
Abstract
Abstract
Introduction
A
Objective
Comparison of the effectiveness of Asherman's syndrome therapy among patients treated by using hysteroscopic (HSK) adhesiolysis with insertion of 100% hyaluronic acid (HA) with a cohort of patients with insertion of intrauterine device (IUD) and a control cohort.
Primary outcome
Treatment of menstrual cycle disorders (recovery of regular and normal intensity menstruation).
Secondary outcome
Achieving pregnancy after spontaneous conception within one year after the end of the hormonal therapy (implantation rate [IR], take home baby rate [THBR]).
Inclusion criteria
1. Reproductive age: 28–39.
2. Presence of moderate to severe forms of intrauterine adhesions diagnosed by hysteroscopy (Stage II-III based on Asherman's syndrome classification according to the American Fertility Society), (Table 1).
3. Presence of regular menstrual cycle of normal intensity before intrauterine intervention leading to Asherman's syndrome.
4. Oligomenorrhea or amenorrhoea before the performance of HSK adhesiolysis.
5. Presence of only the uterine factor of sterility.
6. Spontaneous efforts to conception.
Exclusion criteria
1. Presence of only light forms of intrauterine adhesions (Stage I based on Asherman's syndrome classification according to the American Fertility Society).
2. Primary oligo–amenorrhea.
3. Presence of uterine myomatosis, adenomyosis, or uterine polyps.
4. Presence of other than uterine sterility factor.
5. Use of assisted reproductive methods within the efforts to conception.
Materials and Methods
Prospective clinical trial of 60 patients treated from 1997 to 2014 for Asherman's syndrome. Inclusion in the clinical trial was possible after meeting the inclusion criteria and absence of exclusion criteria. All included patients had a regular menstrual cycle of normal intensity before intrauterine intervention caused the development of Asherman's syndrome. After the intrauterine intervention, a period of oligomenorrhea to amenorrhea followed in all patients. With suspicion of Asherman's syndrome, all patients underwent hysteroscopy, and stages of intrauterine adhesions, in accordance with the American Fertility Society, were evaluated. Subsequently, all patients underwent HSK adhesiolysis using scissors and electrocoagulation loop. In 20 patients, the operation was finished with intrauterine insertion of 100% HA (Cohort A), 18 patients had a nonhormonal IUD inserted in the uterine cavity at the end of surgery (Cohort B), and in 22 cases, the operation was ended without insertion of any antiadhesion devices (Cohort C). All patients underwent a 3-month hormonal support therapy in the pattern of 2 mg estradiol being administered orally or in patches from the 1st to the 25th day of cycle and with 200 mg progesterone being added orally or vaginally from the 15th to 25th day of cycle. After the end of hormonal therapy, the recovery of a regular menstrual cycle with normal intensity (of 25–32 