
Abstract
Abstract
Introduction
I
It is important to recognize these lesions, as they may be an important cause of severe dysmenorrhea or pelvic pain that is refractory to oral contraceptive pills and/or nonsteroidal anti-inflammatory medications in young female patients.
5
The following diagnostic criteria have been suggested for accessory uterine cavity
2
:
(1) An isolated accessory cavitated mass, usually located under the round ligament (2) Normal uterus, Fallopian tubes, and ovaries (3) A surgical case with an excised mass and pathologic examination (4) An accessory cavity lined by endometrial epithelium with glands and stroma (5) Chocolate-brown colored fluid contents (6) No adenomyosis in the uterus, although there may be adenomyosis in the myometrium of the accessory cavity because of increased intracystic pressure.
Although case reports of these lesions have been published, there has yet to be a report of pregnancy in an accessory uterine cavity. This article presents a case of an ectopic pregnancy in an accessory uterine cavity; this was successfully treated with methotrexate and excision of the accessory cavity.
Case
A 32-year-old, gravida 4, para 1, married Caucasian female initially presented to her gynecologist complaining of a 4-year history of cyclical lower abdominal pain. She was prescribed oral contraceptive pills; however, her pain did not resolve. Transvaginal ultrasound was performed, which showed an isoechoic, partially cystic lesion in the right uterine fundus. She subsequently underwent a diagnostic laparoscopy, which showed an ∼3-cm cystic bulge in the right uterine fundus directly below the round ligament insertion. This lesion was aspirated and found to contain blood. The uterus, Fallopian tubes, and ovaries otherwise appeared normal.
This patient then had a hysterosalpingogram that showed a normal uterine cavity and patent Fallopian tubes. She was then referred for consultation. Given the imaging results and presence of hemorrhagic contents of the cavity, she was diagnosed with a noncommunicating accessory uterine cavity. She was offered surgical management; however, as she was asymptomatic at that time, she chose to proceed with expectant management.
After her initial presentation, this patient became pregnant and had a missed abortion at ∼6 weeks estimated gestational age. A dilatation and curettage was performed, and karyotyping of the products of conception showed trisomy 13. She subsequently had a chemical pregnancy and an endocrinology work-up was performed. This patient was found to have hypothyroidism and was started on thyroid replacement. She began clomid for ovulation induction. She achieved pregnancy and delivered a live female infant at term via spontaneous vaginal delivery.
Approximately 18 months later, the patient presented to the emergency department with pelvic pain. She was found to have a ß–human chorionic gonadotropin (ß-hCG) level of 52,397 mIU/mL. Ultrasound testing at that time showed a fetal pole and a small yolk sac, but no fetal heartbeat was identified. She was diagnosed with a spontaneous abortion, and a dilatation and curettage was performed. Pathology testing, however, showed decidualized tissue but no chorionic villi were identified. She was referred again for consultation. A repeat ultrasound was performed in the office, and the products of this conception were noted to be located in the accessory uterine cavity (Fig. 1). The patient was treated with methotrexate (50 mg/m2) and her ß-hCG levels were followed until the level dropped to <1 mIU/mL. Follow-up ultrasound testing showed retained debris in the accessory uterine cavity, measuring 6×4.6×6 cm. A decision was then made to proceed with excision of the accessory cavity. The patient had magnetic resonance imaging (MRI) performed prior to this surgery; the MRI which showed a 4.5×3.6×3.5 cm lesion in the right fundus of the uterus (Fig. 2).

Ultrasound showing the accessory uterine cavity with pregnancy.
