
Abstract
Abstract
Introduction
A
With more laparoscopic hysterectomies being performed for increasingly large uteri, prediction of surgical outcomes is becoming more important. There is a paucity of information regarding preoperative predictors of surgical outcomes in the large uterus that could be helpful in perioperative planning.
One such preoperative predictor of uterine size is the ultrasound three-dimensional measurement of the uterus with estimation of uterine volume. Ultrasonographic estimation of uterine volume is derived from the prolate ellipsoid formula (4/3π× L/2×W/2×D/2; wherein L=length, W=width, and D=depth) developed by Kung and Chang in 19966 and confirmed by other researchers.3,7
Later studies correlated postoperative uterine volume with adverse surgical outcomes.5,8 However, there are currently no studies that correlate preoperative ultrasound measurement of uterine mass directly with surgical outcomes in total laparoscopic hysterectomy (TLH).
Materials and Methods
This study was a retrospective exploratory study analyzing surgical outcomes from type VII TLHs performed by a single surgeon for benign indications between September 5, 1996 and August 30, 2012.
Patients' data were included if the patients had preoperative ultrasound evaluation with length, width and depth documented. Patients' data were excluded if the patients had malignancy as a surgical indication (or on final pathology), incomplete data, or had concomitant surgical procedures performed (i.e., Burch procedure, transobturator tape, cholecystectomy, posterior repair, sacropexy, ureteral reanastamosis, cystotomy closure, herniorraphy).
Data collected were separated into primary and secondary covariates as well as primary and secondary outcome measures. The primary covariate was ultrasound-predicted uterine mass. Secondary covariates were age, body mass index (BMI), parity, and physician experience (on date of surgery). Primary outcome measures were operative time, estimated intraoperative blood loss, and hospital stay. Secondary outcome measures were conversion to laparotomy, need for blood transfusion, and surgical complications. A Spearman correlation was used to compare postoperative uterine mass and ultrasound-predicted uterine mass.
The prolate ellipsoid formula was used to calculate ultrasound-predicted uterine mass by converting uterine length, width, and anterior–posterior (AP) diameter to volume: ([uterine volume]=4/3×pi×L/2×W/2×AP/2). Furthermore, uterine volume was converted to mass in g using: uterine mass=50.0+0.71×(uterine volume). 6
Descriptive statistics (median, standard error [SE], minimum and maximum for continuous measures, and frequency and percentages for ordinal measures) were produced for the entire cohort and subsets of the cohort. Simple linear regression was used to study associations between continuous outcome variables (blood loss, operative time, and length of stay [LOS], but only one at a time) and ultrasonographically predicted uterine mass. For each of these continuous outcome measures, the effect of other covariates (including age, race, BMI, etc.) were explored in addition to uterine mass, using a multiple linear regression analysis. Simple logistic regression was used to study associations between dichotomous outcome measures (such as conversion to laparotomy, need for blood transfusion, and indicators of surgical complications) and ultrasonographically predicted uterine mass. For each of these dichotomous outcome measures, the effect of other covariates (such as age, race, BMI, etc.) were explored in addition to uterine mass, using a multiple logistic regression analysis.
All results were declared significant at a significance level of 5% (p<0.05). Because there were multiple outcomes, compared with ultrasonographically predicted uterine volume, the significance level was adjusted for multiple comparisons. All analyses were performed using the IBM Statistical Package for the Social Science, version 20.0 (SPSS, Chicago, IL).
The University of Louisville's institutional review board acknowledged that the study was Non-Human Subjects Research according to the “Common Rule” on April 17, 2012 as the study was an analysis of a prior produced databank.
Results
Of 1458 patients undergoing laparoscopic hysterectomy over 15.4 years (9/18/1996 to 1/26/2012), 1004 patients were included in the data set for analysis. Data for patients undergoing oncologic procedures (158), with a pre- or postoperative diagnosis of cancer (185), undergoing concomitant procedures (98), and missing data points (13) were excluded (Fig. 1). The most frequent indications for laparoscopic hysterectomy were leiomyoma (32.3%), pelvic mass (23.3%), and pelvic pain (11.1%). The remaining 33.4% were performed for other benign indications (Table 1).
