
Abstract
Abstract
Introduction
H
Several risks are associated with hysterectomy, including chronic postoperative pain. Chronic postoperative pain is a phenomenon developed in a high number of patients after surgery, including amputation, breast surgery, thoracotomy, inguinal hernia repair, mastectomy, caesarean section, and, as mentioned, hysterectomy. 7 Chronic postoperative pain following large surgical procedures such as amputations and thoracotomy holds an estimated incidence rate of 30%–50%.8–10 However, smaller surgical procedures such as hernia repair also pose a significant risk of developing chronic postoperative pain since an estimated incidence has been found to be 10%–30%.11–13 Chronic postoperative pain is observed in 4.7%–31.9% of the cases after conventional hysterectomy (abdominal, vaginal, laparoscopic, and laparoscopic-assisted vaginal hysterectomy).14–24
Patients affected by chronic postoperative pain report decreased quality of life. 25 Since chronic postoperative pain is a clinical challenge to manage adequately, risk factors are important to elucidate to prevent this condition. Women experiencing preoperative pain and a high intensity of acute postoperative pain are at high risk of developing chronic postoperative pain.26,27 Minimally invasive surgery has the potential of reducing morbidity and blood loss, shortening hospital stay, and reducing acute postoperative pain.28–30 In addition, minimally invasive surgery is able to reduce nerve injury during surgery, which may play an important role in the development of chronic postoperative pain. 11 However, it is still uncertain whether robot-assisted laparoscopic hysterectomy can reduce the development of chronic postoperative pain.
The aims of this study were to investigate and compare (1) the developing chronic postoperative pain after robot-assisted laparoscopic hysterectomy and after abdominal hysterectomy and (2) potential risk factors for developing chronic postoperative pain after hysterectomy.
Materials and Methods
Study design
This cross-sectional study included women who had undergone hysterectomy at Aalborg University Hospital, Denmark, and had been identified by the Danish Gynecologic Cancer Database (DGCD). DGCD contains information about Danish gynecologic cancer patients diagnosed since January 01, 2005. DGCD covers information such as patient history, gynecology, pathology, oncology, and nursing aspects. Inclusion criteria were women who had undergone abdominal or robot-assisted laparoscopic hysterectomy on the basis of a malignant tumor in the corpus uterus. Moreover, the surgical procedure must have been performed in the period from January 01, 2010 to December 31, 2012. Exclusion criteria were major complications, conversion to abdominal surgery (for robot-assisted laparoscopic surgery), mental disorders and dementia, or relapse in the operational follow-up period. The study was performed in accordance with the declaration of Helsinki and was conducted in agreement with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 31
The questionnaire
The questionnaire was structured in two parts: The first contained questions related to the preoperative period, and the second was related to the postoperative period. The following variables were collected: presence of preoperative pelvic pain, chronic postoperative pain, pain intensity ratings by numeric rating scale (NRS), frequency of the pain, location of the pain, and the effect of the pain in everyday activities. Chronic postoperative pain was defined as suffering from constant or periodical pain for at least 3 months. 23 The questionnaire was controlled for validity in a pilot study. A questionnaire was mailed with a pre-paid envelope and sent to each patient. To ensure a high response rate, each unresponsive subject was contacted by phone 3 weeks later. Two weeks after the phone call, all letters were gathered for data collection. In addition, questionnaires may introduce a risk of bias regarding misunderstandings among the women answering the questions. This was addressed by contacting women by phone whenever there was an indication of misapprehension among the answers in a questionnaire.
Danish Gynecologic Cancer Database
DGCD was used to collect the following variables for each woman: (1) number of comorbidities before operation; (2) type of comorbidities before operation; (3) body mass index (BMI) at the time of operation; (4) the duration of the operation (minutes); (5) blood loss during operation (mL); (6) any type of intraoperative lesions to the bladder, ureters and bowel; (7) number of births; and (8) date of operation.
Statistical analysis
Continuous data were displayed as mean and categorical data as frequency (percentage). The sample size was defined by the number of eligible women who had undergone hysterectomy at Aalborg University Hospital in the period from 2010 to 2012. To detect any potential confounding factors between the two surgery groups, which could affect the development of pain, an analysis of demographic and clinical factors was performed. The demographic factors were age (years), education level, and employment status. The clinical factors were BMI, number of births, preoperative pelvic pain, preoperative pain elsewhere (e.g., head, neck or knees), comorbidities before operation, and time since operation. Each of these factors was compared in a Mann–Whitney U test for continuous data and a chi-squared test for categorical data between the two surgical procedures (abdominal and robot-assisted laparoscopic hysterectomy). Afterward, the following surgical outcomes were evaluated: acute postoperative pain intensity (NRS), duration of operation (minutes), and blood loss during operation (mL). These variables were also analyzed using the Mann–Whitney U test for continuous variables with type of surgery as the independent factor and the chi-squared test for categorical variables.
