
Abstract
Abstract
Introduction
B
Currently, there is a paucity of literature reviewing the caregiver burden among postoperative geriatric patients. 13 This is of particular interest to the field of urogynecology, as many of these patients are 65 or older. 14 Given increasing rates of surgical correction for pelvic-floor disorders and the impact this will have on the large number of our aging population,15,16 this study was conducted to characterize the burden of geriatric urogynecologic surgery patients on their informal caregivers. In addition, we sought to investigate specific variables related to the physical and emotional toll of providing care, as well as perceptions of both the caregiver and the patient during the postoperative period.
Materials and Methods
This was an institutional review board (IRB)–approved prospective cohort study conducted at TriHealth Good Samaritan Hospital, in Cincinnati, Ohio. Participants included female patients ages 65 or older, who were planning to undergo major urogynecologic pelvic-floor surgery, and their primary informal caregivers, who anticipated providing at least 50% of the postoperative care for these patients. For the purpose of the study, the current authors used the United States Department of Health and Human Services definition of “informal caregiver” as the unpaid person delivering the majority of care to the person considered to be ill or disabled. 12
Inclusion criteria for major urogynecologic pelvic-floor surgery included any patient who consented to vaginal hysterectomy with pelvic-floor defect repairs, vaginal pelvic-floor defect repairs without hysterectomy, robotic sacrocolpopexy with pelvic-floor defect repairs, robotic sacrocolopexy alone, or colpocleisis/colpectomy. Pelvic-floor defect repairs were considered to be two or more of the following: anterior native tissue repair; posterior native tissue repair; apical suspension; or enterocele repair.
Transvaginal mesh or graft augmentation procedures were not included as the study site does not routinely perform them. Any anti-incontinence procedure was permitted as an adjunct to the major surgeries listed above. Exclusion criteria included inability to read, write, and speak English for patient and caregiver; dementia; minor pelvic-floor surgery (i.e., outpatient procedures such as anti-incontinence surgeries); multiple informal caregivers anticipated postoperatively; or expected formal caregiving such as that in a structured nursing or rehabilitation facility after surgery.
Screening was performed in an outpatient office setting during scheduled surgical consultation visits and during the inpatient admission the morning of surgery. After informed consent was obtained from the patient and her chosen primary informal caregiver, baseline questionnaires were administered. Patient information obtained at baseline included: demographics; Short Form–12 general health survey (SF-12) 17 ; and a nonvalidated questionnaire regarding each patient's baseline functional status and level of care currently required as well as expectations for her postoperative care. Caregiver information obtained at baseline included: demographics; SF-12; assessment of current relationship to the patient and reported expectations for her care postoperatively; Zarit Burden Inventory (ZBI) 18 ; and the Caregiver Burden Index (CBI).19,20 Per the single institution's practice, routine postoperative instructions were given at the time of surgical consultation (baseline), including but not limited to: (1) no lifting>10 pounds for 6 weeks; (2) no tub baths/hot tubs/sitz baths for 6 weeks; (3) no intercourse, enemas, or vaginal/rectal suppositories for 6 weeks; and (4) personal showering, dressing, toileting, and walking (stairs included) permitted with no driving for 2 weeks.
Additional questionnaires were distributed to patients at routinely scheduled postoperative visits at 2, 6, and 12-week intervals including a 10-cm graphic rating system adapted from validated visual analogue scales (VAS) 21 for patient perception of burden on caregiver and patient perception of postoperative pain, with 10 being worst. At these timepoints, patients also completed the SF-12, general questions about perceived postoperative care, and a list of postoperative complications. At the same time intervals of 2, 6, and 12 weeks, caregivers completed the SF-12, ZBI, CBI, and nonvalidated questionnaire regarding postoperative caregiving duties. If a caregiver was unavailable in the office at any follow-up interval, the questionnaires were mailed along with a self-addressed, postage-paid return envelope, and a follow-up reminder phone call was made by the research nurse. A study stipend of $50 was given to each pair after their interval questionnaires were completed and received.
