
Abstract
Abstract
Introduction
H
Historically, the uterus has been removed by either the abdominal or vaginal route. 3 With the gynecologic advancement in endoscopic surgery, laparoscopic hysterectomy is becoming more appealing to patients and their gynecologists, especially with the Da Vinci Robotic System (DRS) assistance. 4
Vaginal hysterectomy is the most preferred approach by gynecologists due to the lower associated morbidity and quick recovery time.5,6 If the patients' clinical findings are suitable and it is determined that a hysterectomy can be safely performed, then the gynecologist may opt for the vaginal surgical approach. 6
The gynecologist will provide the patient with all the methods of hysterectomy when clinically indicated. The type of hysterectomy must be decided with the patient and her gynecologist based on the medical history, clinical findings such as uterine size, the surgeon's experience, equipment availability, and the patient preference.
Most studies about hysterectomy are retrospective with the comparison of two procedures such as laparoscopic-assisted vaginal hysterectomy with traditional abdominal hysterectomy or robotic compared with conventional laparoscopic hysterectomy. In this study, we compared the three methods of hysterectomy performed in this center. All the procedures were performed by one surgeon (the author). All the laparoscopic-assisted vaginal hysterectomy cases were converted to Da Vinci robotic laparoscopic hysterectomy (RLH) in January 2008. This change occurred due to the availability of the robotic system at the hospital as well as the comfort level of the surgeon to perform the procedure. There was no conversion to conventional laparoscopic hysterectomy in our case and, subsequently, no conventional laparoscopic hysterectomy in our study.
An overview of the three methods of hysterectomy will enable the gynecologists to evaluate which method of hysterectomy they prefer and which method the gynecologists are most comfortable with performing on their patients. The main concern is what is best for the patient's clinical outcome with consideration of the cost involved in each procedure.
Total vaginal hysterectomy (TVH) and RLH have less length of hospital stay than total abdominal hysterectomy (TAH). TAH and RLH have higher hospital charges than TVH, but there was no significant difference between TAH and RLH (Table 1).
RLH, robotic laparoscopic hysterectomy; TAH, total abdominal hysterectomy; TVH, total vaginal hysterectomy.
Materials and Methods
This was a retrospective study for all consecutive hysterectomy cases (n=203) performed by the same surgeon and assisted by a surgical assistant from January 1, 2008, to July 31, 2013. The cases were performed at Emory Saint Joseph's Hospital in Atlanta, GA. Patients' electronic medical records were used to collect data on patient characteristics (age, body–mass index [BMI], ethnicity, and parity), length of hospital stay, operative time, estimated blood loss (EBL), and total charges. A patient questionnaire was given by mail, in person, or over the phone to collect data on postoperative outcome (patient pain level, days until self-care, days of pain analgesic use, days until first bowel movement, days until returning to work, and weeks until first intercourse).
All patients were positioned in the lithotomy position with the use of Allen stirrups. Patients were placed with severe flexion of the legs for TVH and very small flexion of legs for TAH and RLH. TAH was performed through a Pfannenstiel incision. A harmonic scalpel (Ethicon, Inc.) was used during the hysterectomy portion, especially when dissecting the bladder and cutting through the vaginal cuff. RLH was performed with a 12-mm robotic zero-angle laparoscope (Intuitive, Inc.). Two 8-mm trocars were placed in the anterior axillary line with one on each side of the abdomen about 1–2 inches above the umbilical level. There was also another 12-mm SurgiQuest trocar (SurgiQuest Company) in the right midaxillary line about 1–2 inches below the umbilical level (Fig. 1). The cosmetic appearance of the scars was excellent due to the location of the trocars further laterally. The location also minimized the collision of the robotic arms.

Trocars placement–Da Vinci robotic laparoscopic hysterectomy (RLH). Color images available online at www.liebertpub.com/gyn
Statistical analysis was performed using JMP 10.0.2 for Windows. Tukey–Kramer tests were used for comparing means of age and BMI within each group. Steel–Dwass tests were used to compare means of length of hospital stay, operative time, EBL, total charges, and all postoperative patient questionnaire results within each group. Pearson chi-square tests were used for comparing ethnicity and parity distributions. Statistical significance was set with an alpha level of 0.05.