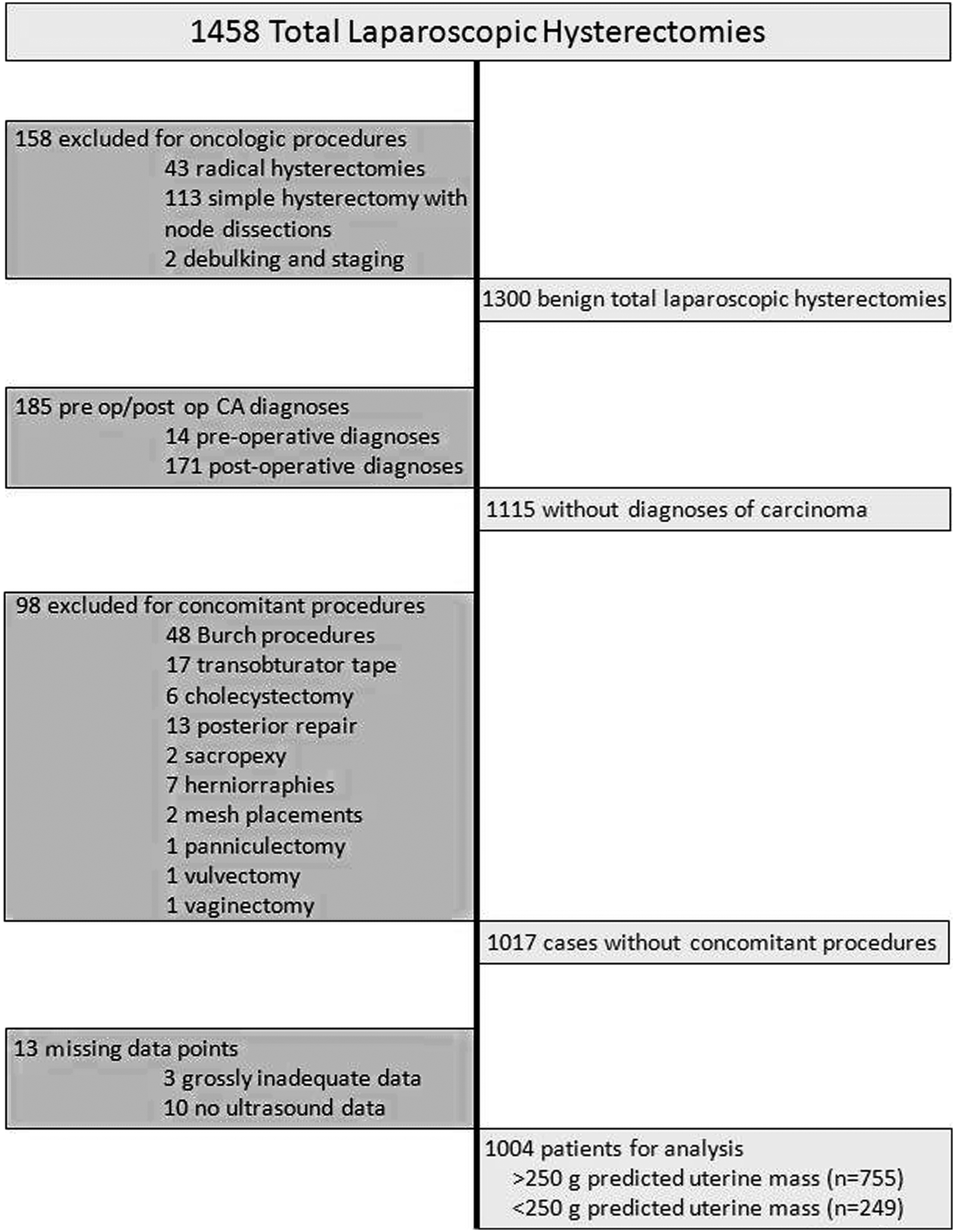
Study flow chart. After cases were excluded for oncologic diagnoses, concomitant procedures, and missing data, 1004 of 1458 cases remained in the analysis.
