
Abstract
Abstract
Introduction
A
Case
A 58-year-old woman presented with a history of dull aching pain and progressive abdominal distension of 2 months' duration. There was no history of any suspicious pigmented skin lesions or surgery for any such skin lesions in her past. She did not have any menstrual cycles since the prior 9 months to presentation. On physical examination, abdominal distension was noted with no palpable mass but with demonstrable shifting dullness. The external genitalia and per speculum examination were normal. There was a vague firm mass felt through the right lateral fornix. On digital rectal examination, it was noted that there was a mass palpable in the pouch of Douglas. The laboratory findings revealed eosinophilia (18%). Her serum CA 125 was 371.8 international units [IU]/mL (0–35 IU/mL), and her serum lactate dehydrogenase was 990 IU/L (100–412 IU/L). An abdominal paracentesis was performed and the fluid cytology was positive for malignant cells. A contrast-enhanced computed tomography (CECT) of the abdomen and pelvis showed bilateral mixed density ovarian lesions with enhancing solid components and cystic areas with fat attenuation within measuring 15×12 cm in the right ovary and 5×4 cm in the left ovary with moderate ascites (Fig. 1).

Contrast enhanced computed tomography abdominal scan showing bilateral mixed density ovarian lesions (arrows) with enhancing, solid-component, cystic areas and fat-attenuating areas and ascites.
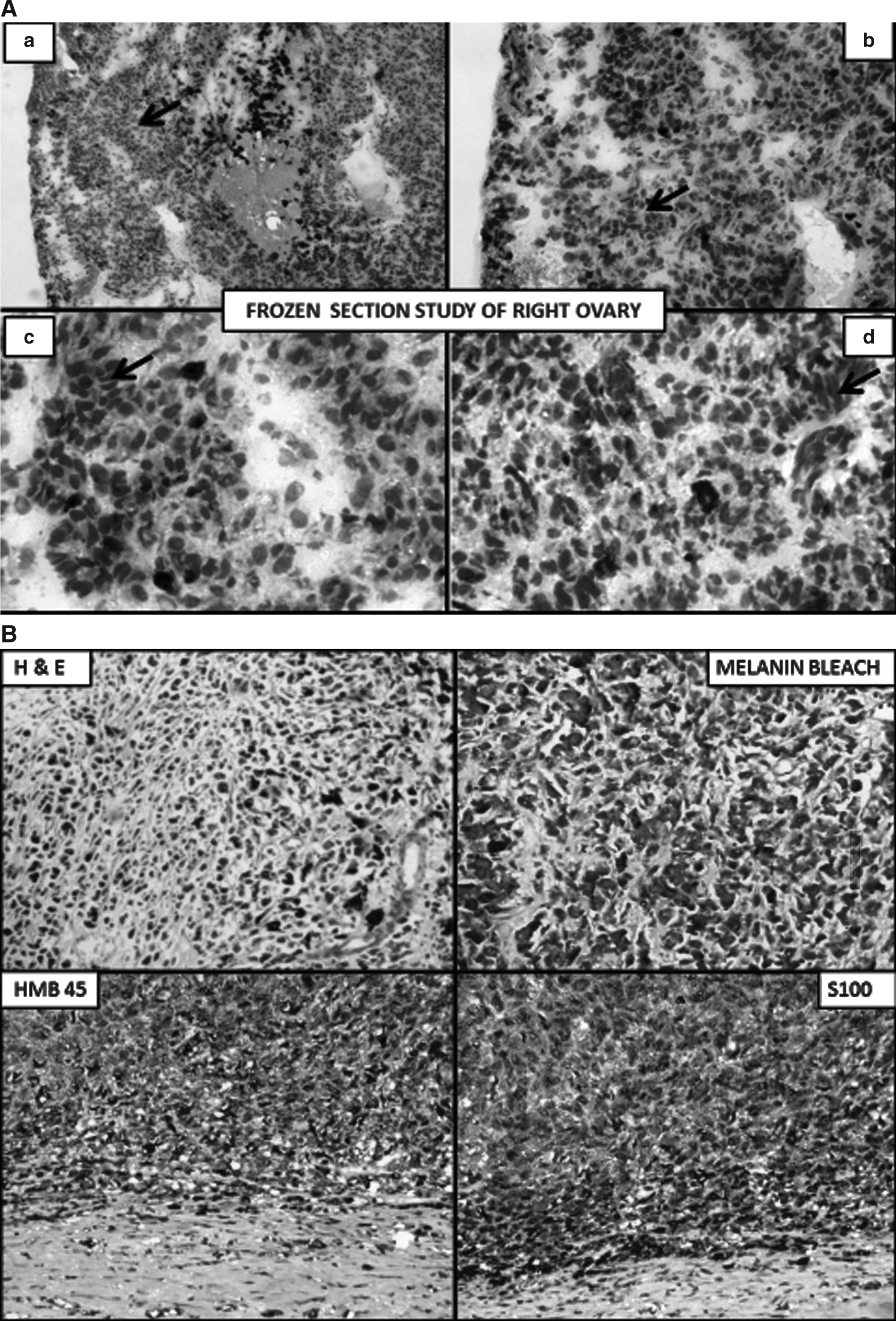
A provisional diagnosis of malignant ovarian neoplasm was made, and the patient underwent a staging laparotomy. At laparotomy, ∼ 3.5 L of serous fluid was found in the peritoneal cavity and there was a complex cystic mass of 15×12 cm in the right adnexa. The mass was adherent to the fundus of the uterus with multiple black colored surface deposits. There was another complex cyst of 5×4 cm in the left ovary and many blackish nodules of varying sizes over the parietal peritoneum, omentum, mesocolon, and mesentery of the small bowel (Figs. 2 and 3). A bilateral salpingo-opherectomy was initially performed and the excised specimens were sent for intraoperative consultation, which reported that the patient probably had a malignant melanoma of the right ovary and a benign mature cystic teratoma of the left ovary. The staging was completed by performing a total hysterectomy, bilateral pelvic and para-aortic lymph-node dissections, a total omentectomy; and many peritoneal and diaphragmatic biopsies.
