
Abstract
Abstract
Introduction
A
Case
A 50-year-old female presented clinically with abdominal pain and fullness. On examination, the abdominal lump was palpable. This patient had undergone a hysterectomy a few years prior in another primary institute, but there were no previous histopathologic reports. Radiologic findings revealed solid, well-circumscribed masses involving both ovaries and measuring 7×6 cm. The masses extended up to the obturator foramen, and there were pelvic nodules.
Intraoperatively, the masses were seen involving both ovaries and obturator foramen with pelvic peritoneal implants. Total resection of the masses, including oopherectomy, was performed, and samples were sent for histopathologic examination.
Grossly the left and right ovarian masses measured 7 cm and 6 cm, respectively, and were solid in consistency. A cut surface was a solid greyish-white. The obturator foramen mass measured 5 cm and had the same gross features as the ovarian masss. Representative sections were taken from tumor tissue.
On microscopic examination, a well-circumscribed tumor composed of uniform cells showing heterologous differentiation and having scanty cytoplasm, uniform nuclei, minimal atypia, and few mitotic figures. The stromal cells were bipolar and were arranged in nests and a trabecular pattern, showing sex-cord differentiation. Features showing nest and sex-cord differentiation blended with intervening stromal cells (Fig. 1) in the background with extensive hyalinization at various places (Fig. 2).
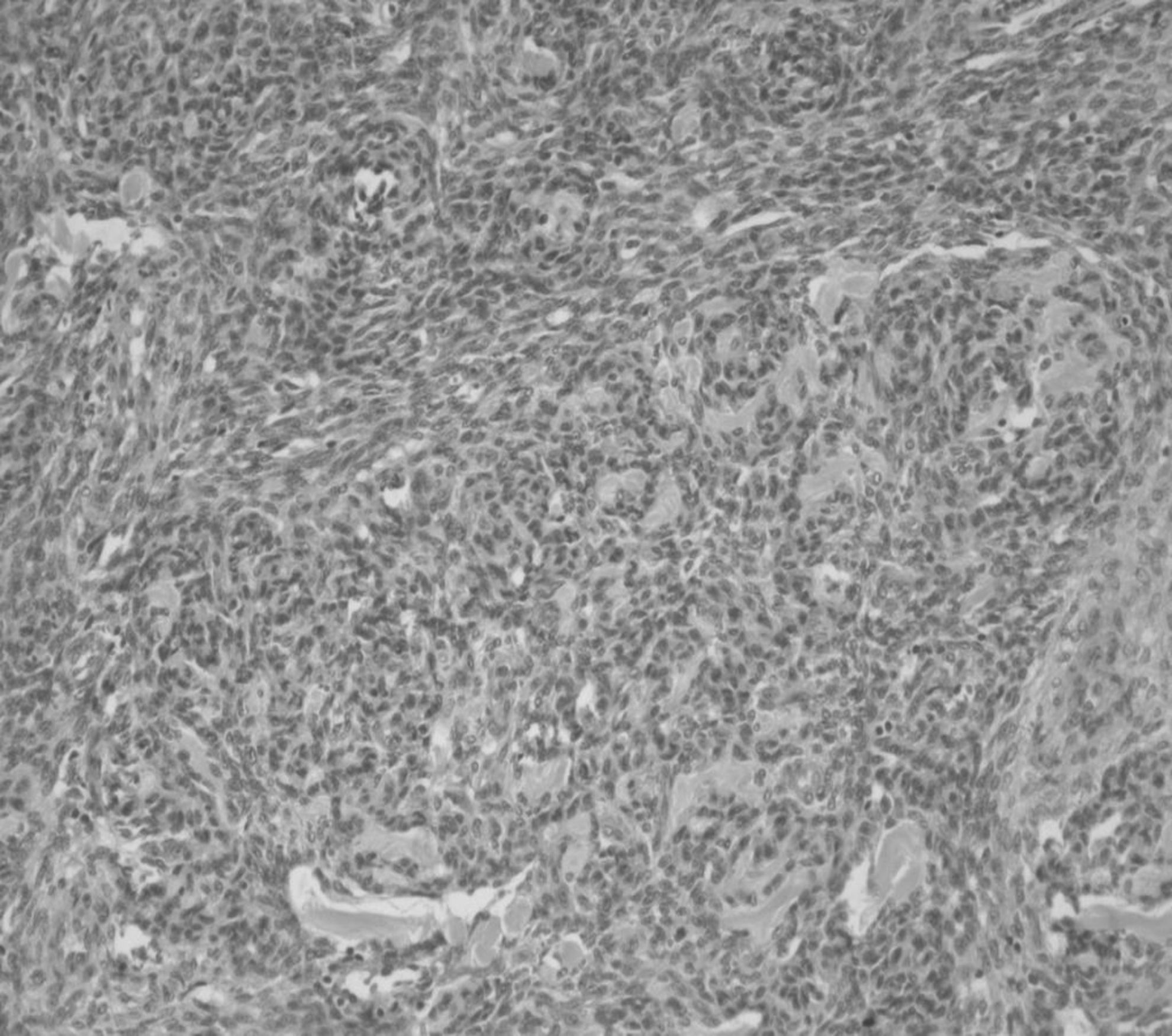
Hematoxylin and eosin stain–100× showed nest and sex-cord–like differentiation with intervening stromal cells (151×134 mm).
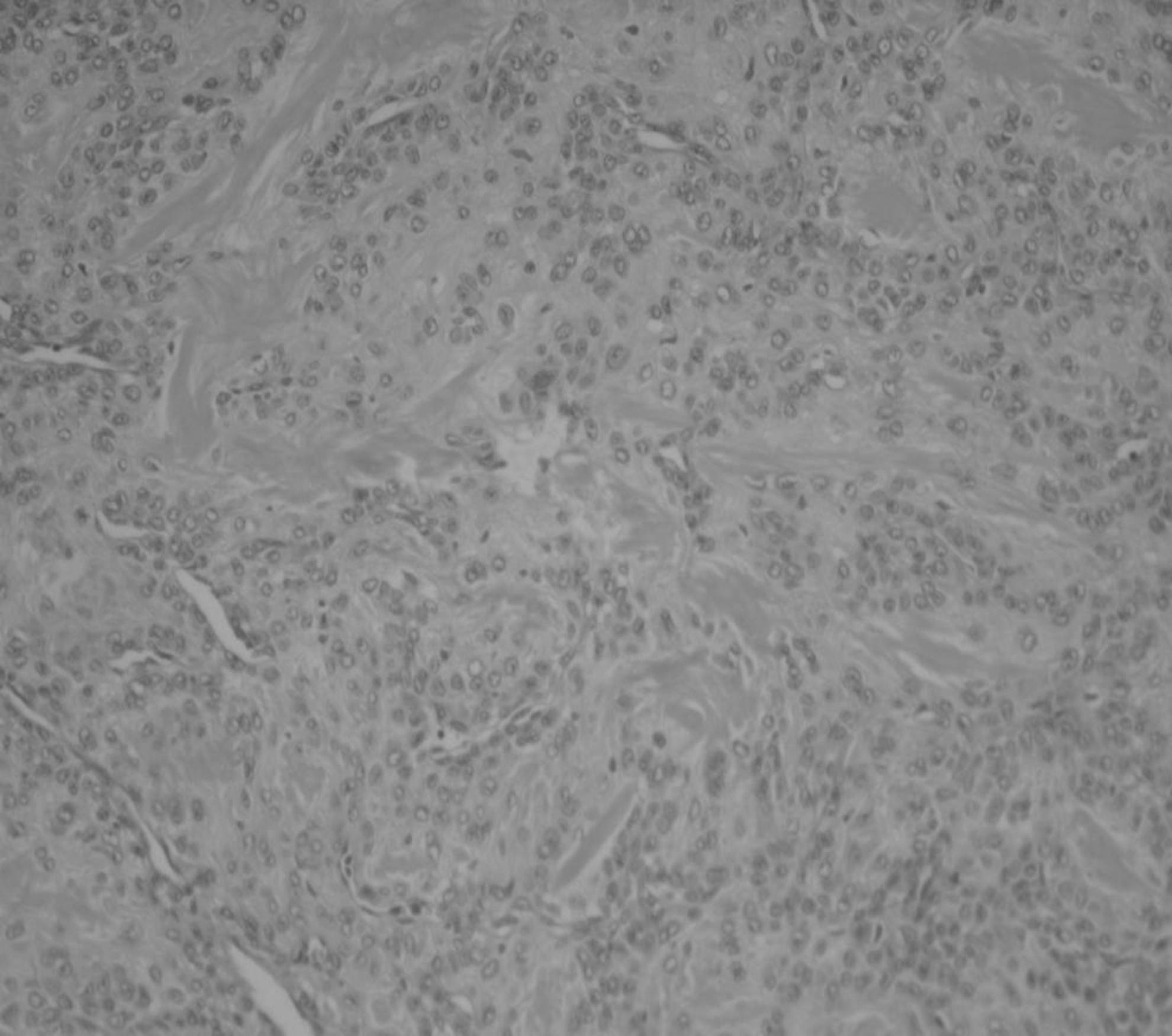
Hematoxylin and eosin stain–100× showed areas of hyalinization within the stroma (151×134 mm).