To detect potential risk factors for chronic postoperative pain, a binary logistic regression was performed with the following independent factors: type of surgery, acute postoperative pain intensity (NRS), preoperative pelvic pain, preoperative pain elsewhere, and age (years). The statistical analyses were performed with IBM SPSS Statistics software for Windows, Version 22.0. (IBM Corp., Armonk, NY).
Results
Two hundred twenty-eight women received letters containing a questionnaire, and 177 returned the questionnaire during the 5-week period. Of the 228 posted questionnaires, 17 were never returned even though the women were reminded by telephone. Furthermore, 26 women were unreachable as they never responded either to letters or to any contact by telephone. Eight women refused to participate in the questionnaire due to various reasons (e.g., severe illness, personal matters). Figure 1 illustrates a flowchart of the questionnaire response from participants. Only six incidences of missing data were encountered, accounting for 0.09% of the total amount of questions. Baseline characteristics can be found in Table 1.
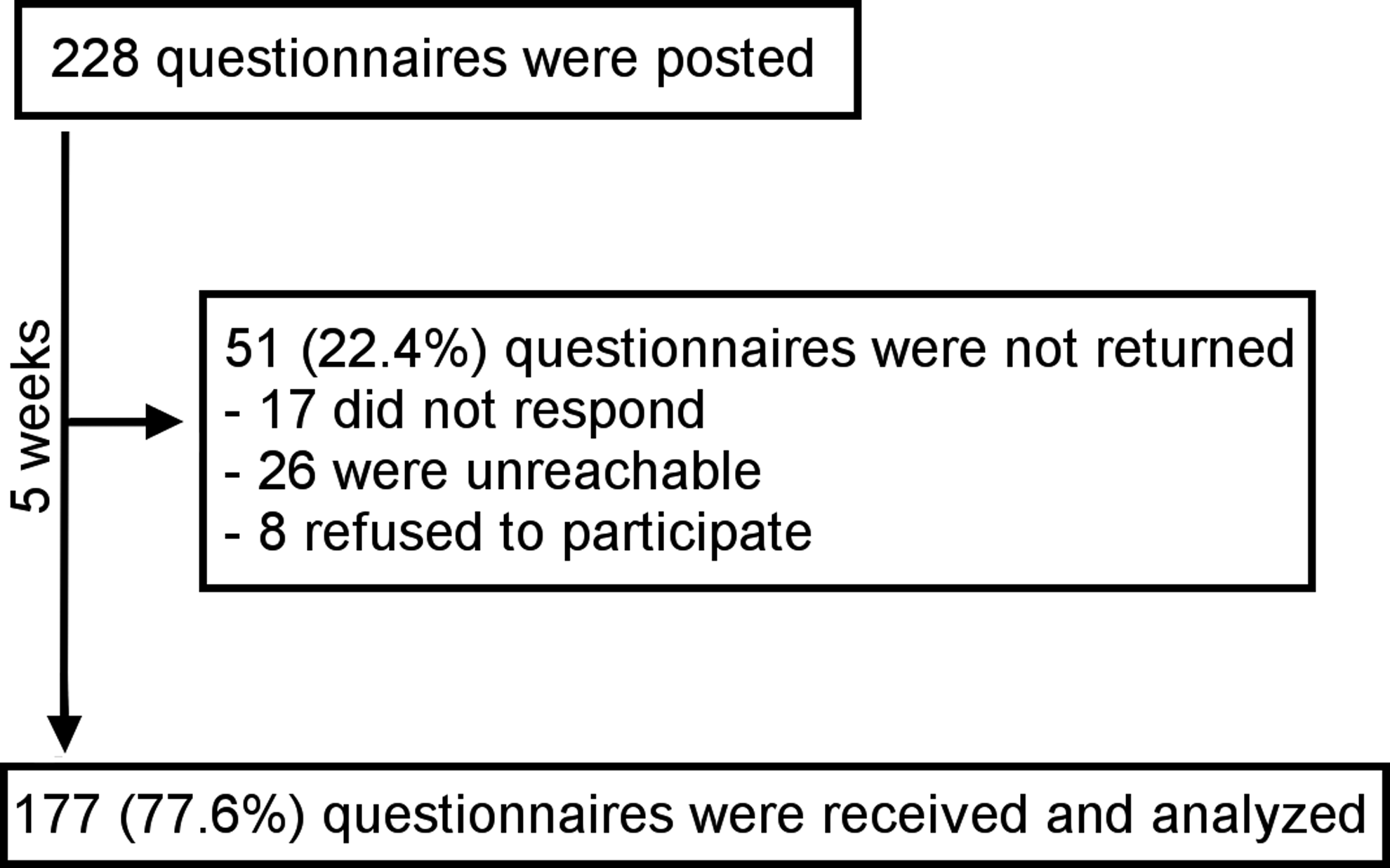
Flowchart of the questionnaire response from all the mailed hysterectomized women.