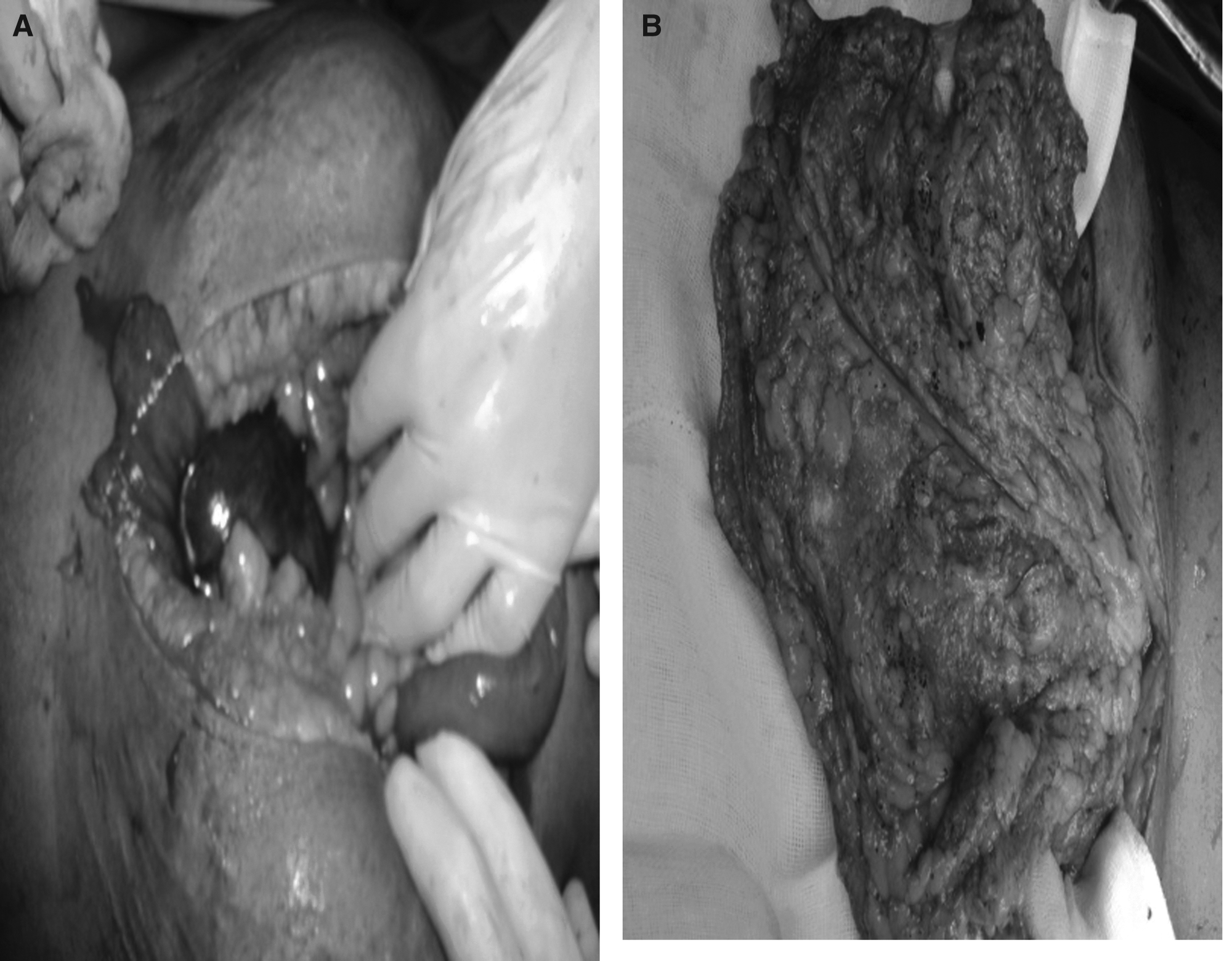

Specimen photographs of the right and left ovaries.