days' length with an intensity of bleeding similar to that before Asherman's syndrome diagnosis) was evaluated for all the patients. Also, the recovery time for return of regular menstruation cycle was evaluated. Regarding patients wishing to get pregnant again, we monitored whether spontaneous conception had been achieved within 1 year after the end of treatment as follows: IR, evaluated pregnancy results, and the frequency of abortions and childbirths; THBR, obtained data were statistically processed using Fisher's exact test (Fig. 1).
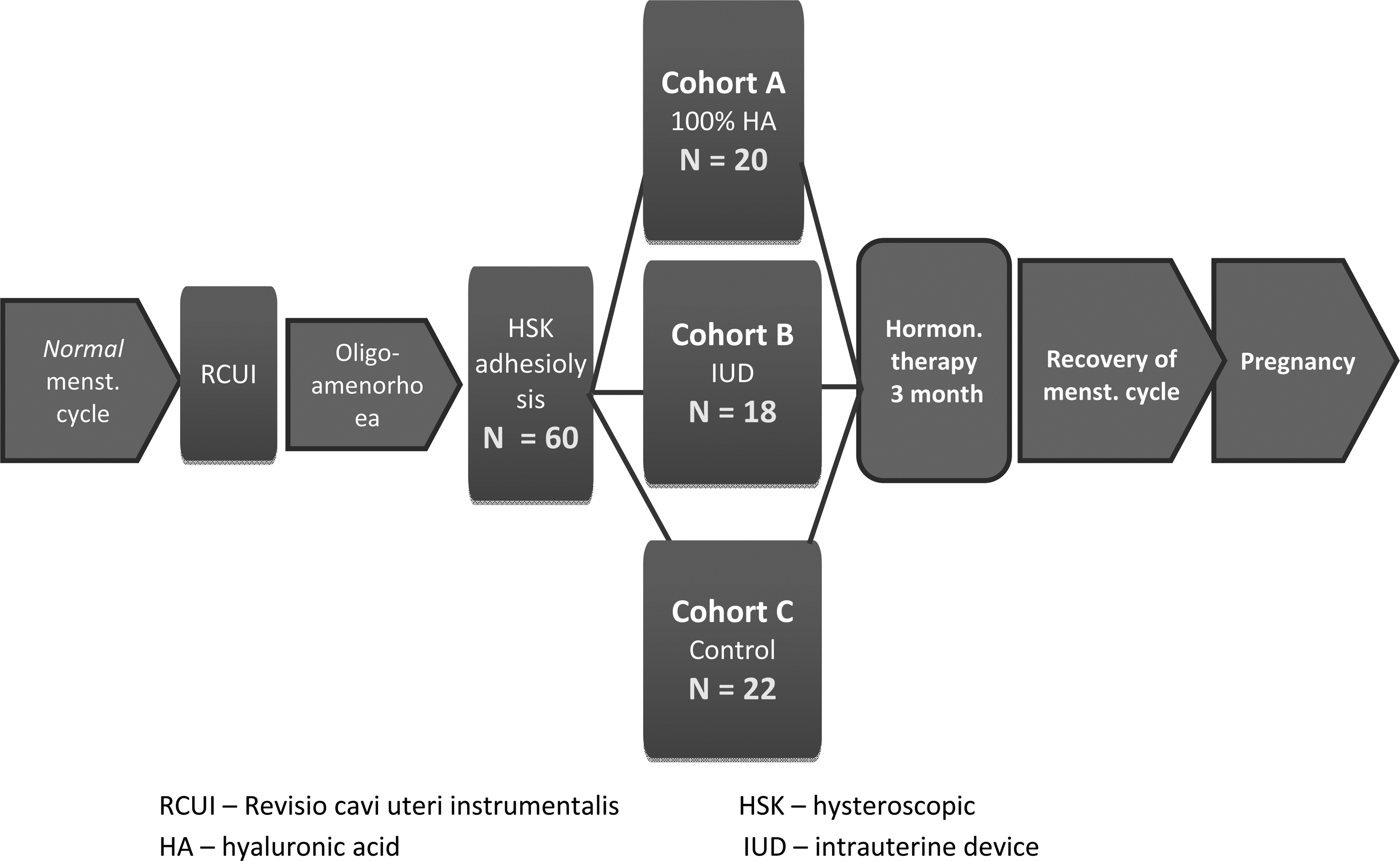
Study design.
Results
After the end of the hormonal therapy, a regular normal intensity menstrual cycle was restored in 12 out of 20 patients (60.0%) in cohort A, in 10 out of 18 patients (55.5%) in cohort B, and in 8 out of 22 patients (36.3%) in the control cohort C (Table 2). Obtained data were statistically processed with Fisher's exact test (Table 3). Given the small number of patients, there was no statistically significant difference proven in any of the followed cohorts. The regular menstrual cycle was restored in all the cohorts ∼4 weeks from the end of the hormone therapy. The efforts to achieve another pregnancy were present in 18 patients from cohort A (subgroup A1), in 10 patients from cohort B (subgroup B1), and in 14 patients from cohort C (subgroup C1). Spontaneous pregnancy within 1 year from the end of treatment was achieved by 14 out of 18 patients in subgroup A1 (IR: 77.7%), by 6 out of 10 patients in subgroup B1 (IR: 60.0%), and by 6 out of 14 patients in subgroup C1 (IR: 42.8%). In subgroup A1, three patients had a spontaneous abortion in the first trimester of pregnancy, one patient decided to get an interruption legalis (for personal reasons), and 10 patients gave birth to a healthy child (THBR: 55.5%). In subgroup B1, two patients had a spontaneous abortion in the first trimester and four patients successfully delivered (THBR: 40.0%). In subgroup C1, two patients had a spontaneous abortion and four successfully delivered (THBR: 28.5%), (Table 2). Acquired data were statistically processed using Fisher's exact test in the aforementioned way (Table 4). Given the small number of patients, there was no statistically significant difference proven in any of the followed cohorts. None of the followed patients (in all the subgroups) had an abortion in the second trimester and no congenital defect was found in their newborns.
HA, hyaluronic acid; IR, implantation rate; IUD, intrauterine device; THBR, take home baby rate.
Fisher's exact test (p-value).
A, cohort of patient with 100% HA; B, cohort of patients with IUD; C, control cohort of patients without insertion of antiadhesion agent.
Subgroup: section of cohorts that included patients with pregnancy attempts.
Fisher's exact test (p-value).
A1, subgroup of patient with 100% HA; B1, subgroup of patients with IUD; C1, subgroup of patients without insertion of antiadhesion agent.