Questionnaires
General demographics included multiple-choice questions about the subject's socioeconomic background. The SF-12 is a 12-question validated survey about one's general health, assessing a mental (MCS) and physical (PCS) composite. 17 Each domain is given a weighted score, ranging from 0 to 100, with 50 considered to be comparable to the mean health of the general U.S. population, while 30 is considered to be 2 standard deviations (SDs) below the general population's health, indicating “below average” health status.
Patient Perception of Postoperative Care, Caregiver Perception of Postoperative Expectations, Patient Assessment of Postoperative Care, Postoperative Complications, and Caregiver Assessment of Postoperative Expectations were all nonvalidated forms created by the authors to query patients or caregiver sinterpretations of their relationships and expectations for care pre- and postoperatively. While edited by the investigators for IRB-approval, these nonvalidated surveys were not pilot-tested.
The ZBI is a validated 22-item multidimensional questionnaire measuring caregiver burden, with 5 subscales and all scores evaluated using a 5-point Likert scale ranging from 0 (never) to 4 (nearly always). The time to administer this survey was ∼10 minutes, with a total score ranging from 0 to 88 and a higher score (no determined cutoff value) reflecting a higher level of burden. 18 While cutoff values can be determined by the user, the authors of the ZBI have suggested that a score 0–20 indicates little or no burden, 21–40 mild-to-moderate burden, 41–60 moderate-to-severe burden, and 61–88 severe burden.
The CBI is a validated 24-item multidimensional questionnaire measuring caregiver burden with 5 subscales and all scores evaluated using a 5-point Likert scale ranging from 0 (not at all disruptive) to 4 (very disruptive). Time to administer the survey was ∼10 minutes, with a total score>36 indicating caregiver “burden.” 19,20
Given that a higher score on the ZBI and CBI indicates a higher degree of burden, and that previous literature has shown the incidence of depression in caregivers to be high, the current authors planned to refer any subject with a higher score (ZBI=41–88; CBI>36) immediately to his or her primary care physician for further depression screening and possible intervention.
Statistical analysis
As this was a preliminary descriptive study, a sample size of 50 patients and their informal caregivers was deemed to be appropriate. Statistical analysis with means, medians, and binomial proportions were used to illustrate the characteristics of the patient group and the caregiver group. For comparisons of scores between groups and within groups, Student's t-test, χ2, Fisher's exact tests, and repeated measures analysis of variance were applied. In addition, Omnibus and Tukey's Honestly Significant Difference (HSD) were applied post-hoc for correlations between demographics and questionnaires. All appropriate measures were taken to ensure the confidentiality of study participants. Their information was de-identified and reviewed in a secure area. Statistical analysis was conducted using SPSS©, Version 19, Chicago, IL. Funding was provided by an educational grant from the TriHealth Good Samaritan Medical Education Fund, Cincinnati, OH.
Results
Fifty-two patients and their caregivers consented to participate (Fig. 1). After enrollment and baseline preoperative data was obtained, 4 persons withdrew. Thus 48 pairs completed the study and the follow up questionnaires.

Enrollment log.
Baseline characteristics of pairs
At baseline, there was a significant difference in mean age, 72.8 (SD 5.3) patient versus 62.8 (SD 13.3) caregiver (p<0 .0001); gender (patients all female versus 19 female caregivers; p<0.0001); marital status (13 patients widowed versus 1 caregiver widowed; p=0.001); and income<$33,500 (23 versus 11; p=0.016; Table 1). In addition, there was a significant difference in the baseline SF-12 PCS score, with caregivers reporting better overall health, 49.57 (SD 1.48) versus 44.98 (SD 1.74; p=0.001; Table 1). Nonetheless, the only significant difference in self-reported medical comorbidities was urinary incontinence (18 patients versus 2 caregivers; p<0.001; data not shown).
