
Abstract
Abstract
Introduction
C
Case Report
A 50-year-old moderately built female presented to the outpatient department of our hospital with a complaint of isolated nodule on upper back measuring 3×3 cm (Fig. 1). This nodule was growing rapidly with no history of pain. Her previous records revealed that about one and a half years ago, she was diagnosed with nonkeratinizing moderately differentiated squamous cell carcinoma of the cervix. She was staged FIGO stage IIb for which she was treated only with chemoradiotherapy for 1 year. Her subsequent period was uneventful till 2 months ago.

Photograph showing cutaneous nodular lesion on upper back.
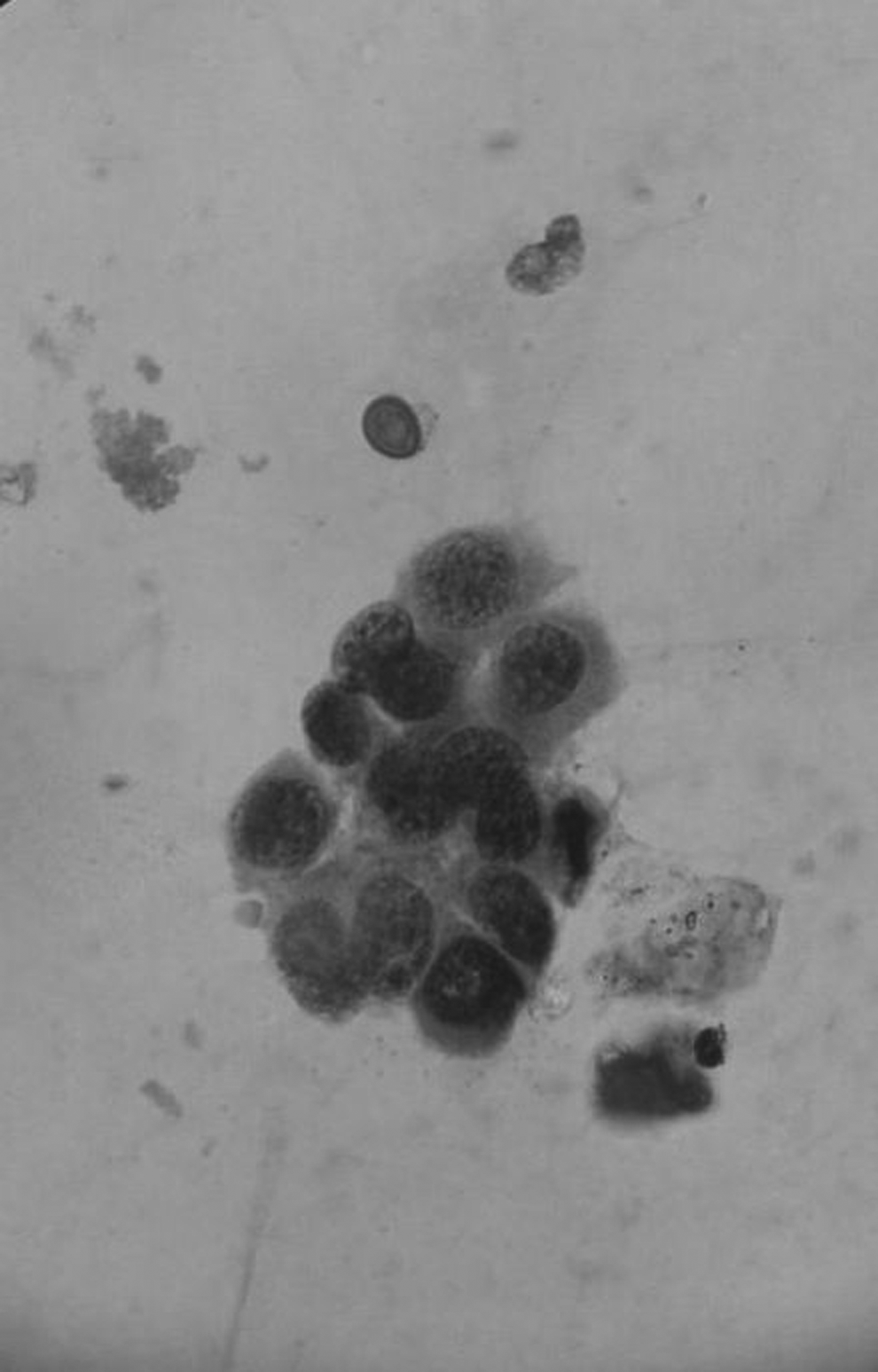
At present, no significant constitutional symptoms were observed. Her gynecological history was uneventful till now. No lymphadenopathy or hepatosplenomegaly was detected on clinical examination. Her chest X-ray and abdominal ultrasound did not reveal any nodal or extranodal spread. Her Pap smear performed 1 week ago showed radiation-induced changes with no evidence of any malignancy. With all these findings, a cytological examination by fine-needle aspiration cytology was performed for this nodule, which yielded a blood-mixed mucoid aspirate. Cytological smears prepared were stained with the Giemsa and Pap stains. These smears examined revealed clusters and singly scattered atypical squamous cells containing moderate amount of basophilic cytoplasm, hyperchromatic nucleus with irregular nuclear outline, and inconspicuous nucleoli (Figs. 2 and 3) in a background of dirty mucinous material. In view of the history of cervical cancer FIGO stage IIb, the final diagnosis of cutaneous metastasis from squamous cell carcinoma was given.