BMI, body mass index.
Pain characteristics
Overall, 32 women (18.1%) suffered from preoperative pain and 24 women suffered (13.6%) from chronic postoperative pain (Table 2). The average pain intensity was 4.44 (range 3.7–5.2) and 3.54 (range 2.7–4.3) for preoperative and chronic postoperative pain, respectively. Furthermore, the highest pain intensity was 6.19 (range 5.2–7.2) and 5.30 (range 4.3–6.4) for preoperative pain and chronic postoperative pain, respectively. In most cases, the pain was experienced either 1–3 days/week or daily. The prevalence of experiencing pain in specific situations was almost similar between preoperative pain and chronic postoperative pain, with heavy lifting as the most prominent factor. However, pain during sexual intercourse seemed to be less frequent in women with chronic postoperative pain. Chronic postoperative pain locations were reported by the women, and the reports show that especially dermatome T12-L3 and S2-4 are affected by the postoperative pain (Fig. 2).
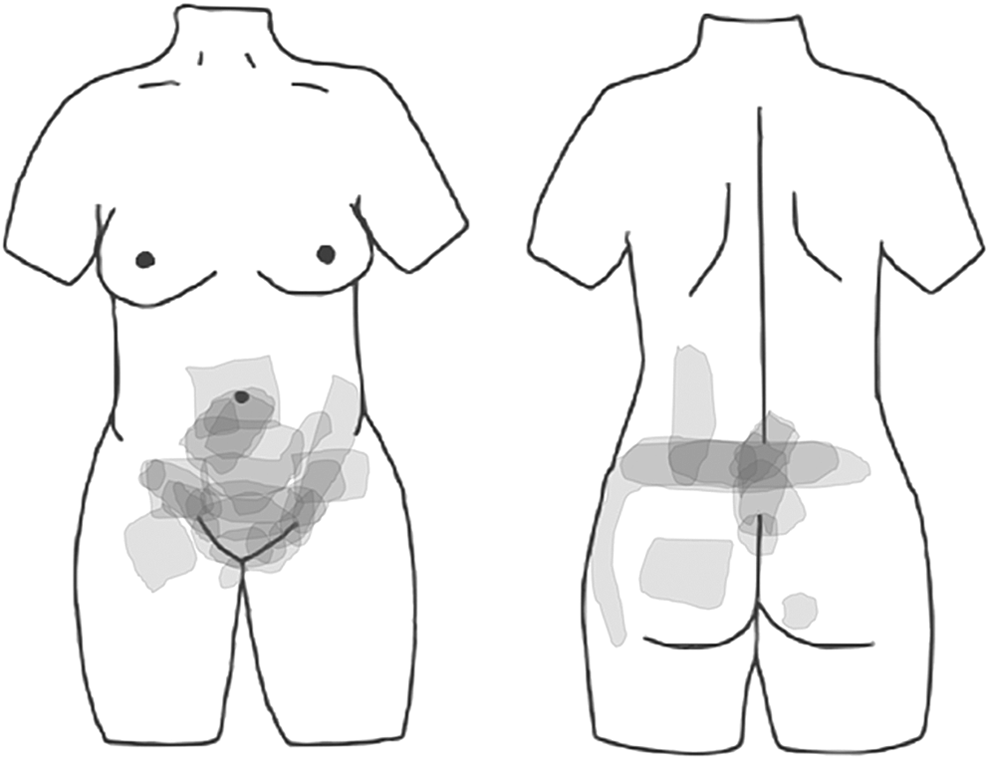
The gray areas illustrate the pain locations where the women experience chronic postoperative pain. The intensity of the color is proportional with the frequency of women reporting similar pain location. These summarized illustrations have been drawn by 22 of the 24 women suffering from chronic postoperative pain.
