
Abstract
Abstract
Introduction
O
These cases are generally misdiagnosed on ultrasonography, but, recently, a few researchers have reported their findings with respect to ovarian pregnancy, which may lead to early and correct diagnosis. 2
This article reports on a rare case of a ruptured ovarian pregnancy that was managed by ovarian wedge resection.
Case
A 26-year-old woman, gravida 2, para 1, was admitted in the current authors' ward with complaints of 4 weeks of amenorrhea.The patient had a history of pain in the abdomen and fainting attacks of 1 day's duration. Her past menstrual cycles were regular. She was married for 6 years, and had had her last childbirth 4 years ago. She was using Cu-T (copper-T) as a contraceptive measure, and was currently pregnant, as indicated by a positive urine pregnancy test.
This patient had pallor, her blood pressure was 110/70, and her pulse rate was 110 beats per minute. On abdominal examination, tenderness was noted over her entire lower abdomen. On bimanual examination, her uterus was noted to be anteverted and normal in size. Fullness was present in all fornices. An ultrasound test showed a complex echoic mass measuring 50×46 mm on the right side of the uterus with significant free fluid in the peritoneal cavity suggestive of a ruptured ectopic pregnancy. There was also presence of the Cu-T in the endometrial cavity.
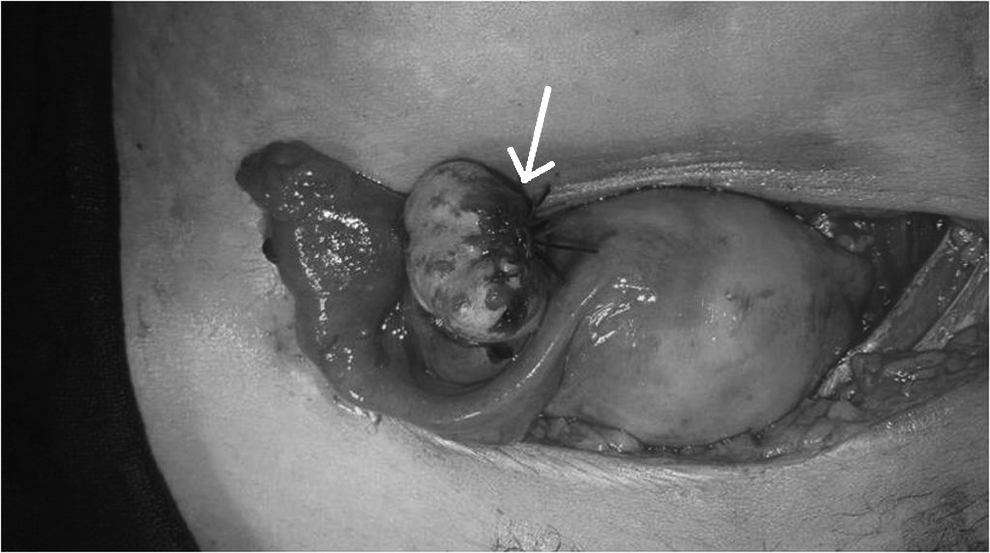
The patient was prepared for laprotomy in view of the diagnosis of a ruptured ectopic pregnancy. Intraoperatively, she was noted to have 800 mL of hemoperitoneum, which was drained, followed by identification of the site of the ectopic pregnancy. On inspection, the uterus and bilateral tubes appeared to be normal. A 3×3-cm, ruptured, ectopic gestational sac was seen on the right ovary with an active bleeding vessel (Fig. 1). Blood clots were removed followed by removal of the gestational sac by ovarian wedge resection (Fig. 2). Thereafter, ovarian reconstruction was performed (Fig. 3). The patient's left ovary was normal. Homeostasis was achieved. The Cu-T was removed.
