
Abstract
Abstract
Introduction
H
Atypical endometrial cells microscopically appear as isolated cells or as rounded clusters of cells with enlarged nuclei and at least one other characteristic of nuclear atypia, such as membrane irregularity and prominent nucleoli. In these cells, the cytoplasm can be minimal to moderate and it is vacuolated. 2 Atypical endometrial cells carry a significant risk for cancer; their presence is suspicious for adenocarcinoma.
Endometrial carcinoma can be characterized as either type I or type II. Type I, which comprises >80% of cases, is more common among women ages 55–65 in the clinical setting of unopposed estrogen, obesity, hypertension, and diabetes. 3 Type I has an endometrioid morphology and the typical precursor is hyperplasia. Type II is more common among women ages 65–75 in the clinical setting of atrophy and thin physique. Type II's morphology may be serous, clear cell, or mixed Müllerian tumors. The precursor tends to be endometrial intraepithelial carcinoma, and Type II has an aggressive course.
Patients with endometrial hyperplasia may initially present with abnormal vaginal bleeding that is investigated via endometrial biopsy and histopathologic identification. 4 Alternatively, in patients undergoing transvaginal ultrasound, findings may include a thickened endometrial stripe. This may then prompt an endometrial biopsy and lead to histopathologic identification of endometrial hyperplasia. 4 In postmenopausal women, the threshold value for serious endometrial abnormalities on transvaginal ultrasound is 5 mm. 5 Although office endometrial biopsy has generally replaced dilation and curettage (D&C) for diagnosis of endometrial hyperplasia or carcinoma, D&C may still be useful as therapy or as a way to provide more tissue for accurate histologic diagnosis. 4
Endometrial hyperplasia can be pathologically classified into one of the following groups: simple hyperplasia without atypia; complex hyperplasia without atypia; simple hyperplasia with atypia; and complex hyperplasia with atypia. 4 Atypia is the most important criterion for progression to adenocarcinoma or coexistence of endometrioid adenocarcinoma. 4 Adenocarcinoma was found in the uteri of 43% of enrolled participants at the time of hysterectomy in one study. 4
What follows are two cases involving novel hysteroscopic findings in the context of endometrial nuclear atypia.
Cases
Case 1
A 73-year-old postmenopausal female, gravida 3, para 3002, with a history of hypertension, osteoarthritis, dyslipidemia, and diverticulitis presented with fullness in the right lower quadrant of her abdomen. She weighed 136 lbs, with a body mass index (BMI) of 24.1, and was 5′3″ tall. Her pulse was 60 beats per minute (bpm) and her blood pressure (BP) was 146/84 mm Hg. On pelvic examination, she was found to have a mildly enlarged uterus (6 weeks' size). She had a thickened endometrium (9.4 mm), an intrauterine myoma, and an endometrial polyp noted on transabdominal and transvaginal ultrasounds. An outpatient endometrial biopsy was attempted, but was unsuccessful due to this patient's cervical stenosis. She underwent hysteroscopy and D&C.
Case 2
A 61-year-old obese, postmenopausal female, gravida 4, para 0040, had a history of leiomyomata uteri (removed during a previous myomectomy), 2 ectopic pregnancies (2 previous diagnostic laparoscopies and salpingectomies), human papilloma virus, hypertension, and hypothyroidism. She presented with postmenopausal bleeding. She described this bleeding as spotting that occurred after a routine pelvic examination. She weighed 185 lbs, with a BMI of 30.8, and was 5′5″ tall. Her pulse was 67 bpm, and her BP was 125/88 mm Hg. On ultrasound testing, it was noted that her endometrium was slightly irregular, but appeared to be normal in texture (hyperechoic) and thickness (4.8 mm). A pelvic examination showed that she had a healthy cervix and an 8–10 weeks' size uterus with a deviation to the left. She elected to undergo a procedure under anesthesia instead of an outpatient endometrial biopsy. Therefore, she underwent hysteroscopy, D&C, and a directed biopsy from the lesion.