Data are represented as n (%) for categorical data and mean (95% CI) for continuous data.
Ten (41.7%) of these 24 women did not experience preoperative pelvic pain.
Based on the mean age of the study sample.
Based on the mean BMI of the study sample.
CI, 95% confidence interval.
Postoperative outcomes
The following demographic factors were analyzed between groups: age (years), BMI (kg/m2), number of births, current job status, and education level. No significant differences were found between groups. However, it is important to note that a higher BMI tendency was observed in the robot-assisted laparoscopic hysterectomy group (p=0.063). The most common education level in both surgical groups consisted of women who had completed elementary school followed by women with a vocational education (Table 3). Number of comorbidities before operation, number of days before the follow-up after the surgery, preoperative pelvic pain, and preoperative pain elsewhere (e.g., head, neck or knees) were compared among groups. The number of days after surgery was found to be significantly different between the two surgical groups (p≤0.01) with the mean being 1103.98 and 950.70 days for abdominal and robot-assisted laparoscopic hysterectomy, respectively.
Data are represented as n (%) for categorical data and mean (95% CI) for continuous data.
p≤0.01.
p≤0.001.
Chi-squared analysis not performed, as these two variables (postoperative chronic pain and type of surgery) are included in the logistic analysis.
The operation time (minutes) and blood loss during surgery (mL) were found to be significantly different between the two surgical groups (p<0.01 and p<0.00, respectively). Robot-assisted laparoscopic hysterectomy had a longer operation time compared with abdominal hysterectomy, whereas blood loss was markedly lower (Table 3). Furthermore, the acute postoperative pain intensity after robot-assisted laparoscopic hysterectomy was significantly reduced in contrast to abdominal hysterectomy (p<0.00).
Risk factors for chronic postoperative pain
The type of operation (abdominal or robot-assisted laparoscopic hysterectomy) was not a significant risk factor for development of chronic postoperative pain (Table 4). The intensity of the acute postoperative pain was found to be a significant predictor for development of chronic postoperative pain (p<0.05) with an odds ratio of 1.27 (confidence interval [CI] 1.05–1.53). Thus, high pain intensity after hysterectomy was associated with an increased risk of chronic postoperative pain. The presence of pelvic pain before the operation was also observed as posing a higher risk of developing chronic postoperative pain (p<0.05) with an odds ratio of 3.56 (CI 1.17–10.87). The age of the patient showed (p=0.05) that the risk of developing chronic postoperative pain decreases with age. Preoperative pain elsewhere (e.g., head, neck, or knees) was not a significant predictor for the development of chronic postoperative pain.
The dependent variable is postoperative chronic pain. Variable nos. 1, 3, and 4 are binominal. Variable nos. 2 and 3 are continuous. The model statistics: χ2=33.167, p<0.000.
p<0.05.
Discussion
This study showed a prevalence of chronic postoperative pain in 16.9% of the abdominal and 11.9% of the robot-assisted laparoscopic hysterectomy group with no significant difference between the types of surgery. Likewise, Brandsborg et al. 23 found no difference in the prevalence of chronic postoperative pain between different conventional hysterectomies (abdominal, vaginal, laparoscopic-assisted vaginal hysterectomy, and laparoscopic hysterectomy). Together, these two observations indicate that the type of surgical procedure for hysterectomy does not influence the development of chronic postoperative pain.