SD, standard deviation; BMI, body mass index; NS, nonsignificant; SF-12, Short-Form 12; PCS, physical composite score for SF-12; MCS, mental composite score for SF-12.
Caregiver characteristics
In general, the majority of caregivers were white (96.6%), male (65.5%), nonsmokers (51.7%), with a reported annual income of>$33,500 (Table 1). Twenty-six spouses (54.2%), 18 children (37.5%), 1 parent (2.1%), 1 sibling (2.1%), 1 grandchild (2.1%), and 1 friend (2.1%) reported being caregivers during the postoperative period. While 61.5% of caregivers had lived with the patients before surgery, only 31.3% of patients still considered their caregivers' schedules in timing their procedure (data not shown).
Surgery and expectations for caregiving
At enrollment, most patients had Stage III pelvic organ prolapse (57.1%) and stress urinary incontinence (44.4%), and then underwent total vaginal hysterectomy with pelvic-floor repairs (16/51; 31.4%) or vaginal pelvic-floor repairs alone (15/51; 29.4%). All patients (100%) expected their primary informal caregivers to assist them postoperatively with at least 3 of the following: bathing; transportation; household chores; dressing/clothing; wound care; cooking; dispensing medications; toileting; and walking/ambulating. Ninety-four percent (47/51) felt that their providers counseled them fully on the postoperative recovery course and 74.5% (38/51) expected to stay 1 night in the hospital. Interestingly, 3.9% felt their total recovery would take 2 weeks or less, 7.8% stated 2–4 weeks, 70.6% stated 4–6 weeks, and 15.7% anticipated a recovery lasting more than 6 weeks. At surgery, 93.9% of patients lived in their own homes or apartments and reported having more than 3 steps between levels (47.9%).
Postoperatively at 2 weeks, only 4.2% (2/51) of patients reported having an indwelling transurethral catheter, although 45.8% (22/51) complained of “voiding dysfunction,” specifically urinary urgency and frequency (22.9%) and/or stress incontinence (10.4%). Other self-reported issues were vaginal bleeding/discharge (72.9%), nausea/emesis (14.6%), and fecal incontinence (8.3%). There were no major surgical complications reported (i.e., bowel injury, bladder perforation, hemorrhage/hematoma, pneumonia, venous thromboembolism, ileus or bowel obstruction, or fistula formation).
The majority of patients stayed 1–2 nights after surgery (93.8%), with the remainder (6.2%) staying 3 nights for pain management. Overall, 2.1% (1/51) was evaluated in the emergency room post hospital discharge for a nonsurgical issue that was managed medically and 4.2% (2/51) were reevaluated for issues related to their surgery, but not readmitted. Finally, at 2 weeks, 87.5% (42/51) felt that the information provided before surgery helped prepare them adequately for postoperative recovery, and 97.9% (46/51) felt that their recovery was improved by having informal caregivers.
Questionnaires
Regarding questionnaires, SF-12 PCS scores decreased in patients from 44.98 (1.74) at baseline to 31.47 (1.22; p=0.0001) at 2 weeks, and 38.12 (1.46; p=0.002) at 6 weeks following surgery, with a return to baseline at 12 weeks (45.92 [1.66]; p<0.0001; Fig. 2). Although there was improvement by 12 weeks, the total PCS score remained below the mean for the general U.S. population (<50), suggesting that, while the bothersome symptoms of prolapse may have resolved with surgery, patient overall health did not improve. SF-12 MCS scores were significantly improved for patients at 6 weeks (53.16 [1.21] to 57.32 [1.28]; p=0.013), with a slight trend back to baseline at 12 weeks (55.13 [1.20]; p=0.006).

Patient questionnaires.