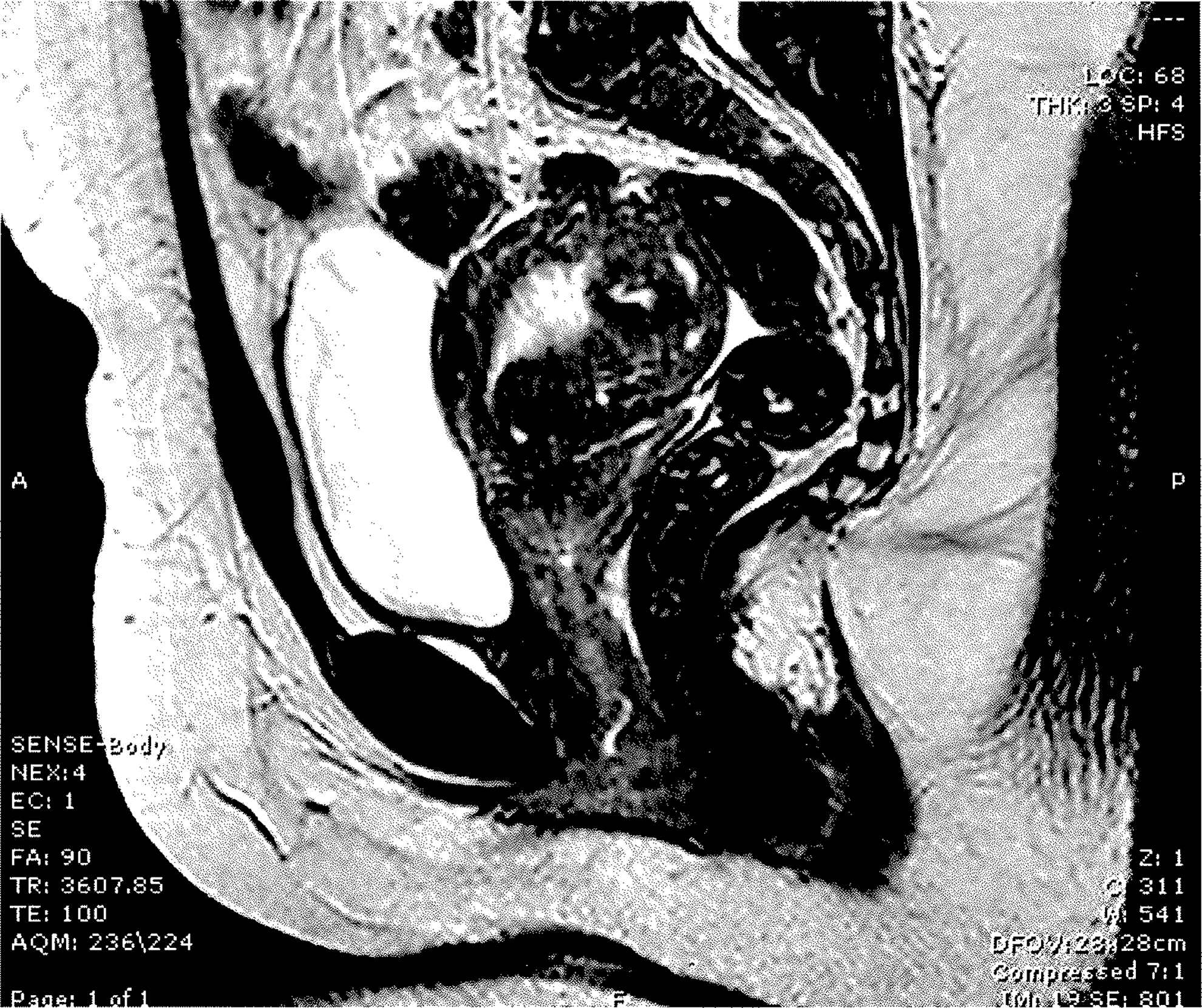
Magnetic resonance imaging of the pelvis showing the accessory uterine cavity separated from the normal endometrium.
Surgical intervention
The patient underwent an examination under anesthesia, laparotomy, and excision of the accessory uterine cavity. An ∼4×3 cm cystic lesion was noted under the musculature at the right uterine cornua. This area was injected with dilute pitressin, and a 3-cm incision was made using a Bovie. The accessory uterine cavity was then dissected from the myometrium, using blunt and sharp dissection (Figs. 3 and 4).

Surgery for removal of accessory uterine cavity.

Accessory uterine cavity.
Microscopic description of excised materials
Sections of the excised material showed a myometrial cavity partially lined by endometrium. Within the center of the cavity, were many immature chorionic villi embedded in blood clots. The villi were predominately necrotic. The smooth-muscle wall had a moderate amount of acute and chronic inflammation, including scattered plasma cells. Chorionic villi were implanted in the muscular wall with little intervening stroma (Fig 5). The endometrial glands appeared to be inactive, being composed of evenly spaced glands without secretions or visible mitoses. The endometrial stroma was mildly spindled and had a moderate amount of acute and chronic inflammation (Fig. 6). Obvious decidualization was not present (Figs. 3 and 4).