The neoplastic cells were immunoreactive to cluster of differentiation (CD10; Fig. 3) and progesterone receptor (PgR), and were negative for h-Caldesmon, cytokeratin, endomysial antibodies (EMA), calretinin, inhibin, MelanA, CD34 protein, and S-100 protein. The sex-cord elements expressed desmin (Fig. 4) and smooth-muscle antibodies (SMA) but were negative for h-Caldesmon. Thus, the diagnosis was low-grade endometrial stromal sarcoma with sex-cord–like differentiation.
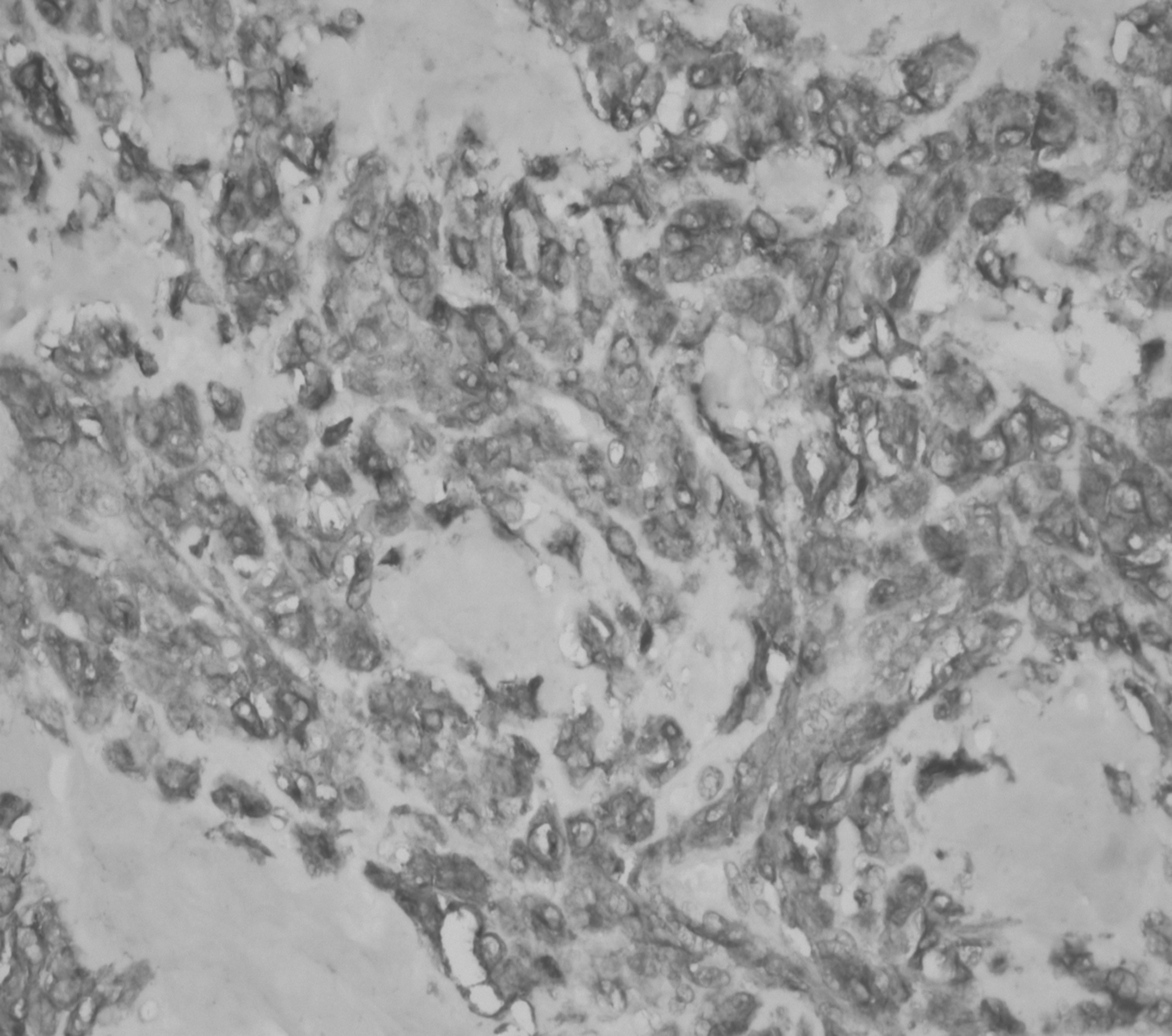
Neoplastic cells were immunoreactive for CD10 (shown at 400×).
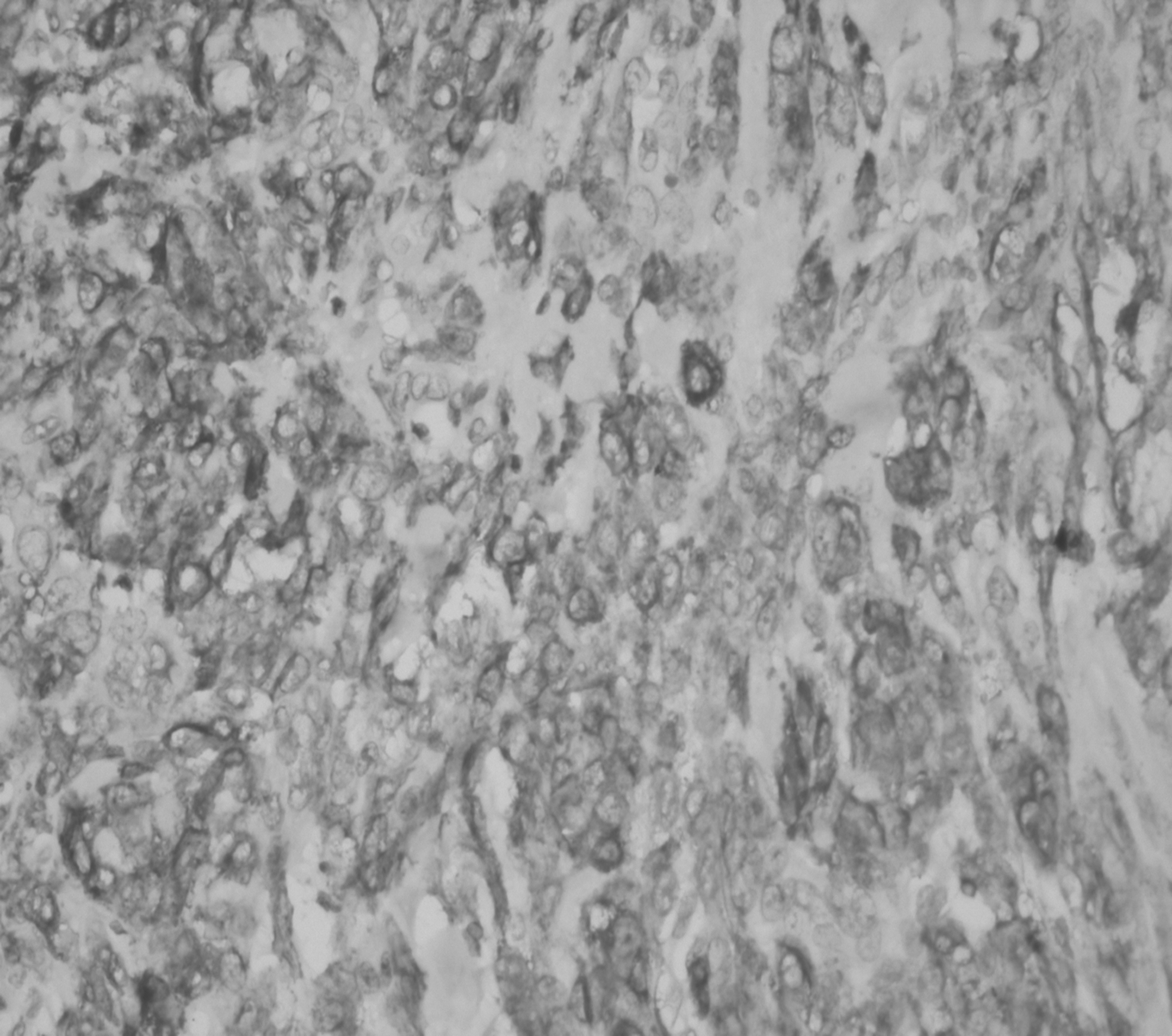
The sex-cord–like elements expressed immunoreactivity for desmin (400×).
Results
Patient was well on regular follow up and after surgical correction.
Discussion
Endometrial stromal sarcoma is a very rare sarcoma accounting for ∼0.2% of uterine malignancies. This scarcoma was initially divided into low-grade and high-grade classifications on the basis of mitotic count. Current World Health Organization classification includes distinction of low-grade endometrial stromal sarcoma and undifferentiated endometrial sarcoma—not on the basis of mitotic count but on nuclear pleomorphism and necrosis. 