Results
Patients' characteristics by the surgical group are shown in Table 2. No statistically significant differences were observed in mean age, mean BMI, ethnicity distribution, or parity distribution between the three surgical groups. The total patient population age ranged from 28 to 77 years with a mean age of 47 years and standard deviation of 8.4 years. Mean BMI was 29.2 kg/m2, and the BMI standard deviation was 6.2 kg/m2. Seventy percent of the patients were African American. The most frequent parity was 2 (38%).
p<0.05, significantly different with hysterectomy group.
BMI, body mass index; SD, standard deviation.
The uterine size had a major impact in the decision-making of the type of hysterectomy to be performed. In our study, the average uterine weight was 232.95 gm in TVH, 440.34 gm in TAH, and 137.10 gm in RLH. The pathologic diagnosis in all types of hysterectomy leiomyoma (n=95; 46.80%), adenomyosis (n=51; 25.12%), and combined leiomyoma and adenomyosis (n=51; 25.12%). Ten patients had other diagnoses such as severe pelvic adhesions and uterine prolapse. Six patients had pelvic endometriosis combined with leiomyoma or adenomyosis (four underwent TAH, one underwent RLH, and one underwent TVH). All cases of TVH had no history of abdominal surgery and repair of enterocele was performed in 37% of them.
All cases were completed without conversion to laparotomy. One case had a small opening in the bladder dome, which was repaired robotically during the RLH procedure.
TAH had a significantly higher hospital stay of 2.71 days (95% CI: 2.70–2.73) versus TVH with 1.62 days (95% CI: 1.57–1.67) and RLH with 1.38 days (95% CI: 1.36–1.40). Means and 95% confidence intervals of length of hospital stay for each surgical group are displayed in Figure 2. RLH had a significantly higher operative time (202 minutes, 95% CI: 190–210) versus TAH (175 minutes, 95% CI: 165–184) and TVH (139 minutes, 95% CI: 118–160). Means and 95% confidence intervals of operative time for each surgical group are displayed in Figure 3. TAH had a significantly higher EBL (197 mL, 95% CI: 142–251) versus RLH (98 mL, 95% CI: 89–107) and TVH (116 mL, 95% CI: 91–142). Means and 95% confidence intervals of EBL for each surgical group are displayed in Figure 4. TAH ($19,135, 95% CI: 18,273–19,991) had significantly higher total charges than TVH ($15,354, 95% CI: 13,788–16,918). Total charges for RLH ($18,255, 95% CI: 17,644–18,866) were significantly higher than TVH and not significantly different from TAH. Means and 95% confidence intervals of operative time for each surgical group are displayed in Figure 5.

Mean hospital stay in days with 95% CI error bars for each surgical group. Color images available online at www.liebertpub.com/gyn
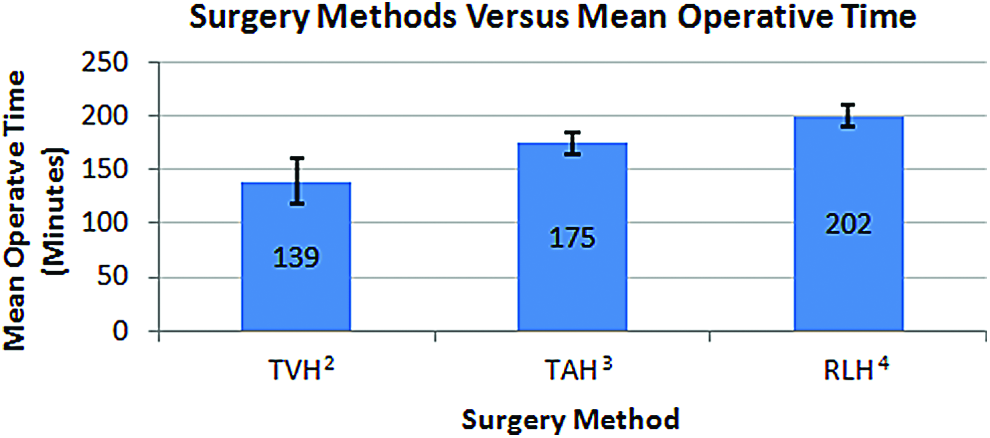
Mean operative time in minutes with 95% CI error bars for each surgical group. Color images available online at www.liebertpub.com/gyn

Mean estimated blood loss in milliliters with 95% CI error bars for each surgical group. Color images available online at www.liebertpub.com/gyn
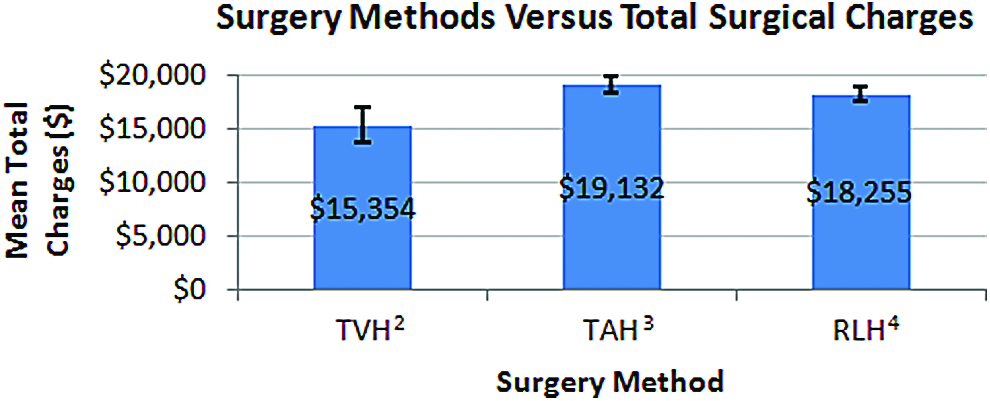
Mean total charges in dollars with 95% CI error bars for each surgical group. Color images available online at www.liebertpub.com/gyn