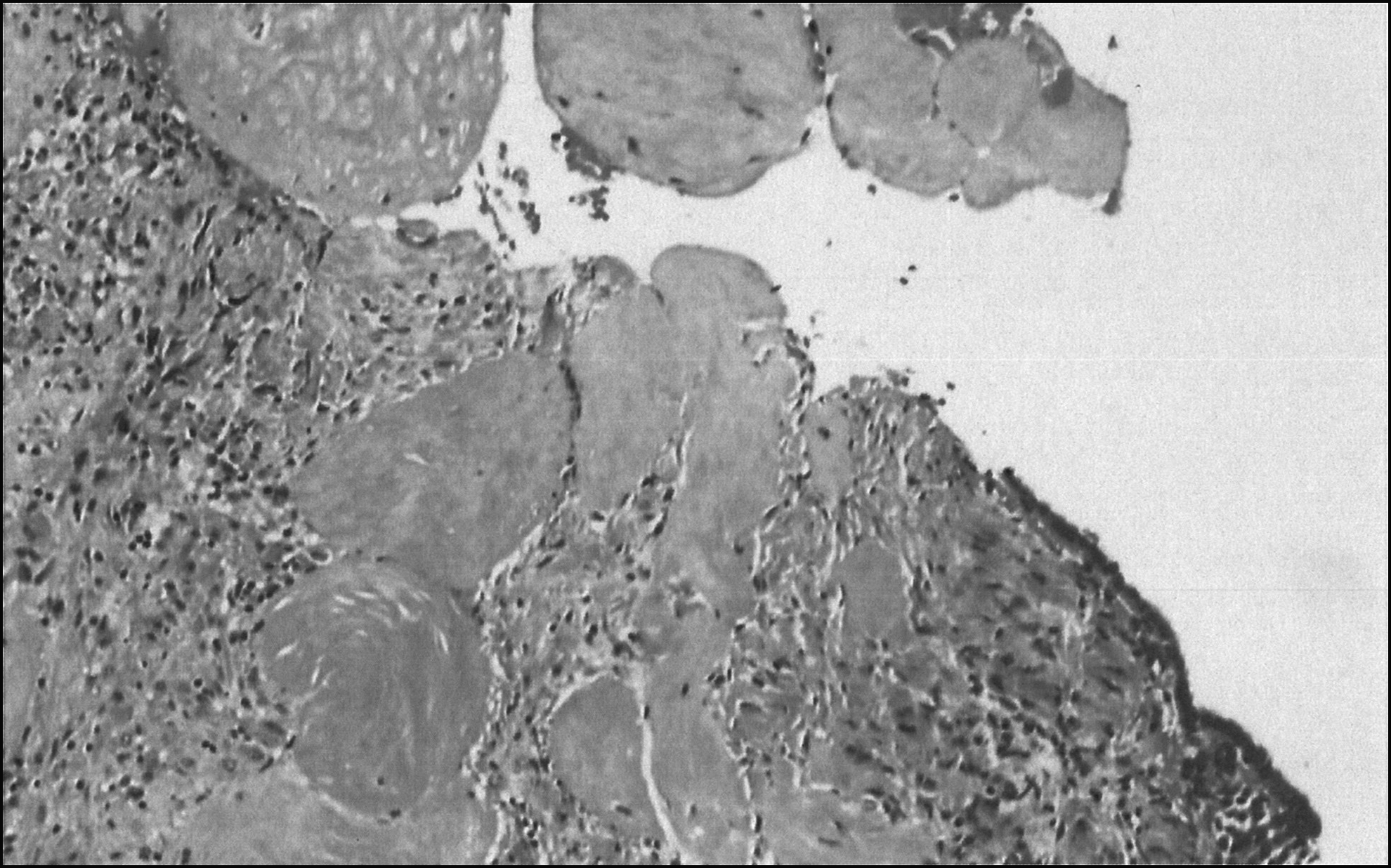
Chorionic villi, representing pregnancy inside the accessory uterine cavity.
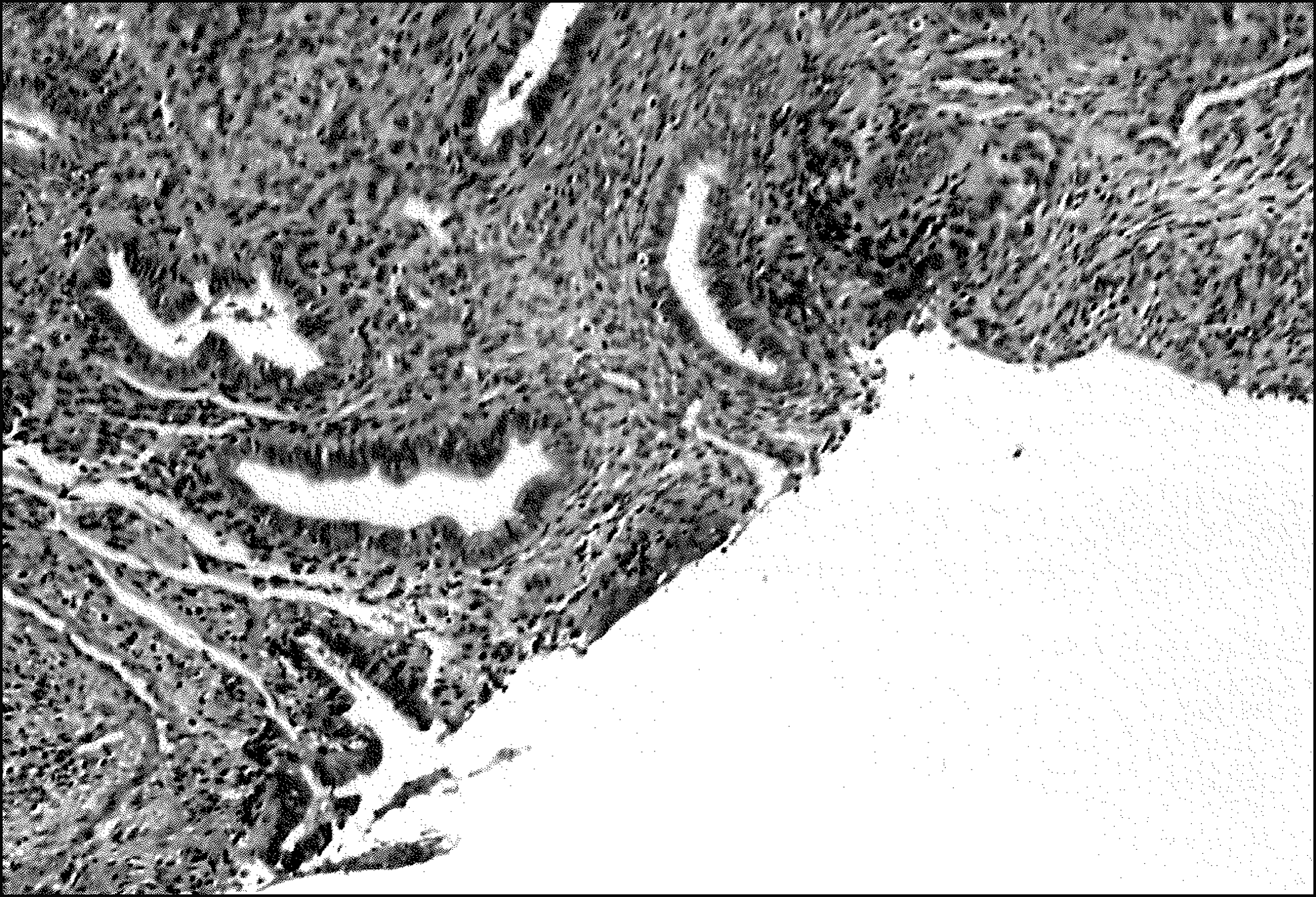
Endometrial lining of the accessory uterine cavity.
Results
Postoperatively, this patient's course was uncomplicated, and she was discharged to go home on postoperative day 1.
Discussion
The uterus, Fallopian tubes, cervix, and upper vagina are formed by the fusion of the paramesonephric ducts by the 22nd week of gestation. 6 Abnormalities in the formation or fusion of these ducts result in various uterine anomalies that occur in 1:200 to 1:600 females. There are currently seven classes of Müllerian anomalies that are recognized by the American Society of Reproductive Medicine: (1) uterovaginal hypoplasia and agenesis; (2) unicornuate uterus; (3) uterus didelphys; (4) bicornuate uterus; (5) septate uterus; (6) arcuate uterus; and (7) uterine anomalies related to diethylstilbestrol exposure. 7 Recent literature, however, supports the addition of a new category of Müllerian anomaly: an accessory uterine cavity. Accessory uterine cavities are noncommunicating uterine masses, lined with functional endometrium and surrounded by myometrial tissue, located within the myometrial wall of the uterus. It is hypothesized that these lesions form from a duplication error in a segment of the paramesonephric ducts during invagination of the coelomic epithelium of the urogenital ridge. As these masses are typically located below the insertion of the round ligament, they may be related to gubernaculum dysfunction. 8
