adnexal mass was presumed to be benign based on echography features, patients' age, CA125 levels and menopausal status.
Records of all patients were reviewed, and data were stored in a data bank.
The study was approved by the ethics committee of the Hospital de Baleia, Fundação Guimarães, Belo Honzonte, MG, Brazil (CAAE 17036713.6.0000.5123).
SILS
All patients were placed under general anesthesia with tracheal intubation and bladder catheterization before they underwent SILS. Each patient was positioned supine, with arms parallel to the body. For sterilization, chorohexidine solution was used. Antibiotic prophylaxis with first-generation cephalosporin was also administered before anesthesia.
The surgical technique was standardized as follows:
(1) Subcutaneous periumbilical injection of 10 mL of bupivacaine with adrenaline; vertical or curved incision (according to patient's features) in the inferior edge of the umbilicus, with a 2.5–3cm extension. (2) Subcutaneous tissue dissection, fascial incision, and peritoneum opening with direct vision (3) Repair stitches in the angles of the fascial incision with Vicryl 1–0 (4) Introduction of the single-access platform in the incision (SITRACC–Edlo S/A Produtos Médicos; Figs. 1 and 2) (5) Inflation of the abdominal cavity with gas, with maximum 15 mm Hg pressure; after pneumoperitoneum was installed, introduction of a 10-mm, 0°, optical device in the corresponding access (6) Cavity inspection (7) Introduction of tissue forceps in the other accesses (5 mm) of the SITRACC, according to the features of the mass as follows: 42-cm Maryland articulated forceps; 42-cm flexible prehension forceps with rack; 50-cm gallbladder prehension forceps with curved rack; or 42-cm curved Metzenbaum scissors (Edlo S/A Produtos Médicos) (8) Prehension and traction of the ovarian ligament with flexible prehension forceps, identification of the ipsilateral ureter through the transparent peritoneum, section and ligature of pelvic infundibulus; resulting material was withdrawn from the abdominal cavity through the umbilical incision, without need for other incisions (9) After lesion withdrawal, and cavity hemostasis review, pneumoperitoneum was undone, and SITRACC was taken off by traction (10) Aponeurosis continuous suture with a Vicryl 1-0, skin suture with Vicryl 4-0, and a local bandage.

Single trocar access instrument (SITRACC–Edlo S/A Produtos Médicos).
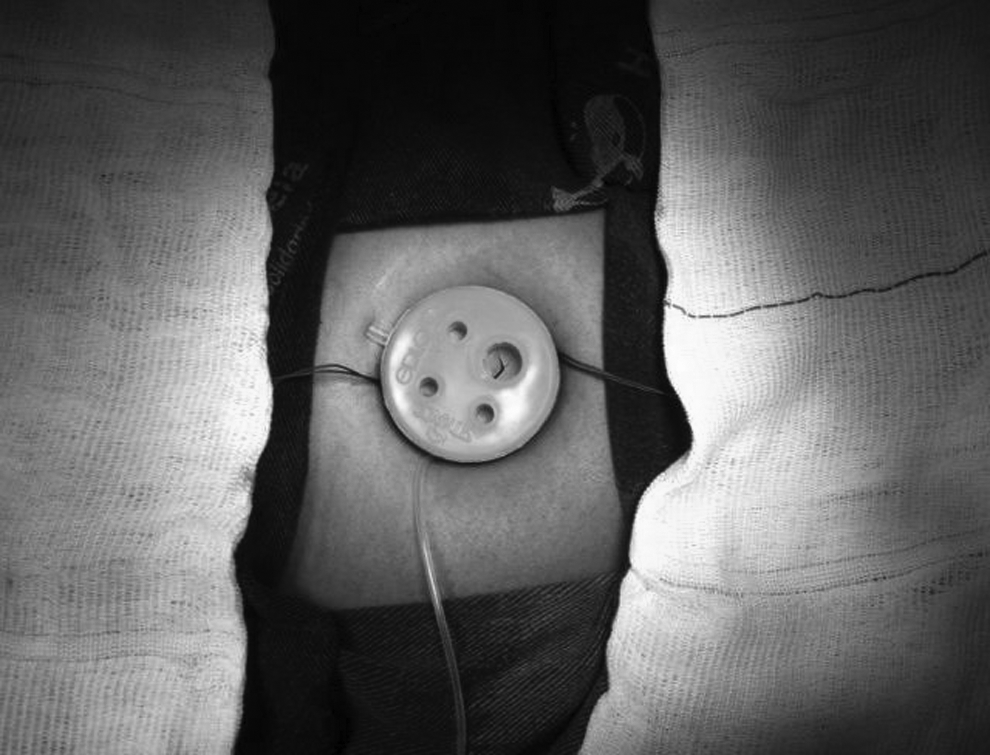
Single trocar access after insertion (SITRACC–Edlo S/A Produtos Médicos).