The final histopathologic examination of the paraffin sections from the operative specimen revealed a mature cystic teratoma of the left ovary with an area of malignant melanoma in the left ovary and metastatic involvement of the right ovary and omentum, as well as in the peritoneal biopsies obtained from the bilateral paracolic gutters and the diaphragm. The sections from the Fallopian tubes and all the 17 lymph nodes harvested were free of tumors. A confirmatory immunohistochemical evaluation was performed with HMB45 and S100, and the tumor cells showed a diffuse, strongly positive reaction (Figs. 4, 5, and 6).

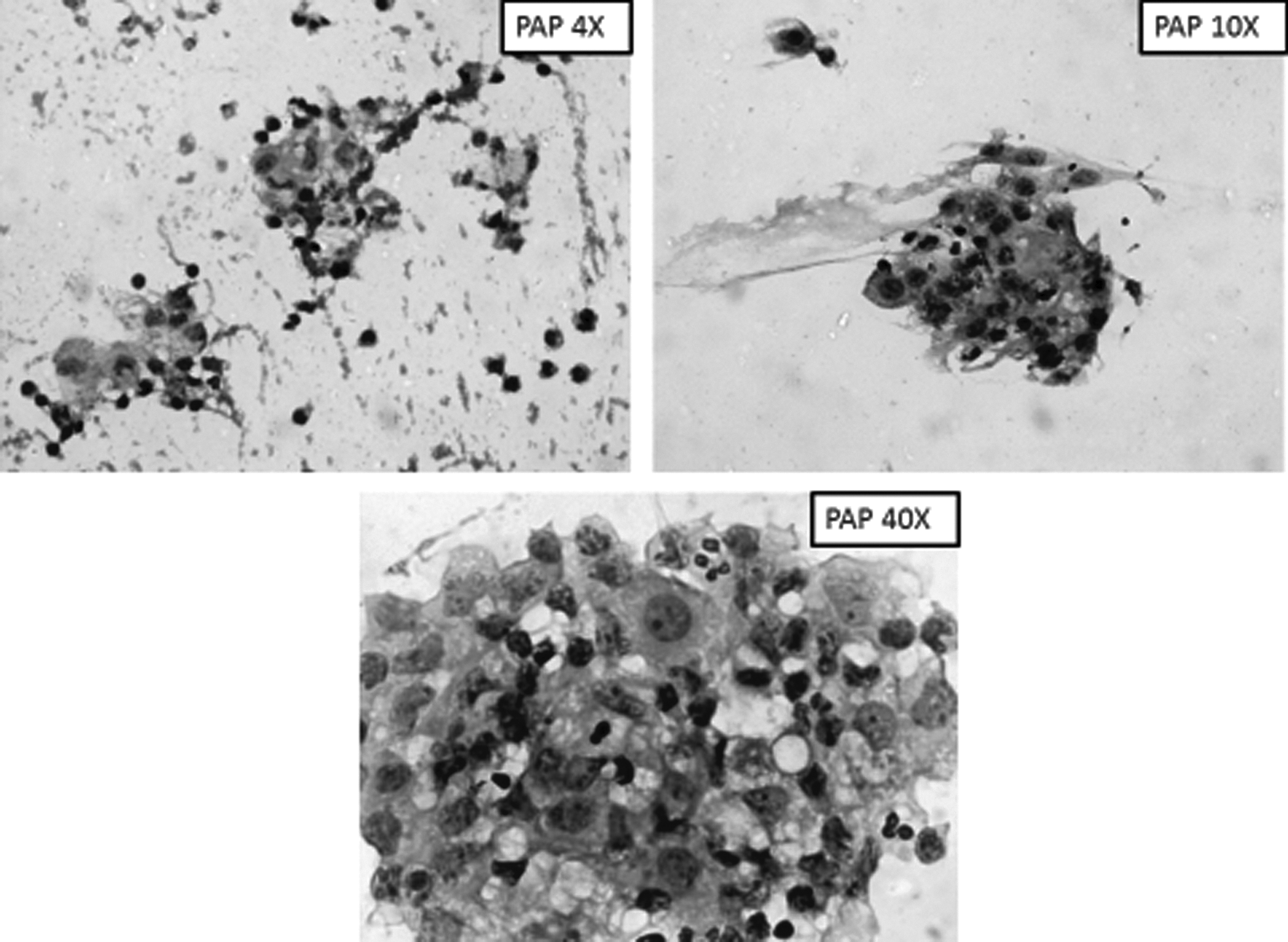
Intraoperative fluid cytology.