Accessory uterine cavities are a rare pathologies, typically found in young women who present with severe dysmenorrhea or chronic pelvic pain. On transvaginal ultrasound, an isoechoic-to-cystic appearing mass can be seen at the uterine fundus, just below the insertion of the round ligament. MRI can also confirm the presence of a cavitated mass with hemorrhagic contents. 2
It is also important to rule out other pathologies, including other Müllerian anomalies or cystic adenomyosis. In order to evaluate for other Müllerian anomalies, a hysterosalpingogram should be performed to confirm a normal uterine cavity with patent Fallopian tubes. MRI will confirm a normal uterine shape. Cystic adenomyosis typically occurs in older, perimenopausal patients. 3 They typically have diffuse adenomyosis lesions with small, usually <5-mm, cysts. These lesions have different histopathology, as they lack an endometrial lining with myometrial muscle fibers. On MRI, accessory uterine cavities have hyperintense T2 signals consistent with functional endometrium; this is not seen in cystic adenomyotic lesions.
Conclusions
Although imaging suggests that accessory uterine cavities do not communicate with the normal endometrial cavity, the presence of a pregnancy within the accessory cavity in the current case suggests that microscopic connections may, in fact, exist between the two cavities. It is important to recognize these lesions so that they can be excised to relieve chronic pelvic pain as well as preventing rare complications such as ectopic pregnancy in this accessory uterine cavity.
Footnotes
Disclosure Statement
No competing financial conflicts exist.