There was a significant reduction of the operative time from the cases performed in 2008 to those done in 2013 (p<0.05), which proves that the learning curve was a major factor in the reduction of RLH operative time (Fig. 6). For every cumulative surgical RLH procedure, the operative time decreased by 0.05 minutes (p<0.05). This suggests that there is a significant relationship between operative time and EBL (p<0.05). For every 1 minute increase in operative time, there is a 0.08 mL increase in EBL (p<0.05). RLH on average has the lowest EBL, compared with the other surgical methods, but the largest mean operative time. All results are summarized in Table 1.

RLH operative time by year of operation. Color images available online at www.liebertpub.com/gyn
TAH had significantly higher reported postoperative pain level and days of analgesic use than TVH and RLH. TAH had significantly higher days until self-care than TVH, and TAH had significantly higher days until returning to work than RLH. There was no significant difference across all groups for days until first bowel movement or weeks until first intercourse. Means of patient questionnaire results and comparison summaries are listed in Table 3.
p-Value, total comparison between all groups using analysis of variance.
BM, bowel movement.
Discussion
Most studies about hysterectomy were comparing two procedures like laparoscopic-assisted vaginal hysterectomy with traditional abdominal hysterectomy or robotic hysterectomy compared with conventional laparoscopic hysterectomy. In this study, we compared the three methods of hysterectomy performed in this center. All the procedures were performed by one surgeon (the author). Our retrospective study of the three groups of all types of hysterectomy demonstrated that each group possesses their own strength and weakness.
TVH is the preferred method by the gynecologists, considering that the clinical findings fit the comfort and safety level of the surgeon who performs the procedure. TVH patients will have no abdominal scar, less blood loss, shorter operative time, and less cost than the other methods. The Johnson et al. (2005) review found no important disadvantages of TVH, compared with any other surgical approach, and thus it remains an excellent option. 7 TVH has limitations because surgeons have a very limited operative field to visualize the pelvic organs and detect abdominal and pelvic disease like bowel adhesions, ovarian lesions, and other pelvic pathology.
In some cases, TAH is the only surgical method that can be performed (e.g., very large uterus >20 weeks in size) when the patients show history of multiple abdominal and pelvic surgeries with high expectation of severely dense abdominal and pelvic adhesions or signs and symptoms suggesting the presence of pelvic endometriosis. The surgeon will expect a higher blood loss, longer hospital stay, and prolonged period before self-care and sexual intercourse. Injecting a diluted solution of vasopressin in injectable saline (1/200,000) under the mucosa around the cervix vaginally (before starting the abdominal approach) and intramural (intra-abdominally) will reduce the blood loss during the TAH. Abdominoplasty can be performed only during TAH, which is much desired by patients with very large uteri, with significant stretching of the abdominal wall. TAH also has a higher cost mostly due to the prolonged hospital stay than RLH and TVH.