4 Endometrial stromal sarcoma tends to occur in premenopausal women. Histologically, this is a low-grade tumor, but its relatively good prognosis is worsened by a high potential for local recurrence and possible metastasis. 2
Endometrial sarcomas usually show metastatic potential at various sites, such as the ovaries, and the abdominal and pelvic peritoneum, but it has been observed that the ovary is the most common transformation site in females with endometriosis. 5 The current case was exceptionally rare, as this patient had no endometriotic focus or any history of hormone replacement therapy. Thus, sparing of the uterine wall and the spread directly to the ovarian tissue confirms the metastatic potential of these sarcomas. Endometrial sarcomas presenting as metastatic deposits at sites such as the ovary and abdominal peritoneum are a great diagnostic challenge to differentiate these masses from gastro-intestinal stromal tumors and leiomyosarcomas. 6
The pathologic features described in the current case were similar to those of previous reports including an infiltrative or diffuse proliferation of uniform round or oval stromal cells. The presence of foam cells also been described. Other forms of differentiation, such as smooth-muscle and epithelial patterns, include endometrioid-type glands and sex-cord–like differentiation.7–9 In the current case, the masses contained sex-cord–like elements that were often arranged in nests; cords; or trabeculae, solid, or tubular arrangements. 1
Conclusions
CD10 is currently regarded as a special marker for endometrial stromal tumors and is also expressed in normal stromal cells. Calretinin, inhibin, CD99, and MelanA seem to be most characteristic for sex-cord markers and usually express calretinin. 10 However, in the current case, all markers for sex-cord elements Calretinin, inhibin, CD99, and MelanA were negative. The differential diagnosis included epithelioid leiomyoma and epithelial neoplasm. These tumors were ruled out because the samples had CD10 positivity. Because desmin was expressed in sex-cord elements, the diagnosis of an endometrial stromal sarcoma with sex-cord–like differentiation was retained. Given that endometrial stromal sarcoma frequently express estrogen receptors and PgR, treatment with hormonal therapies may be efficacious for patients with advanced, residual, and recurrent cases. 3
Footnotes
Disclosure Statement
No financial conflicts exist.