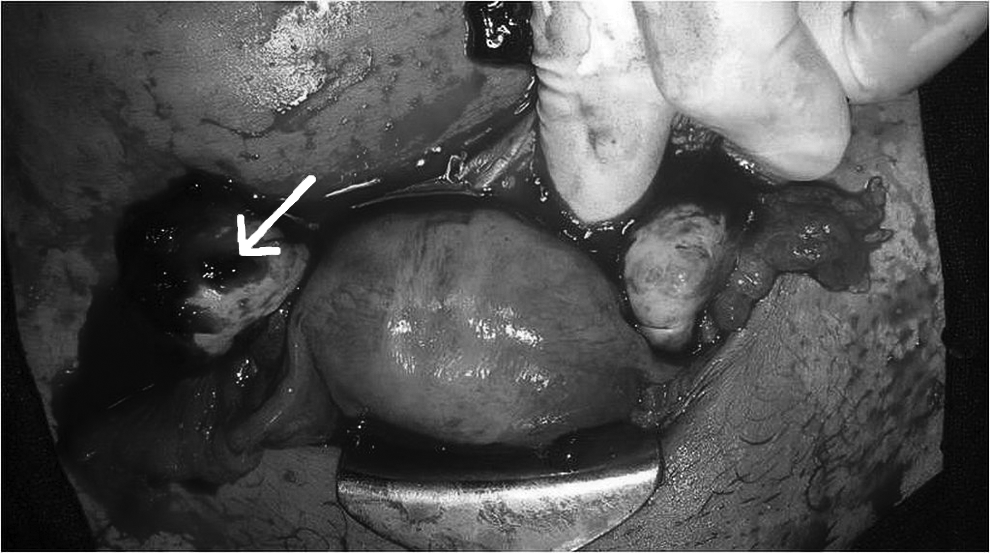
Ruptured right ovarian pregnancy (arrow).

Ruptured area after removal of products of conception (arrow).
Reconstructed ovary (arrow).
On histopathology, the excised ovarian mass showed hemorrhage, fibrin, chorionic villi, and trophoblasts, indicating ovarian implantation.
Results
The patient was discharged after 5 days. On follow-up, it was noted that she conceived after 6 months.
Discussion
Ovarian pregnancy is one of the rarest form of ectopic pregnancy. The first case was reported by St. Maurice as described by Farell and Abrams in 1682. 3 Primary ovarian pregnancy occurs if the ovum is fertilized when it still lies within the follicle. This phenomenon is postulated to be a consequence of ovulatory dysfunction. In a secondary ovarian pregnancy, there is tubal abortion followed by secondary implantation of the embryo in the ovary. Some researchers have suggested that these pregnancies rupture only at or after 8 weeks; however, the current patient had rupture of her ovarian pregnancy at 4 weeks. 4 The most common presenting symptoms include abdominal pain, vaginal bleeding, and amenorrhea, which is not unlike other ectopic gestations, although a patient with a ruptured ovarian pregnancy may present with a sole complaint of pelvic pain.
The initial diagnosis is generally made on the operating table, and the final diagnosis is made only on histopathology, on the basis of the four Spiegelberg criteria
5
:
(1) The gestational sac is located in the region of the ovary. (2) The ectopic pregnancy is attached to the uterus by the ovarian ligament. (3) Ovarian tissue in the wall of the gestational sac is proved histologically. (4) The tube on the involved side is intact.
De Seta et al. reported that pelvic inflammatory disease causes an increased risk of intrafollicular pregnancy because of hampered follicular dehiscence that induces reduction in tubal motility and thickening of ovarian albuginea. 6
The other risk factor associated with the development of ovarian pregnancy is the current use of an intrauterine device (IUD). An IUD is effective for preventing intrauterine and tubal pregnancies in 99.5% and 95% of women, respectively. However, it has little effect on the prevention of an ovarian pregnancy. 7 Raziel et al. reported that 90% of ovarian pregnancies occurred in IUD users. 8 The current patient was also using a Cu-T.
Other risk factors include endometriosis, 1 sexually transmitted disease, ovulation-induction agents, tubal sterilization, and a history of abdominal surgery. In addition, higher rates have been noted for African American females—rates that further increase progressively with age.
Several case reports have been published indicating a relationship between ovarian pregnancy and infertility treatments such as in vitro fertilization, embryo transfer, and intrauterine insemination. Common features in all of these procedures is enlargement of the ovary because of stimulation with gonadotropins. 9 Grimes et al. reported reproductive system pathology or infertility in >50% of 24 cases. 10 Unlike tubal pregnancy, for which there is a 15% chance of recurrence, no case of a repeat ovarian pregnancy has been reported, 10 which indicates that a previous ovarian pregnancy may not be a risk factor for its recurrence.
