
Abstract
Abstract
Introduction
P
Case
A 46-year-old woman (gravida 5 para 4), was presented with symptoms of abdominal discomfort, bloating, and a palpable abdominal mass. Abdominal examination revealed a large, mobile, nontender firm mass, extending up to the level of the umbilicus. The patient's vaginal examination was unremarkable.
In 2004 she had undergone subtotal laparoscopic hysterectomy, because she had a fibroid uterus and menometrorrhagia. During that operation, a morcellator was used to extract the 495-g uterus. Shortly after the primary surgery, this patient underwent a culdotomy and drainage of an infected vault hematoma. The remaining postoperative course was unremarkable. She had no previous illnesses and was not using any type of medications.
Blood test results, including tumor markers, were normal, and serial normal Papanicolaou smear results were negative for dysplasia. A computed tomograpy scan was performed, showing a 15×18–cm mass with radiologic characteristics of a fibroid growth and several nodules measuring 3–4 cm with a similar appearance located in the abdominal cavity. Small retroperitoneal and right axillary lymph nodes were also noted. Bilateral mild hydronephrosis and bladder compression by the large abdominal mass were noted. The patient had a magnetic resonance imaging (MRI) scan, which confirmed these findings, revealing a large mass with no connection to the cervix or to the urinary bladder, and additional four smaller masses. No enlarged lymph nodes were seen on the MRI scan (Fig. 1).
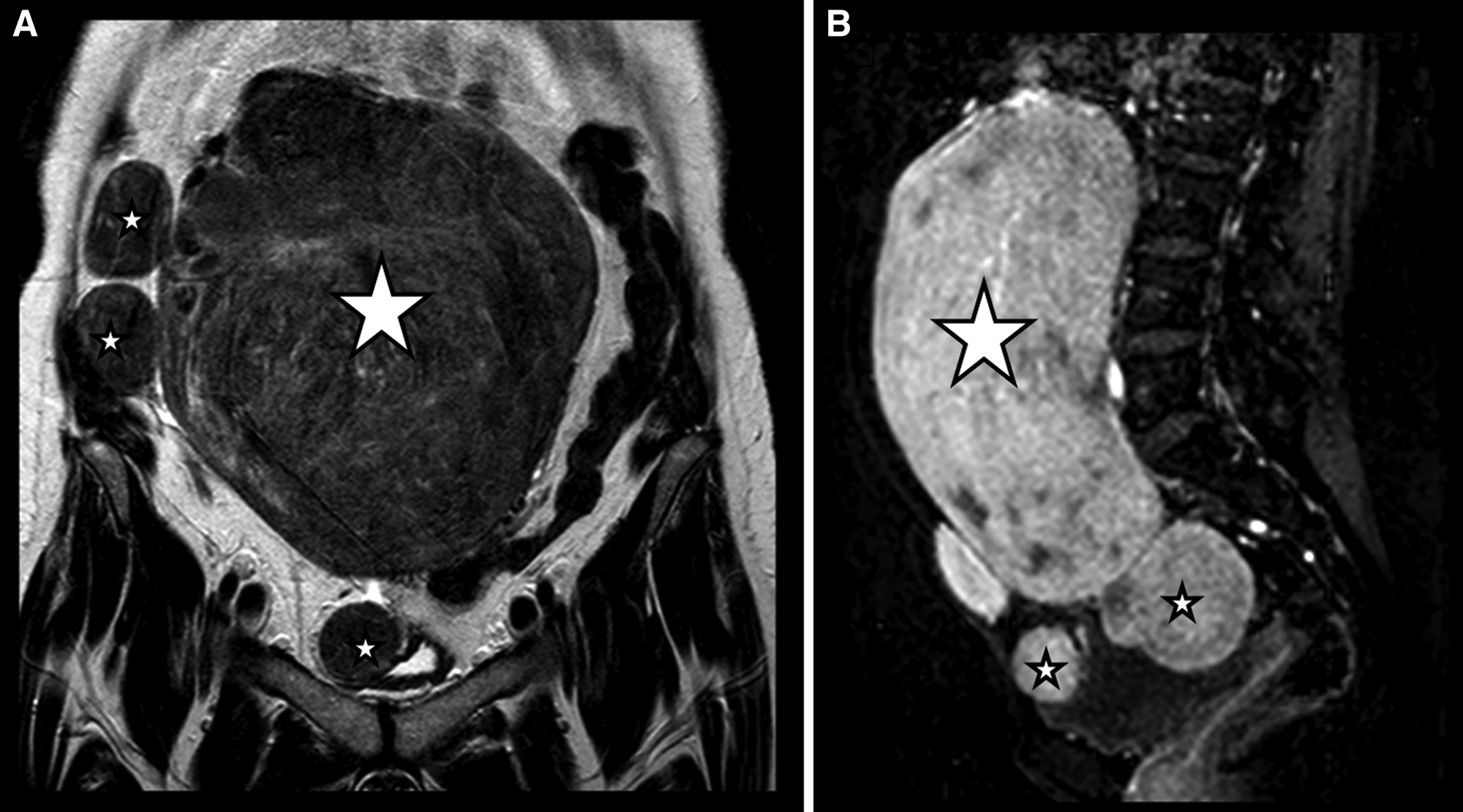
Magnetic resonance imaging scan showing an enlarged parasitic myoma (large star) and several smaller nodules measuring 3–4 cm (small stars).
Right axillary fine needle aspiration showed no signs of malignancy. Based on these clinical findings, a consultation with a gynecologist–oncologist recommended an explorative laparotomy with a frozen-section pathologic examination. The working diagnosis was of parasitic myomas.
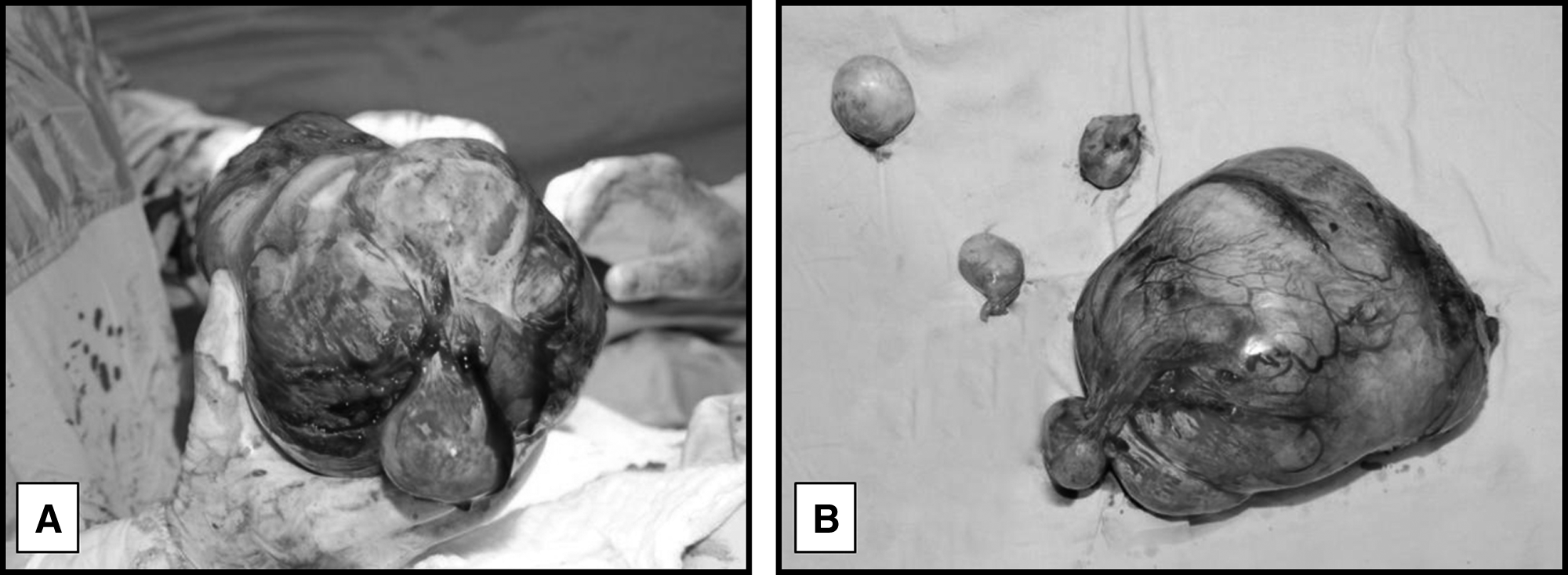
Subsequently, the patient underwent an explorative laparotomy. A mass measuring 23×16×13 cm was excised from the posterior abdominal wall. The mass was obtaining its blood supply from the sigmoid colon and the posterior abdominal wall. Four discrete myomalike masses, measuring 4–5 cm each, were also identified and excised carefully. The total weight of the excised masses was 2650 g (Fig. 2). None of the masses were attached to the uterine cervix stump. Intraoperative frozen section revealed leiomyoma, a diagnosis which was subsequently confirmed by a postoperative pathologic examination of the whole specimen.