The patients' median age was 48 years (range: 15–90) and median BMI was 26.0 kg/m2 (range: 16.3–70.5). More than half (57.3%) of the cases had a BMI>25. Median parity was 1 (range: 0–9), with 41.6% of patients being nulliparous. The median ultrasonographically predicted uterine mass was 135 g. Stratified by uterine mass, 2 groups were established for comparison: (1) 755 (75.2%) had predicted uterine mass <250 g (median: 113.0 g; range: 55.5–249.8 g); and (2) 249 (24.8%) had predicted mass >250 g (median: 429.6 g; range: 252.9–2306.2 g). Both groups had similar demographic profiles (Table 2).
BMI, body mass index.
Median skin-to-skin operative time was 105 minutes (range: 26–355). Smaller uteri (mass <250 g) required 97 minutes (range: 26–355), and larger uteri (>250 g) required 141 minutes (range: 48–273; p<0.05; Table 2, Fig. 2). Estimated blood loss (EBL) was higher among larger uteri, 150 mL (range: 0–2000), compared with 50 mL (range: 0–2100; p<0.05; Fig. 3). Quantified units of blood transfused failed to reach statistical significance between small and large uterine groups with similar numbers of units transfused (median: 0; ranges: 0–5 and 0–2, respectively). However, when blood transfusion was considered as a dichotomous variable, women with larger uteri were transfused more often (3.6%), compared with women who had smaller uteri (1.5%; p<0.05). LOS was 1 day (range: 0–13) in both groups and, when dichotomized to ≤1 day (16.5%) versus >1 day (17.7%) there was no difference (p=0.684). There was no difference in risk of conversion to laparotomy when stratified by predicted uterine mass (Table 3).

Correlation between ultrasound-predicted uterine mass and skin-to-skin operative time.
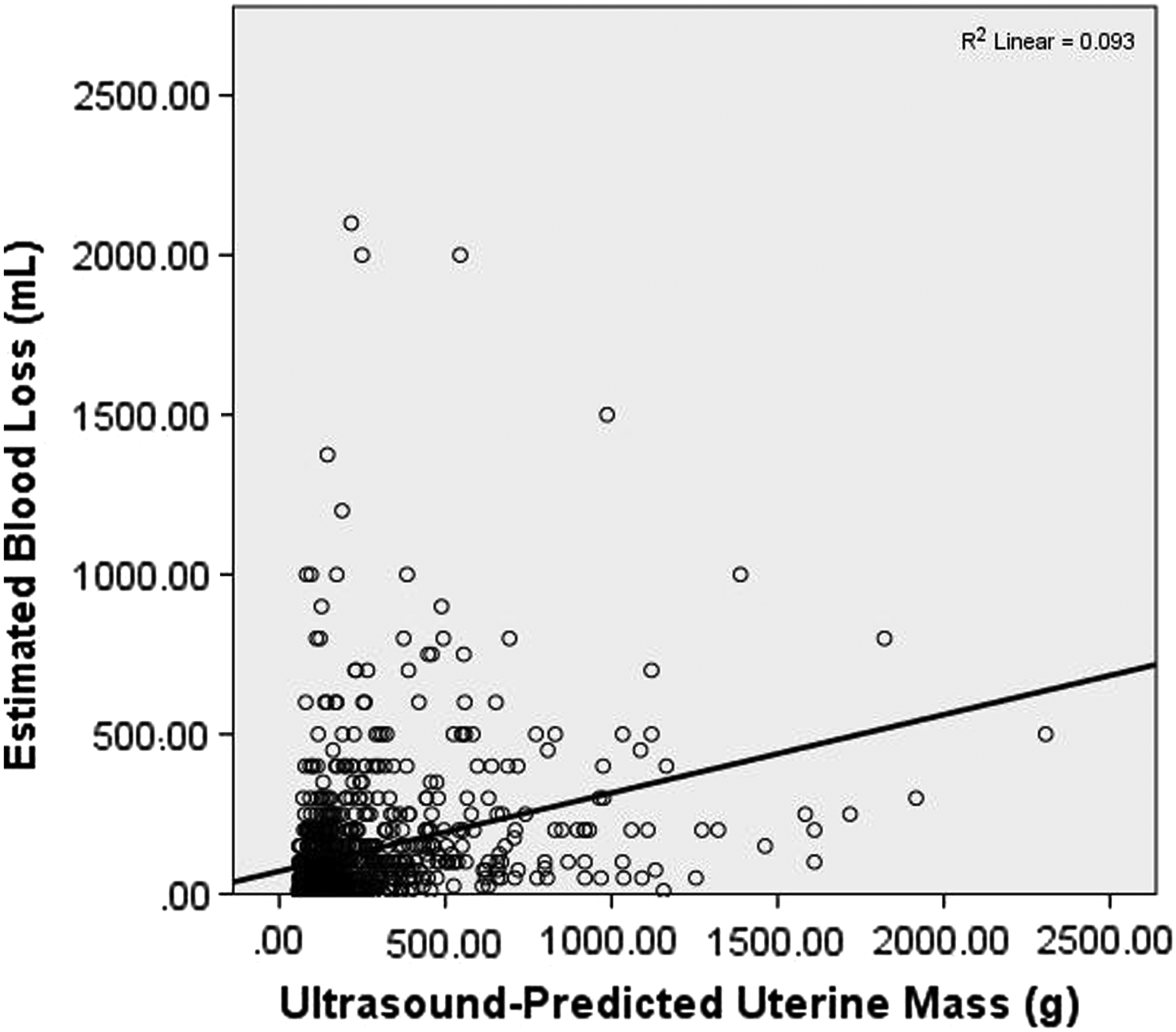
Correlation between ultrasound-predicted uterine mass and intraoperative estimated blood loss. R2=0.093.