This might not be surprising, as chronic postoperative pain is assumed to be caused predominantly by nerve transection. 32 The nociceptive afferent fibers innervating the uterus follow a vast plexus of sympathetic fibers, which more or less encapsulates the uterus. 33 Thus, removing the uterus transects multiple nerves regardless of which type of surgery is used. On the other hand, the reduced cutaneous injury provided by the robot-assisted laparoscopic hysterectomy was expected to lower the risk of developing chronic postoperative pain due to the reduced number of cutaneous nerve cuts. This is also shown when comparing minimally invasive techniques (laparoscopic) with open hernia repairs.11,34,35 However, hysterectomy presents a more massive injury of visceral structure as compared with hernia repair. This indicates that visceral damage, as compared with somatic damage, is the prominent factor for the chronic postoperative pain. This is further supported by the location of the observed chronic postoperative pain areas (Fig. 2) around the dermatomes T12-L3 and S2-4. These are the spinal segments converging somatic input with visceral nociceptive afferents from the reproductive organs 36 and representing the areas of referred pain from the reproductive organs in women. 37
Risk factors for developing chronic postoperative pain
In this study, both presence of preoperative pain and higher intensity of acute postoperative pain were found to be risk factors for developing chronic postoperative pain in agreement with other studies.23,38–40
The underlying mechanisms that can explain why preoperative pelvic pain leads to chronic postoperative pain can be due to the ongoing nociceptive input to the spinal cord before the operation, which may alter the stimulus–response relationship and give rise to increasing neuronal excitability.27,41 These ongoing nociceptive stimuli alter the central nervous system by affecting the function of second-order neurons in the dorsal horn. Thus, pelvic pain before the operation can potentially cause some degree of sensitization, and hence, it could be more likely that chronic pain will develop.27,32,42 The acute postoperative pain that potentially leads to chronic postoperative pain could most likely be caused by the same phenomenon. 26
The sensitization provoked from the bombardment of nociceptive input from a visceral organ can cause viscera–visceral and visceral–somatic cross-sensitization. 43 To further evaluate the risk factors of developing chronic postoperative pain in a woman undergoing hysterectomy, we suggest quantitative sensory tests of somatic structures before surgery. The dermatomes of interest are T12-L3 and S2-4 since the nociceptive afferents innervating the uterus, cervix, fallopian tubes, and ovaries converge with the iliohypogastic, ilioinguinal, genitofemoral, lateral femoral cutaneous, and pudendal somatic nerves. 36 Allodynia in these areas has been found to be a risk factor in the development of chronic postoperative pain after hysterectomy. 44
Postoperative outcomes between surgical procedures
It was hypothesized that there would be a difference between the robot-assisted laparoscopic hysterectomy and abdominal hysterectomy in some of the postoperative outcome parameters. The results showed a significantly longer operation time and a lower blood loss in robot-assisted laparoscopic hysterectomy compared with abdominal hysterectomy. The observed lower blood loss in robot-assisted laparoscopic hysterectomy is in accordance with several other studies demonstrating robot-assisted laparoscopic hysterectomy to be more efficient in preventing blood loss.45–47
This study demonstrated a significantly longer operation time with robot-assisted laparoscopic hysterectomy compared with abdominal hysterectomy, which is consistent with multiple other studies.45–47 However, one other study by ElSahwi et al. 48 reported the opposite and found the operation time of robot-assisted laparoscopic hysterectomy to be shorter than abdominal hysterectomy. 48 The finding of longer operation time might be due to a bigger need of prepping time in the operating room, docking time, and troubleshooting on various faulty technical aspects of the robot 49 and, in addition, the amount of training may be an important aspect.
General limitations
The average number of days from the time of surgery to the day the women received the questionnaire was 1001.8 (2.7 years). This is important to note since this time potentiates the risk of recall bias for all the questions about the time before and right after the hysterectomy. This includes questions such as preoperative pelvic pain, preoperative pain intensity, preoperative pain elsewhere (e.g., head, shoulder, or knees), and acute postoperative pain intensity. Furthermore, the women who had undergone abdominal hysterectomy were found to have a significantly older operation history by 153.28 days compared with robot-assisted laparoscopic hysterectomized women, which could make a difference in the risk of recall bias between the two groups.
All hysterectomies were performed at one hospital, which limits the validity of this study, as it should be replicated at other hospitals.
Conclusion
Surgery with either abdominal or robot-assisted laparoscopic hysterectomy was not an important factor for the incidence of development of chronic postoperative pain. The presence of preoperative pelvic pain and higher intensity of the acute postoperative pain were associated with a greater risk of developing chronic postoperative pain. Robot-assisted laparoscopic hysterectomy produced a lower blood loss and lower acute postoperative pain intensity, but it had a longer operation time compared with the abdominal hysterectomies. Even though robot-assisted laparoscopic hysterectomy minimizes the somatic trauma, it is suggested that the damage of visceral nociceptive afferents is the main contributor to the manifestation of chronic pain.
Footnotes
Acknowledgments
The authors thank Associate Professor Carsten Dahl Mørch, PhD, for his thorough counseling regarding statistics. Furthermore, they extend their gratitude to Professor Axel Forman for his keen feedback during the composition and revision stages of the article.
Disclosure Statement
No competing financial interests exist.