Results
The patient's postoperative hospitalization was uneventful, and she was discharged 3 days post operation.
Discussion
Leiomyoma is the most common benign uterine tumor, found in about 25% of women in reproductive age and in as many as 80% of surgically excised uteri.4,5 These benign masses are monoclonal tumors, originating from the smooth-muscle layer of the uterus. Myomas are often asymptomatic, although some may cause symptoms, such as abnormal uterine bleeding, abdominal pain and discomfort, urinary complaints, dyspareunia, and infertility. 6 The classification of myomas is derived from their location in relation to the uterine-wall layers: submucosal; intramural; and subserosal. There are also pedunculated myomas—either submucous or subserous. 1
A rare form of leiomyoma is a parasitic myoma, classically defined as a myomatous mass detached from the uterus and receiving its blood supply from adjacent pelvic or abdominal organs. 1 The main presenting symptoms of parasitic myomas are pain and abdominal discomfort, rather than uterine bleeding, which is typical for uterine myomas. Of note, because of the rarity of this entity and these nonspecific symptoms, in some cases, the diagnosis of parasitic myoma has not even been considered preoperatively. Parasitic myomas can reach considerable dimensions, and previous reports describe masses up to 25–30 cm.1–3,7
When reviewing the literature concerning this entity, three hypotheses for the formation of parasitic myomas are proposed: (1) Diminished uterine blood supply—either spontaneous or iatrogenic; (2) de-novo formation; and (3) postoperative seeding of myoma fragments, mainly attributed to morcellation. 2
The “classic” appearance of parasitic myomas was first described in 1909, when Kelly and Cullen presented a series of 37 cases of parasitic myomas. 1 Their definition of this entity was “myomata that have for some reason become partially or almost completely separated from the uterus and receive their main blood supply from another source.” They also posed an illustrative description of the process by which the uterus gradually attempts to rid itself of myomas by contracting and extracting them to its outermost layer, while the myomas seek an alternative blood supply until their main blood supply comes from another abdominal organ, mainly the omentum, while they are detached from the uterus.
It is assumed that relative hypoxia of the distal part of the myoma promotes generation of growth factors, enhancing proliferation of blood vessels and adherence to adjacent structures, gradually leading to the creation of a new independent blood supply. Necrosis or torsion of the stalk of the pedunculated myoma, detaches it from the uterus, leaving it to become “parasitic” to the adjacent structures. It is noteworthy that, some of the myomas classically labeled as “parasitic,” were indeed pedunculated myomas, receiving their blood supplies from both the uterus and adjacent organs. Only some of these myomas were separated fully from the uteri. 1
Parasitic myomas were also described following the use of a gonadotropin-releasing hormone agonist, 7 and following magnetic resonance–focused ultrasound for management of symptomatic myomas. 2 Both treatment modalities are aimed at reducing blood supply to the myoma, in order to decrease its size. However, they can, paradoxically, result in hypoxia and eventually lead to detachment of the myoma from the uterus. The same mechanism was suggested (by Kho and Nezhat 7 ) after uterine artery embolization—another treatment for reducing blood supply to the myoma; however, no case reports of this mechanism were published.