Discussion
It is difficult to evaluate the incidence of Asherman's syndrome among the population at large—it mainly depends on the level of healthcare and a general health awareness in the society, on diagnostic possibilities, the frequency of legal or illegal abortions, the technology of performed intrauterine interventions (use of a blunt or sharp curette and suction evacuation of uterine cavity after childbirth and abortion), incidence of tuberculosis, and so on. A prevalence of 0.3% 2 was recorded in infertile patients examined by sonohysterography. Women with recurrent pregnancy losses, who were examined by hysteroscopy, have diagnosis of intrauterine adhesions (7%–21.8%). 3 Generally, we found that Asherman's syndrome at the moderate to severe stages occurs with a low incidence among the population. Due to its rare occurrence, exact guidelines are not provided in the available literature on selecting an optimal therapeutic procedure. The evaluation of effectiveness of individual therapeutic methods appears only sporadically in the literature and with ambiguous conclusions. The low prevalence of the moderate to severe forms of Asherman's syndrome was also confirmed with our clinical trial. During 16 years, we only observed 60 patients who met the inclusion criteria specified by us. The statistical processing of this small number did not register a statistically significant difference in any of the followed patient cohorts. The statistical analysis was calculated for a difference of 50% versus 25% (the approximate difference between subgroup A1 and C1, essentially the greatest difference in the entire analysis), the strength of the test was 0.8, and the limit of significance was 0.05. The difference of 25% would be statistically significant with a number of 58 patients in each cohort. The results of our clinical evaluation, given the small numbers, will have to be finally confirmed with continued clinical trial over the coming years and through involvement of other centers.
The treatment of Asherman's syndrome must be complex. Its aim is to recover the destroyed endometrium and create a physiologic state suitable for conception. The treatment consists in re-creating the spacious cavity of the uterus of a normal shape in the most effective way by means of HSK adhesiolysis. The next treatment stage consists in preventing relapse of intrauterine adhesions. An integral part of the therapy is also the estrogen–progestin therapy lasting a minimum of 3 months, which stimulates regeneration of the endometrium and re-epithelialization of traumatized surfaces.
The risk of reformation of adhesions is high (from 3.1% to 23.5%), particularly in cases of severe adhesions (20%–62%). 4 Insertion of an IUD (or intrauterine balloon) at the end of hysteroscopy surgery can be used in the prevention of intrauterine adhesions. A modern alternative is the insertion of 100% HA in the uterus. Details focusing on comparing the effectiveness of the individual methods are rarely found in literature.
One hundred percent HA
Recently, preparations containing 100% HA are very often used in antiadhesive therapy. They are natural products from an extracellular matrix and synovial fluid from joints and are mainly used as a barrier to prevent adhesions forming after abdominal and pelvic surgery. The antiadhesive effect depends on the molecular weight and concentration of the preparation. Preparations with 100% HA in the form of gel 5 are designed for use in the uterine cavity. The gel with 100% HA is highly viscous. When applied into the uterine cavity, a mechanical barrier is created, which prevents adhesion formation. It stays in place for 7 days (adhesions typically develop from third to fifth days), after which time it is completely absorbed. In the prospective randomized controlled study, 6 100% HA was inserted into the uterine cavity after completion of adhesiolysis in 43 patients with Asherman's syndrome. The presence of gel was ultrasonographically controlled, and the gel was capable of keeping the uterine walls apart for 72 hours. When second HSK was performed 3 months later, a statistically significant reduction in postsurgery intrauterine adhesions was recorded, compared to the control cohort (14.0% vs. 31.7%). 7 Our clinical evaluation confirmed the effectiveness of 100% HA insertion.
Intrauterine device
Insertion of IUD was described in many studies as an effective and frequently used method to prevent renewed formation of adhesions. The IUD in the uterine cavity keeps bloody surfaces apart in the initial phase of healing and is intended to reduce the amount of newly formed adhesions. In the last two decades, the use of different types of IUD was described in several studies. 8
Forty-eight women with secondary amenorrhea included in a prospective observation study 9 were treated by inserting an IUD with copper. Altogether, 40 women had normal periods in several weeks following the IUD insertion. The copper contained in the device caused an aseptic inflammatory reaction and stimulated the endometrium by releasing many types of prostaglandins. The effectiveness of devices without a copper content, in terms of preventing intrauterine adhesions, depends on their shape. The IUD loop referred to as the best choice to prevent adhesions has, unfortunately, not been available on the Czech market for some time now. 10 IUD insertion effectiveness in the prevention of intrauterine adhesions was also confirmed by a coherent retrospective study from 2013, where IUD insertion leads, compared with the control cohort, to a significantly higher reduction of intrauterine adhesions at a significance level of p<0.001. 11 This study, however, does not deal with effects on reproduction. IUD insertion entails a small risk of uterine perforation and higher incidence of inflammatory complications.
Conclusion
Primary outcome
The insertion of 100% HA into the uterine cavity after the disruption of moderate to severe intrauterine adhesions enabled recovery of a normal regular menstrual cycle in 60.0% of patients, compared to the cohort of patients who had insertion of IUD (55.5%) and with the control cohort with no antiadhesive agent inserted (36.3%).
Secondary outcome
The insertion of 100% HA into the uterine cavity also improved the IR (77.7%) and THBR (55.5%), compared to the cohort of patients who had insertion of IUD (IR: 60.0%; THBR: 40.0%) and with the control cohort with no antiadhesive agent inserted (IR: 42.8%; THBR: 28.5%).
Given the small number of the included patients, there was no statistically significant difference identified in any of the followed cohorts after completion of statistical analysis.
Footnotes
Disclosure Statement
No competing financial interests exist.