(1) No extraovarian site of primary melanoma
(2) Unilateral tumor with a component of teratoma
(3) Good correlation of patient's age and symptoms with those that are well-documented in the literature.
(4) Demonstration of melanocytic junctional activity (desirable but not necessary for diagnosis
Results
Following surgery, this patient was evaluated with whole-body F18 flourodeoxyglucose positron-emission tomography/computed tomography to look for any probable site of primary or other metastatic areas, and that did not reveal any other sites of disease. The patient was referred to medical oncology services of the Sri Venkateswara Institute of Medical Sciences, in Tirupathi, Chittoor District, AP, India, for further treatment. At the time of this writing, the patient had completed 2 cycles of chemotherapy with temozolomide with few side-effects.
Discussion
Melanocytes, the cells from which melanoma originates, are normally distributed in the skin (dermo–epidermal junction), meninges, choroid of the eye, mucous membranes, and upper esophagus. These cells produce melanin pigment, which is responsible for the colors of the skin and eye. Malignant melanoma most commonly arises from the skin (91.2%), followed by the eye (5.3%) and the mucous membrane (1.3%). In 2.2% of the remaining cases, the site is undeterminable.
Malignant change in a dermoid cyst itself is rare, accounting for 0.2%–2% of cases, with the commonest histology being squamous-cell carcinoma, followed by adenocarcinoma, and melanoma (which is rarest of all).
6
To date, only 46 cases have been reported in the literature, of which one report is a compilation of 20 cases.
Differentiation of primary from metastatic melanoma in the ovary is challenging for pathologists. 13 This differentiation is mostly based on the criteria proposed by Cronje and Woodruff, 14 which is provided in Box 1. In the current case, the first 3 of the 4 criteria were met, and although junctional activity was not seen, it is not mandatory for the diagnosis. 15 Junctional activity is often destroyed by tumor invasion, or the melanoma may arise from a component other than the dermo–epidermal junction. 4
Although the current authors agree that one cannot rule out a rare possibility of a regressed cutaneous primary melanoma presenting with ovarian metastasis, the positive peritoneal biopsy and fluid cytology in the presence of ovarian melanoma strongly points to ovarian origin.4,16 It has also been suggested that, if an ovarian cystic teratoma is associated with markedly elevated levels of CA-19-9, lactate dehydrogenase (LDH), and squamous-cell carcinoma–related antigen, there is a strong possibility of a malignant melanoma arising in a teratoma. 17 In the current case the patient had elevated levels of LDH and other markers were not measured. This case is probably the first case of a primary ovarian maliganant melanoma arising in a cystic teratoma with metastasis in the opposite ovary.
Owing to the bilaterality of the teratomas, another debatable point is if a melanoma arising in the teratoma of the right ovary effaced the teratomatous elements in it and spread to the left ovary and beyond. 18 In contrast to the primary site, metastatic melanoma of the ovary commonly occurs in young women (mean age: 38 years), 19 with a known primary elsewhere in each patient's body and is often bilateral with no identifiable teratomatous elements. 18
Another condition that needs to be differentiated is peritoneal melanosis, which is a benign pigmentation of the peritoneum, mesentery, surface of the ovaries, and appendix. Peritoneal melanosis can be primary or secondary. One variant of secondary peritoneal melanosis associated with an ovarian teratoma was first described by Afonsoy et al. in 1962. 20 At laparotomy, the condition may mimic primary a ovarian melanoma, but the histologically benign-appearing cells will have an absence of mitotic activity and invasive features. 21
Preoperative diagnosis of a primary ovarian melanoma is rarely possible. There is a single case reported in the literature, wherein a preoperative definitive diagnosis was made with a computed tomography scan of the patient's abdomen and pelvis.22,23 In this regard, magnetic resonance imaging is more useful, as it can detect melanin pigment in the ovary by the hyper-intense signal on T1-weighted images.
24
Standard treatment consists of surgical resection, whenever feasible. Although, there has been no proven benefit of any adjuvant treatment, in some of the cases reported earlier, the patients received chemotherapy, biologic therapy, or both,
Conclusions
Primary malignant melanoma of the ovary is difficult to diagnose without a component of teratoma. Even with teratomatous elements, this is a diagnosis that involves excluding more-common metastatic disease from a more-common cutaneous primary.
Footnotes
Disclosure Statement
None of the authors have any conflict of interest with respect to this article