Smears showing clusters and singly scattered atypical squamous cells containing moderate amount of basophilic cytoplasm, hyperchromatic nucleus with irregular nuclear outline, and inconspicuous nucleoli in a background of dirty mucinous material (Giemsa stain, 400×).
Smears showing atypical squamous cells against a mucinous background (Pap stain, 400×).
The cutaneous nodule was excised 1 cm lateral margin free from tumor, while the deep resected margin showed some suspicious malignant cells. No other sites of metastasis were identified. Since these cases show high rate of recurrence, the patient was referred to a higher center for external beam radiotherapy and further follow-up.
Discussion
The incidence of cutaneous metastasis from visceral malignancies is 0.7%–9.0% and is most commonly seen in carcinoma arising from the breast, ovary, and colon. Cervical cancer spreading to skin is rare. The average age at which this presentation is diagnosed is 52 years. 5 The mechanism of metastasis can be seen as having three basic patterns: (1) mechanical due to anatomical proximity and lymphatic drainage, (2) site specific due to selective attachment of tumor cells to specific organs, and (3) nonselective. Metastasis to skin from visceral organs is mainly through the hematogenous route by means of vascular channels. Clinically, patients present with nodules, plaques, and inflammatory telangiectatic lesions. These may develop within 1 year to even 10 years after initial diagnosis. Imachi et al. reviewed 1,190 patients with cervical cancer, of which, 15 developed skin metastasis, and observed that the incidence of this metastasis increased in advanced stage with highest 4.8% in stage IV, 1.2% in stages III and II, and lowest 0.8% in stage I disease. 6 The incidence of skin metastasis was reported to be higher in case of adenocarcinoma or undifferentiated carcinoma than in squamous cell carcinomas. This cutaneous metastasis is regarded as a sign of terminal disease.
Cutaneous metastasis has been shown to be related to radiotherapy in some cases. 7 A proposed explanation for this is the occurrence of radiation-induced endothelial cell damage leading to tumor cell trapping. Another possible explanation is obstruction of deep lymphatics by radiation leading to increased flow through superficial lymphatics. However, radiation has not been shown to increase the spread of tumor.
No definite guidelines are available for treatment of such cases, and usually, palliative chemoradiotherapy, surgery, or a combination of both is given. Prognosis with skin metastasis is poor. Its occurrence is considered as a preterminal event with the time from diagnosis to death being 3–6 months even with palliative treatment. 5 The time interval between initial diagnosis of cervical cancer and presentation of cutaneous metastasis is important as earlier the metastasis, the worse is the prognosis.
To the best of our knowledge, this is the first case reported in India presenting as cutaneous metastasis of cervical cancer at an unusual location, that is, upper back. It represents the importance of clinical history and the role of pathologist in diagnosis of such rare lesions.
Conclusion
Suspicious cutaneous lesions especially in patients with a history of cancer should be promptly investigated as they can represent the evidence of advanced malignant disease, thereby leading to early therapeutic intervention and decreased morbidity.
Footnotes
Disclosure Statement
No financial conflicts of interest exist.