Results
Case 1
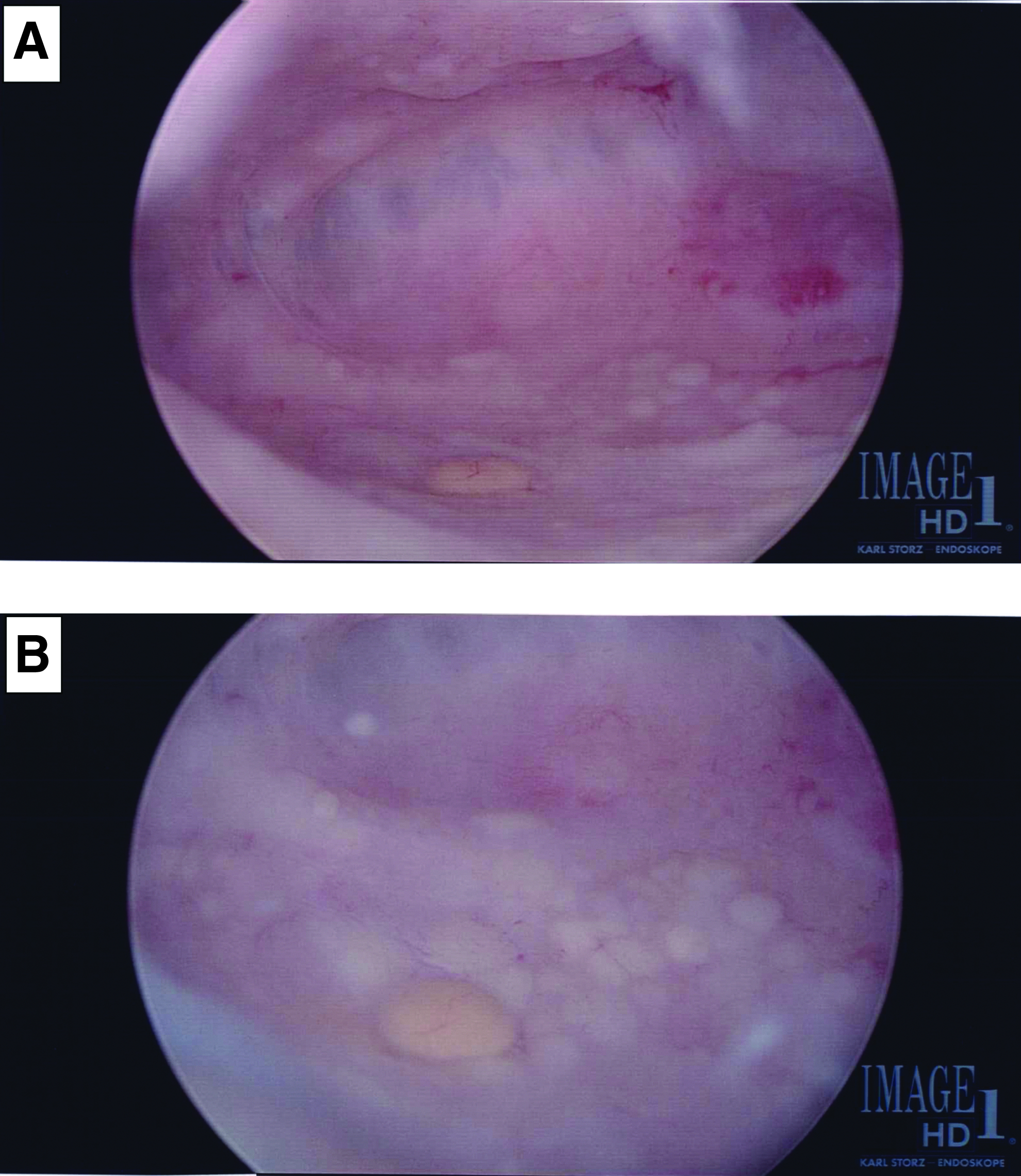
Hysteroscopy showed the presence of numerous small, round, yellow, and faint light yellow, slightly elevated lesions in the endometrial cavity and a submucal myoma (Fig. 1). Histopathologically, it was noted that there were scanty fragments of superficial endometrial endothelium with focal, marked nuclear atypia, but a p53 immunostain was inconclusive.

Hysteroscopic findings in Case 1.
The patient chose to undergo a robotic total abdominal hysterectomy and bilateral salpingo-oophorectomy. The endometrial cavity of the uterine specimen was tan–red, and there was a diffusely irregular endometrium measuring 0.2–0.5 cm in thickness. There was a 2.5×2×1–cm subserosal leiomyoma on the right aspect of the uterus. There also were many intramural leiomyomas, measuring 0.2–1 cm.
Case 2
Hysteroscopy showed numerous small, round, yellow, slightly elevated lesions in the endometrial cavity (Fig 2). Histopathologically, mitotic figures were identified within a fragment of proliferative endometrium. There were also fragments of a leiomyoma and a polypoid fragment of endometrium with features suggestive of an endometrial polyp.
Hysteroscopic findings in Case 2.
This patient also elected to undergo robot-assisted hysterectomy and bilateral salpingo-oophorectomy. No other diagnosis was made on frozen section. The endometrium of the uterine specimen measured 0.1 cm in thickness. There were many intramural and calcified subserosal leiomyomas; the largest subserosal leiomyoma measured 4×3×2.5cm. There were no areas of hemorrhage or necrosis, and no other diagnosis was made on frozen section.