For caregivers, SF-12 PCS scores remained virtually unchanged aside from one minor significant decrease in PCS score from 2 to 6 weeks (49.57 [1.68] to 47.6 [1.74]; p=0.017; Fig. 3) Interestingly, SF-12 MCS scores improved significantly from baseline to 6 weeks (p=0.029) with a slight trend back to baseline by 12-weeks (p=0.004). Mean ZBI scores increased from baseline to 2 weeks (7.15 [1.01] to 9.09 [1.09]; p=0.002), suggesting a greater burden on caregivers at that time. Similarly, mean CBI scores worsened from 4.66 (0.76) to 8.74 (0.78) at 2 weeks (p=0.0001). Both ZBI and CBI had slight but significant decreasing trends back to baseline scores by 12 weeks for caregivers (ZBI, p=0.03; CBI, p=0.0002; Fig 3).
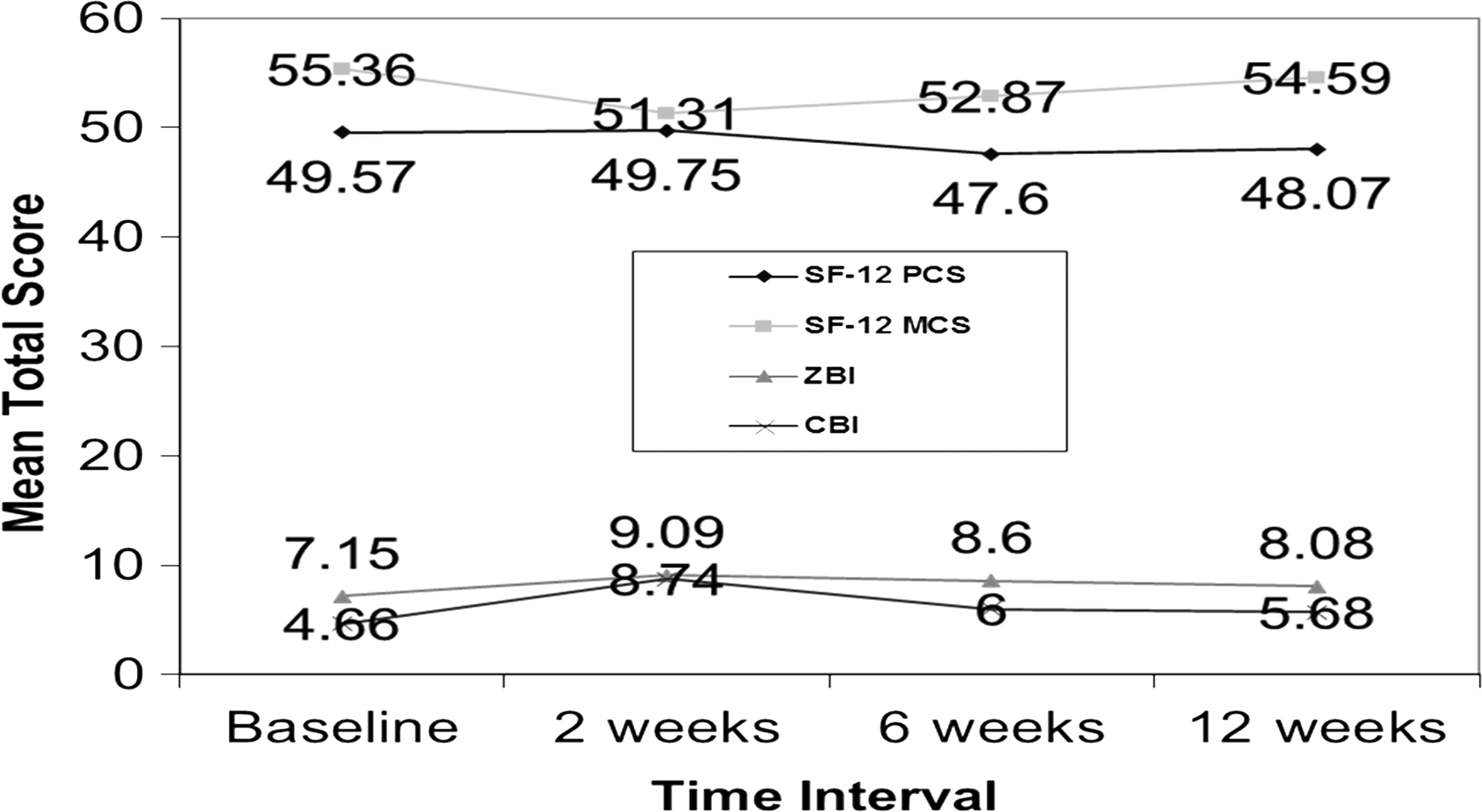
Caregiver questionnaires.