min, minutes.
When ultrasound-predicted uterine mass was stratified by mass <250 g, 250–500 g, 500–1000 g, 1000–1500 g, and >1500 g, operative time and EBL showed a stepwise increase. Operative time increased from 97 minutes for uteri with mass <250 g to 170 minutes for uteri between 1000 and 1500 g (p<0.01). There were seven uteri >1500 g, and operative time did not sequentially increase from the prior stratification groups (100–1500 g) either as a factor of inadequate sample size or possibly a leveling off of operative difficulty. EBL sequentially increased from 50 mL in the <250-g–uteri group to 250 mL in the >1500-g–uteri group (p<0.01). The incidence of EBL>500 mL increased from 2.7% of cases to 28.6% of cases in the largest groups (Table 4).
min, minutes.
Multivariable linear regression performed for the three primary outcome variables was: (1) duration of surgery (minutes): (2) EBL (mL); and (3) LOS in the hospital (days). The regression for these three variables showed that age, BMI, physician experience in cases completed, ultrasound-predicted uterine mass, and conversion to laparotomy predicted a longer operative time (p<0.01). Parity was not shown to be correlated to operative time. EBL was directly related to ultrasound-predicted uterine mass, BMI, and conversion to laparotomy, and was inversely related to physician experience. Age and parity were not significantly correlated with blood loss. LOS was predicted by ultrasound-predicted uterine mass, physician experience, conversion to laparotomy, and protocol change from a 2-day to a 1-day postoperative hospital stay. Predictors of LOS, although statistically significant, had unstandardized coefficients of <0.01, which essentially predicted no relationships among the variables (Table 5).