Summary of both cases
Both patients did not want conservative therapy and long-term follow-up. Both patients elected to undergo robotic-assisted total abdominal hysterectomy and bilateral salpingo-oophorectomy.
Discussion
On hysteroscopy, it was noted that these 2 patients had yellowish lesions in their endometrial cavities. Biopsies of these lesions showed the presence of atypical endometrial cells. It is possible that these characteristic hysteroscopic findings were associated with endometrial nuclear atypia.
In one retrospective and descriptive study, Pato-Mosquera et al. found that the correlation between hysteroscopic findings and histopathologic diagnosis was 77.7% for normal endometrium, 77.9% for polyps, 17.8% for hyperplastic appearance, and 100% for carcinoma suspicion. The authors concluded that, in spite of the generally good relationship between hysteroscopic visual inspection and anatomopathologic diagnosis, biopsy should be performed. 6
In one prospective study of patients admitted with histories of abnormal uterine bleeding, Patil et al. demonstrated the following hysteroscopic findings: proliferative 34%; secretory 16%; hyperplasia 18%; atrophic 8%; endometrial polyp 9%; submucosal myoma 11%; carcinoma of endometrium 3%; and misplaced Copper-T 1%. The authors concluded that, in patients with abnormal uterine bleeding, hysteroscopy provides a more accurate diagnosis than D&C. Among patients with hyperplasia, the endometrium appeared to be thickened, edematous, and undulating on hysteroscopy. 7
Another study suggested that hysteroscopic features of endometrial hyperplasia include focal or extensive endometrial thickening, irregular vascular network, architectural distortion and crowding of gland openings, and gland cyst formation. 8 Yet another other study suggested that hysteroscopic features of endometrial carcinoma include polypoid proliferations that appear cerebroid with ulceration, necrosis, friability, and irregular vessels. 9 However, these features may be missed in focal neoplasias or within endometrial polyps. 9
In one study, Barati et al. described a case of endometrial hyperplasia with atypia, which hysteroscopically appeared as obvious white endometrial elevations in the endometrial lining. However, the authors also noted that pathologic diagnosis of hyperplasia is possible even in patients without obvious lesions on hysteroscopy, so biopsy was still advised. 10
Although the current cases also had elevated endometrial lesions on hysteroscopy, these lesions were yellowish and associated with atypia without hyperplasia. Outpatient endometrial biopsy might miss these lesions.
As described above, the presence of atypical endometrial cells is suspicious for adenocarcinoma. Among patients found to have atypical endometrial hyperplasia (AEH), a hysterectomy should be performed if fertility is not desired. With AEH, there is a 20%–45% risk of underlying malignancy, and hysterectomy is required for final diagnosis. If malignancy is found, another surgical procedure may be needed for comprehensive surgical staging and removal of retained ovaries. 4
If a woman with AEH desires childbearing, refuses hysterectomy, or has a medical condition that makes hysterectomy undesirable, she should be treated hormonally. In this case, the drug of choice is 160 mg/day of megestrol in divided doses. The endometrium should be reevaluated histologically at 3-month intervals for at least 1 year. Before endometrial biopsy, the patient should be withdrawn from progesterone for 7–14 days to allow withdrawal bleeding, and biopsy or D&C should be scheduled after bleeding stops. 4 A potential alternative hormonal treatment consists of a progestin-containing intrauterine device. 4
Both patients, because of their hysteroscopy-detected lesions, underwent very vigorous D&C procedures. Their endometria showed the presence of nuclear atypia. Several weeks later both patients elected to undergo hysterectomy, and because of the vigorous D&C procedures that had been performed, the hysterectomy specimens did not show atypical endometrial cells.
In a systematic review and meta-analysis, Polyzos et al. 11 found that hysteroscopy detected a significantly higher rate of malignant peritoneal cytology and significantly higher disease upstaging because the presence of malignant cells was noted in the peritoneal cavity, compared with no use of hysteroscopy. De Sousa Damião et al. suggested otherwise in a prospective longitudinal study showing that diagnostic hysteroscopy performed under low pressure CO2 (≤80 mm Hg) does not cause spreading of endometrial cells into the peritoneal cavity for patients with early stage endometrial cancer. 12 In addition, in a retrospective cohort analysis of women diagnosed with endometrial cancer, Soucie et al. found that hysteroscopy is not associated with a higher rate of stage III disease or mortality. 13
Conclusions
On hysteroscopy, it was noted that these 2 patients had yellowish endometrial lesions, and biopsy revealed the presence of atypical cells. These characteristic hysteroscopic findings may possibly be associated with endometrial nuclear atypia. It would be useful to investigate similar hysteroscopic findings via histopathology.
Footnotes
Disclosure Statement
No financial conflicts exist.