A second possible mechanism for the formation of parasitic myomas involves de novo differentiation and proliferation of pluripotent stem cells. These cells, derived from embryonal remnants of the Müllerian or Wolffian ducts, supposedly form distant leiomyomas—located intraperitoneally, retroperitoneally, or even extra-abdominally.8,9
In the last decade there has been an increase in reports suggesting a probable novel etiology for parasitic myomas—an iatrogenic seeding of leiomyoma fragments during operative procedures, mainly when morcellation was carried out.2,3,7
Advances in operative techniques are bringing about a rise in the popularity of minimally invasive surgery, which results in the need to extract large masses through small incisions. For that purpose, morcellators were developed ∼15 years ago. These instruments are designed to shred tissue by mechanical (blade) or bipolar energy. This technique, however, caries a potential of seeding tissue fragments in the peritoneal cavity. 10
Postmorcellation parasitic myomas may be found throughout the pelvic and abdominal cavity.2,3 Some postmorcellation parasitic myomas arise in sites that are specific to the operative technique, such as trocar sites following laparoscopy11,12 and the vaginal vault after a vaginal hysterectomy with morcellation. 13 Postmorcellation parasitic myomas vary in size and are often multiple.2,3
The occurrence of postmorcellation parasitic myomas after myomectomy was evaluated in two studies. An Italian group examined 321 cases of patients who underwent laparoscopic myomectomy with morcellation during a 3-year period and detected 4 cases (1.2%) of postmorcellation parasitic myomas. 3 A Norwegian group showed a 0.12% occurrence—3 cases of 2470 operations during an 8-year period. 14
The shift in the etiology and presentation of parasitic myomas from “classical” large myomas, to postoperative—usually multiple—parasitic myomas, is attributed to differences in both imaging and operative techniques. In previous years, the diagnosis of myomas was more challenging, resulting in delayed medical care. Thus, many patients presented with large neglected myomas, which gradually evolved to be parasitic myomas. At present, imaging modalities, especially ultrasound, are widely available for routine follow-up or on-demand examinations, and many women undergo at least one imaging study during their reproductive years and around pregnancies. This high prevalence of imaging studies results in earlier diagnosis of myomas and other intra-abdominal pathologies, sometimes even as asymptomatic incidental findings. Early diagnosis and intervention may prevent progression toward parasitic mymoas. However, intervention has its toll, as presented above, in the form of the new etiology of postmorcellation parasitic myomas.
Morcellation has also been discussed in the literature for its possible association with spreading of endometriosis 15 and leiomyosarcoma. 16 Recently, the U.S. Food and Drug Administration has issued a warning regarding the use of morcellation and the risk of spreading undetected cancerous tissue in women with unsuspected malignancies. 17 The American College of Obstetricians and Gynecologists (ACOG) and the Society of Gynecologic Oncology (SGO) have addressed this issue, stating that, although morcellation enables the use of minimally invasive procedures for hysterectomy and myomectomy, morcellation is generally contraindicated in the presence of malignancy or high suspicion for malignancy, and in premalignant conditions. Both the ACOG and the SGO advocate careful patient selection, physician training, and considering use of intraperitoneal bags during operation. These organizations also recommend advising patients about the potential risk of seeding undiagnosed cancerous tissue, as well as the possibility for dissemination of ectopic benign tissue (leiomyoma, endometriosis, etc.), requiring additional subsequent interventions.18,19
Conclusions
Postmorcellation parasitic myomas comprise an increasingly reported novel entity, which is most commonly iatrogenic in origin. Awareness of the possibility of this postoperative complication may diminish its prevalence, by enabling suitable precautions. The current authors agree with the recommendations of other authors emphasizing the importance of removing all fragments of tissue completely following morcellation, ensuring adequate irrigation, and thorough pelvic and abdominal cavity inspection. Trocar sites and the abdominal wall should also be examined carefully. Furthermore, morcellation within an endoscopic bag, although technically challenging, has also been proposed.2,3 Careful preoperative patient evaluation and patient selection, including assessing the risk for an occult malignancy, are also advised.17–19 These measures may prevent future discomfort for the patient and alleviate the need for additional surgery and further morbidity.
Footnotes
Disclosure Statement
None of the authors have a conflict of interest.