Results
The demographic data of patients are presented in Table 1. The most common previous disease was arterial hypertension, which was present in 11 patients (17%); 8 patients reported smoking habits (12,5%).
Histologic results of all the recruited patients showed benign lesions (Table 2). Benign cysts (28; 43,8%), solid teratomas (10; 15,6%), and endometriosis (8; 12,5%) were the most prevalent findings.
There was only one case of conversion to laparotomy, because of the presence of extensive adhesions in an overweight patient. With respect to postoperative complications, there was one case of of incisional hernia—this was the only event that required new hospital admission. The average length of stay in the hospital was 22 hours (range: 17–28).
Discussion
According to a review published in 2013, there are ∼66 studies on SILS in gynecologic surgery, which are 17 case reports, 32 case series, 13 retrospective studies and 4 randomized trials. 8
Despite their limitations, there are studies reporting the use of SILS in oncologic cases, for disease staging, lymphadenectomy, or tumoral exeresis. In 2009, Fader and Escobar published a pioneering study—a case series of 14 cases of gynecologic malignant disease that were approached with SILS. 9
The current authors emphasize that, even with the rising interest envolving with respect to minimally invasive procedures, there are not defined criteria for patient eligibility nor for which would be the most important prognostic factors.
One of the hypothetic advantages of the SILS technique is the insertion of SITRACC through direct visualization, which can possibly minimize the risk of adjacent organ injury. In addition, extraction of masses through a larger port may avoid spillage into the abdominal cavity. Other benefits may be the smaller trauma to the abdominal wall, cosmesis, faster recovery, and less postoperative pain. 10
The reduced mobility of the surgeon's hands and the handling of instruments could be considered limitations. In order to ameliorate this situation, the literature cites the use of intrauterine manipulation devices and a combination of short and long instruments, reducing the contact between them. 10
The use of cephalosporins as prophylaxis in laparoscopic surgeries is not something that has acheived a consensus. In Hospital de Baleia, it was decided to use prophylaxis initially, considering the larger incision required for introduction of the SITRACC (∼ 3 cm) in a region that is considered to be contaminated (e.g., an umbilical scar). Currently, considering the low rates of surgical-site infection, the antibiotic prophylaxis is no longer indicated in the current procedures.
In this study, the average length of stay in the hospital was 22 hours, ranging from 17 to 28 hours. All patients were discharged in good clinical condition. The reduced hospital stay was possible because of the absence of severe immediate postoperative complications. Comparable results were reported by Kim et al. in a case series of 24 patients with adnexal masses that approached with SILS. 11
The low rates of conversion to laparotomy are similar to the numbers reported by other researchers. Even in severe conditions with more technical difficulties, SILS has been accomplished successfully. 9
Conclusions
In this case series, it was possible to conclude that SILS is a viable technique for the approach of adnexal masses, particularly those of benign characteristics. SILS in the latest breakthough in minimally invasive surgery and could represent a significant gain for patients and health care systems, considering the costs of hospital stays.
Footnotes
Disclosure Statement
No competing financial conflicts exist.