SE, standard error; CI, confidence interval; BMI, body mass index.
A Spearman correlation analysis of 954 cases compared postoperative uterine mass to predicted uterine mass and found a strong coefficient of correlation (r=0.867; p<0.05). Fifty cases were excluded from the analysis because of absence of postoperative uterine mass data (Table 6).
There, were 1004 predicted uterine masses by ultrasound, but only 954 each had a postoperative measured uterine mass on the pathology report, therefore 50 cases were excluded from the analysis.
Surgical complications were reported with an overall frequency of 9.3%, with 5.4% requiring reoperation. There was a trend toward increasing operative complications associated with uterine mass (8.5%; 11.6%; p=0.135; Table 7).
=Complication that required reoperation.
Discussion
While vaginal hysterectomies are typically the first minimally invasive option, there are data that suggest some advantages to total laparoscopic hysterectomy in selected cases.9,10 Furthermore, the type VII TLH (all steps performed laparoscopically 11 ), does not depend on descensus, capacity, or laxity, unlike vaginal and laparoscopically assisted vaginal hysterectomy. This makes the procedure available for a subset of obese and nulliparous patients who may otherwise need total abdominal hysterectomy (TAH) or conversion to laparotomy from laparoscopic assisted vaginal hysterectomy or vaginal hysterectomy.
Previous work suggests that TLH for uteri of increasing size results in increasing operative time, and intraoperative blood loss. 5 These data, however, are based on postoperative uterine-mass measurements.
The current findings suggest that ultrasound prediction of uterine mass can be used to determine potential surgical outcomes in TLH, including increased skin-to-skin operative time, intraoperative EBL, and need for blood transfusion.
One of the authors (O'Hanlan) 5 of this article previously reported a correlation of increased operative time and EBL with increasing uterine size as measured postoperatively by surgical pathologists using an overlapping dataset. This current report shows that this important information can be obtained preoperatively to aid in surgical planning and patient counseling.
Knowing the difficulties associated with performing TLH on larger uteri, an attempt was made establish a model that would assist in developing guidelines for when to perform immediate surgery versus neoadjuvant shrinkage using leuprolide or other biologics. The goal was to show a specific predicted uterine mass that was associated with a definitive increase in operative time and EBL. Figures 2 and 3 show a nearest fit line to the data, indicating trends. However, with such poor fit of the lines (R2=0.093 and R2=0.128), a reliable model could not be established, likely because of the skew of the data toward smaller uteri.
Stratification of ultrasound-predicted uterine mass shows that increasing uterine size predicts longer operative times and increased EBL (Table 5). These data suggest a cutoff point of 250 g as clinically significant with regard to increase in operative time (Δ 30 minutes) and incidence of surgical blood loss >500 mL (Δ 7.1%). Because it is difficult to establish the clinical significance of a minute of operative time or an mL of blood loss, it was difficult to establish a guideline based solely on these data. Future studies should compare these outcome measures in laparoscopic hysterectomy versus TAH to examine if there is a uterine size at which referral of a patient to a more expert colleague or laparotomy would be more beneficial.
A strength of this study is that it details a large population with a broad demographic group allowing careful selection of the patient population from a large database. This dataset is representative of women undergoing hysterectomy at a mean age of 48 years (range: 15–94) with a mean BMI of 26.0 (range: 16.3–70.5). 1 Parity was widely distributed; 58.4% were parous and 41.6% were nulliparous. Indications for hysterectomy in the dataset were similar to those of the United States as a whole with fibroid growths being the most common indication. 1 These data reflect a higher incidence of pelvic mass as an indication probably because the surgeon who performed the procedures is a gynecologic oncologist. Race, ethnicity, and socioeconomic status were not examined; however, this may be helpful information for future studies, as these factors may be related to surgical outcome data.