Regarding the VAS, patients' perception of burden placed on their caregivers decreased significantly over time from 2 weeks (2.83/10) to 6 weeks (2/10; p=0.01), then to 12 weeks (1.62/10; p<0.001). Similarly, patient perception of postoperative pain decreased significantly over time from 2 weeks (1.91/10) to 6 weeks (0.48/10; p=0.001), then to 12 weeks (0.05/10; p=0.001).
Secondary outcomes
Further analysis was performed to explore associations among variables. The patients' self-reported perceptions of pain (on a VAS) and sense of burden on their caregivers (on a VAS) at 2 weeks did not correlate (Spearman's correlation) with the caregivers' perceptions of being burdened, based the latter's on ZBI and CBI scores. However, there was convergent validity noted as ZBI and CBI scores changed similarly at each timepoint within the study such that they measured the same outcome consistently (Table 2).
VAS, visual analogue scale; ZBI, Zarit Burden Inventory; CBI, Caregiver Burden Inventory.
In addition, the current authors sought to evaluate if any demographic variables were associated with higher noted burden on validated indices. Among caregivers, there were no associations noted between total ZBI or CBI and demographics (i.e., age, gender, income, or marital status). While initial omnibus analysis revealed a significant association between SF-12 MCS scores at 2 weeks and relationship of caregiver to patient (p=0.05); when post hoc Tukey's HSD was applied, the difference between SF-12 MCS scores among spouse–caregivers and child–caregivers was no longer found to be significant. Finally, although analysis of associations between caregiver burden and patient postoperative complications was planned, there were, fortunately, too few complications of surgery for evaluation.
Discussion
This study defines the level of physical and emotional burden on caregivers for geriatric urogynecologic surgical patients, using validated indices. Specifically, caregivers reported increased burden at 2 weeks postoperatively, with a return to baseline by 6 weeks that was sustained at 12 weeks. This was related to in each case to patient's diminishing physical health after surgery; as each patient's physical health temporarily worsened the caregiver's sense of being burdened increased. In addition, the current authors determined concomitant trends in patients' postoperative pain, patients' perception of burden placed on caregivers, and caregivers' sense of being burdened. Although no significant correlation was noted, patients' pain and perception of placing burden on caregives increased in a similar manner to the caregivers' sense of being burdened in the immediate postoperative period.
Other studies have shown that the act of caregiving may result in caregivers perceiving their own health status as being poor. 22 One reason for this is the association between a patient's declining health status and the increasing burden upon the caregiver. In addition, the number of hours of care and intensity of care provided has correlated with severity of depression. 23 The current study failed to describe a similar correlation possibly because of the shorter duration of burden.
The current authors also did not note associations among validated questionnaires and demographics—such as gender, income, marital status, or relationship to patient—which differs from other literature describing the burden on caregivers being greatest when the primary caregiver is a spouse, is a smoker, older, resides with the care recipient, or has a lower reported income, or when the patient herself is hospitalized instead of being an outpatient.2,4,22–24 However, the vast majority of caregivers in the current study were spouses residing with the patients. Although caregivers affected by a higher subjective burden may be more likely to ask for help, up to one-third of caregivers feel “trapped by their roles,” while 40% do not feel supported by health and social services.11,25 In the current study, the subjects were not queried if they “asked for help” in their informal caregiving roles. Nonetheless, the study did show that patients reported the sense of burden they imposed on their caregivers at 2 weeks correlated positively with the caregivers' perceptions of being burdened.