Several theories have been suggested to explain ovarian implantation, such as reflux of the conceptus following normal fertilization from the Fallopian tube along with blood from the uterus 11 or fertilization occurring within the follicule following defective ovum release at ovulation. 1 Given that ovarian pregnancy may result from in vivo fertilization of unrecovered oocytes, patients should be informed to avoid intercourse near the ovulation period. 12
Ovarian pregnancies are very unlikely to be diagnosed preoperatively, as they may resemble any other ovarian cyst. Hallat, in his study of 25 cases of ovarian pregnancies, reported that the most significant finding was the inability to distinguish an ovarian pregnancy from a hemorrhagic ovary or a ruptured corpus luteum. 1 These pregnancies are twice as likely to be diagnosed at surgery (mostly incidental, given that a patient is generally operated for a tubal ectopic pregnancy or a ruptured corpus luteal cyst) or following the pathologic diagnosis. 13
In the present case, the current authors suspected a ruptured tubal pregnancy preoperatively on the basis of a positive urine ß–human chorionic gonadotropin (ß-hCG) pregnancy test and ultrasonography findings.
Ovarian pregnancies could be misdiagnosed because they are mostly and easily confused with a ruptured corpus luteum. Diagnosis of ovarian ectopic pregnancy should be suspected when a hemorrhagic mass is identified near the ovary with a normal Fallopian tube noted during surgery for a suspected tubal ectopic pregnancy.
In the current case, to confirm the diagnosis of an ovarian ectopic pregnancy, tissue samples from the excised right hemorrhagic ovarian mass were sent for histopathologic examination. The presence of trophoblastic activity in the ovarian tissue confirmed an ovarian pregnancy.
Within the last decade, some researchers have described ultrasound findings in cases of ovarian pregnancy, and knowledge of this condition can increase the chance of early diagnoses by a radiologist. Comstock et al. reported a case series evaluating the ultrasonographic appearance of proven ovarian ectopic pregnancies. They showed a wide, echogenic ring with an internal echolucent area as compared to a thin tubal ring with tubal pregnancies or corpus luteum cyst; a yolk sac or fetal heart motion was also identified on occasion. 2
Patel et al. reported a rare case of a twin ovarian pregnancy that was diagnosed by ultrasound. 13 Other sonographic findings in various studies have included complex adnexal masses13,14; solid, cystic masses, with or without fluid in the cul de sac; fluid surrounding the ovary; and ovarian enlargement. Informed usage of transvaginal ultrasound (TVUS) can assist in making a correct definitive diagnosis of an ovarian pregnancy, helping to rule out a hemorrhagic corpus luteum or a tubal ectopic gestation. Even in circumstances in which ovarian pregnancy might not be expected—such as in a patient absent a history of tubal pathology, sterilization, endometriosis, infertility (or treatment thereof), prior ectopic gestation, nulliparity, and lack of IUD usage—appropriate studies, such as high-resolution TVUS and color Doppler complement bimanual examination, can enable a correct preoperative diagnosis of an ovarian gestation, potentially preventing rupture and thence a surgical emergency. 14
Conservative treatment, as in tubal pregnancy, is of the utmost importance if the patient is young and desires to bear children after an ovarian pregnancy. Methotrexate is an effective therapeutic option for managing an unruptured ovarian ectopic pregnancy, which, however, is diagnosed rarely. 15 In the past, oophorectomy had been advocated as a treatment for ovarian gestations, but ovarian cystectomy is now the preferred procedure. 13 The current authors used wedge resection of the ovary to conserve fertility in the current patient. Patients with ovarian pregnancy could have a good prognosis for future fertility, therefore conservative surgical management, as in the current case, is advocated.
The diagnosis of ovarian pregnancy is difficult and is a continuing challenge to gynecologists and surgical practitioners. Ovarian rupture destroys the integrity of the organ and occasionally, that of the Fallopian tube, preventing recognition of such a gestation. In delaying the diagnosis, there is the danger of rupture, secondary implantation, and difficulties during surgery. Moreover, early detection of an ovarian pregnancy permits surgery and excision of the ectopic pregnancy without excessive removal of healthy ovarian tissue. Therefore, although ovarian pregnancy is a rare event, awareness of this condition is important for reducing its associated morbidity and mortality.
Conclusions
It can be concluded that ovarian ectopic pregnancy should be considered as one of the important differential diagnoses in a female of reproductive age presenting with an acute abdomen with early amenorrhea. Diagnosis of ovarian pregnancy should be suspected in high-risk patients with elevated ß-hCG, lack of intrauterine gestation, and/or a complex ovarian mass seen on ultrasonography.
Footnotes
Disclosure Statement
No competing financial conflicts exist.