Although this dataset was representative of the general population undergoing TLH, the surgeon performing the operations may not represent the typical gynecologic surgeon. These data are more applicable to the experienced laparoscopic surgeon as these data represent a large number of laparoscopic hysterectomies performed by a single surgeon who is an American Board of Obstetrics and Gynecology (ABOG)–certified gynecologic oncologist, and a very experienced laparoscopist with ∼1600 laparoscopic hysterectomies performed to date. Indeed this study's data did show that, after controlling for other factors, surgical experience independently predicted decreased operative time and EBL. Thereby, operative time and blood loss reported may be artificially lower than that of less-experienced laparoscopists.
Three limitations of this dataset stand out: (1) its retrospective nature; (2) the use of nonstandardized ultrasonographers; and (3) and the duration of the dataset. Because of this study's retrospective nature it was difficult to determine if all ultrasonographers measured the uteri similarly. Size-assessment techniques and observations of uterine morphology vary and improved over the 15-year study period, as had surgical skill and technology. An attempt was made to control for physician experience with multivariable regression.
There was a selection bias because operations for patients with suspected severe adhesive disease, as reflected by prior operative reports, were not attempted laparoscopically, consistent with current standard of care. To try to standardize operative time, cases with major concomitant procedures were excluded; however, minor procedures that do not typically affect operative time and blood loss (e.g., lysis of adhesions, appendectomy, uterosacral ligament suspension) were not excluded. 5 It is possible that some of these factors may have affected outcomes; however previously reported data on these procedures have not shown a significant difference. 5 These procedures, while potentially causing a significant increase in operative time and blood loss, were intentionally left in the analysis because of their frequent association with large uteri from prior myomectomy and their necessary inclusion in standard gynecologic care.
Many biases could not be avoided because of the retrospective design of the study. A prospectively controlled clinical trial using standardized reporting of ultrasound measurements would be more effective for predicting morbidity and potentially avoiding unnecessary mortality. The determination of whether hysterectomy for the large uteri is performed better laparoscopically, laparoscopically with preoperative medical debulking of fibroids, by referral to a colleague, or through laparotomy can be refined by such a study. While uterine mass predicted by ultrasound may predict overall surgical outcomes, further study may reveal that surgical difficulty increases based more specifically on the width or AP diameter of the uterus. These factors may delay or preclude access to the uterine arteries and posterior cul-de-sac, therefore affecting both operative time and blood loss.
Given that pelvic ultrasonography is commonly ordered for diagnosis of gynecologic problems and often establishes the indication for hysterectomy, there is no additional cost or patient inconvenience. Radiologists routinely provide the 3 dimensions of the uterus, measure the endometrial stripe, assess the ovarian morphology, and report the presence of free-fluid. The ability to predict surgical outcomes in laparoscopic hysterectomy based on standard ultrasound measurements may aid in patient counseling, selection of approach (vaginal, laparoscopic, open), preoperative planning (directed or autologous blood banking, obtaining assistance from more experienced surgeons, use of cell-saver), and intraoperative management (uterine artery coagulation or embolization).
Conclusions
Ultrasound-predicted uterine mass appears to effectively predict increased operative time, EBL, and incidence of blood transfusion in patients with large uteri, thereby providing important data for preoperative patient counseling and surgical planning for total laparoscopic hysterectomy.
Footnotes
Acknowledgments
The authors acknowledge the following individuals for their help with preparing the statistical information for this article: Shesh N. Rai, PhD, for statistical planning; and Kara B. Dassel, PhD, and Doug Lorenz, PhD, for statistical assistance.
Disclosure Statement
Dr. Mark W. Dassel has no conflict of interests. Dr. James M. Shwayder obtained a grant for a minimally invasive surgical fellowship from Ethicon Endosurgery, is a consultant for Philips Ultrasound, has testified as an expert witness in many trials, and is a speaker for Cook OB/GYN and Phillips Ultrasound. Dr. Katherine A. O'Hanlan is a speaker and consultant for Baxter, Covidien, CareFusion, and 3-Dmed, and is a consultant for ConMed and LSI Solutions.