To date, most studies examining caregiver burden focus on patients with chronic illnesses, such as dementia, blindness, substance abuse, and cancer.2,4,22–24 As there are well-established findings in these populations, the current authors excluded patients who were diagnosed with dementia and their caregivers, although the current authors this group might have had a higher caregiver burden at baseline, resulting in potentially more significant changes in burden inventory scores over time.
In contrast, the current study was focused on the acute care of surgical patients in the immediate postoperative period rather than patients with chronic illnesses. A Canadian study, performed during the same time as the current study and recently published, reported on a cohort of patients ages≥65 who underwent surgery and the burden that placed on their informal caregivers. 13 While the outcomes measures were similar (ZBI) to the current study, the Canadian population differed from the current study by including patients of all genders undergoing only ambulatory procedures. Nonetheless, although the current study sample was underwent inpatient major urogynecologic surgery, the current authors had similar findings of temporarily increased postoperative caregiver burden related to patient function.
Furthermore, those prior studies on caregiver burden implemented specific counseling protocols as a method of decreasing anticipated burden. For example, a study from the University of Wisconsin illustrated that psychoeducational interventions can decrease the stress among spouse caregivers of disabled persons, 26 while Casado et al. reported that interventions among Korean caregivers of geriatric persons may be more effective if they “include approaches specifically designed to build family support and improve family agreement.” 5 In contrast, the current study design did not include implementation of protocols for burden reduction; thus, the current authors were unable to evaluate any intervention outcomes. Nevertheless, despite extensive prior research in this area, there is “little evidence for the effectiveness of current interventions.”27
The strengths of this descriptive cohort study include a prospective evaluation of both patients and their caregivers, using validated well-established indices for general health and burden. In addition, many timepoints were examined from baseline to the final postoperative visit to assess for trends. Although several surveys were used at several timepoints, there was a low attrition rate. Limitations include a homogenous study population with regard to demographics and socioeconomic backgrounds. The current authors focused on data collected from one institution and the current study results may not be generalizable to all urogynecologic surgical populations or to other surgical subspecialties. While no correlations were notable between patient perception of burden and caregiver perception of being burdened, the sample sizes may not have been large enough to detect a difference. Finally, patients and caregivers were not queried about what interventions could be implemented to counteract their physical and emotional burdens—information that may have been useful.
Conclusions
Caregivers should be counseled about the anticipated burdens they might experience in the short term while caring for postoperative urogynecologic patients and be assured that these burdens are likely to resolve during the 12-week postoperative period. The current authors recommend that physicians include caregivers in the surgical consultation visit for patients, provide written and verbal instructions on expectations for postoperative care, and encourage informal caregivers to ask for help. The ability to identify issues in this population as well as characterizing patients that may be higher risk of imposing higher caregiver burdens will enable physicians to provide practical counseling and access to further resources to support caregives who are in greater need.
Footnotes
Acknowledgments
The authors extend thanks to Jennifer Mills, MD MSc, a family medicine resident, at Bethesda North Hospital, in Cincinnati, OH for data collection and entry; Justin Gregg, MA, a senior research outcomes administrator, at the Hatton Institute for Research and Education of the Good Samaritan Hospital, Cincinnati, OH for data analysis; and Angela Fellner, PhD, an academic clinical research supervisor, at the Hatton Institute for Research and Education, of Good Samaritan Hospital, for data analysis. These individuals report no financial disclosures.
In addition, the authors participated in the following aspects of the research process: Drs. Oakley and Pauls worked on protocol/project development, data collection and analysis, and manuscript writing and editing. Drs. Crisp, Estanol, Westermann, Ghodsi, and Kleeman worked on protocol, data collection, and manuscript editing
Disclosure Statement
None of the authors listed have any relevant financial disclosure to make with respect to this article.