With the right amount of training and skill, along with appropriate patient selection, RLH can be highly advantageous. Patients will most likely encounter less blood loss, less postoperative pain, and faster recovery. The length of the operative time and the cost are comparable with TAH and significantly higher than TVH. There are several limitations of conventional laparoscopic hysterectomy. The learning curve is very big because hand movements are counterintuitive and the long instruments working through a fixed entry point are affected by small movements and even tremors can be accentuated. In addition, the instruments have a limited range of motion (dexterity) and often require ergonomically challenging positions. This can result in fatigue and frustration by the surgeons during lengthy cases. Finally, the two-dimensional optics and the unstable camera platform result in loss of depth perception and difficult visualization depending on the stability and skill of the assistant operating the camera. Due to these limitations, many hysterectomies are still done as an open procedure (TAH). However, with the advent of the DRS developed by the Intuitive Surgical and the United States Federal Drug Administration (FDA) approval in April 2005 for gynecologic cases, many hysterectomies, which would have been done with an abdominal incision (TAH), are now being performed with minimally invasive techniques utilizing the DRS (RLH).8,9
Our study involved comparing vaginal, abdominal, and Da Vinci RLH with the clinical outcome and cost. Vaginal hysterectomy is the most preferred approach by gynecologists if the patient's clinical findings are suitable for the procedure.
The use of Da Vinci robot-assisted laparoscopic surgery has grown exponentially, especially in the field of gynecology since it was approved by FDA on April 2005. 10 Robot-assisted and laparoscopic surgery eliminates the need for large morbid and esthetical incisions and reduces blood loss, postoperative pain, use of pain medications, and length of hospital stay.11,12 The first series, which included 11 successful robotic laparoscopic hysterectomies that were performed, was in 2002 by Diaz-Arrastia. 13 In addition, Fiorentino et al. reported a pilot study assessing RLH and patient outcomes in 20 patients with benign conditions in 2006. 13 Two patients were converted to laparotomy because of poor visualization (conversion rate 10%). The mean operating time was 3.2 hours.
Advantages of robotic surgery, compared to conventional laparoscopic and open surgery, are dexterity, more precise movements, tremor reduction, and better visualization of the operating field (magnification and 3D). 14 The difficult minimally invasive surgery is accessible for surgeons without advanced training as it has a short learning curve. Fatigue and frustration become less of a limiting factor for the robotic surgeon, compared to the conventional laparoscopic surgeon.14–16
The major drawback of the DRS is the loss of tactile and force feedback. This can be surmounted by training and partially compensated for by the 3D visual feedback. In addition, placement of the trocars is limited to avoid collision of the robotic arms. However, in the newer Da Vinci robotic XI, this became less of a problem. Placement of the 8-mm trocars at the level of the anterior axillary lines bilaterally in the Da Vinci robotic SI will give the articulated arms a wide range of motions and less collision. The scars of these incisions are much less feasible and more cosmetically acceptable to the patients.
Cost of Robotic Surgery
(A) Equipment: The major difference in the cost of the open, laparoscopic, and robotic procedures is the expense of the specialized equipment. 17 Laparoscopic surgery has a relatively lower case cost as it is multipurpose and can be used by other specialists to perform different types of surgery. 17 Unlike the laparoscopic surgery, the robot has a more limited number of applications. The fixed cost depends highly on the number of cases the robot is able to operate over in its amortized life span. 17 This results in a distinct financial disadvantage because each instrument has a limited preprogrammed number of uses (n=10). Although one would expect equipment costs to decrease with time (analogous to the retail computer market), there has been an increase in costs despite the increase in number of procedures performed nationwide. 18 There has been no decrease in costs of robot-related products due to the lack of market competition. 18
(B) Operative times: Determining the operative cost depends greatly on the operative time, including the time to the start-up procedure, to perform the procedure, and to prepare the room for the next operation. Overall, the setup and breakdown of the robotic system takes significantly longer, compared to the preparation of the laparoscopic or open surgery (Fig. 3). Over the years, certain techniques have developed with the experience of the operating room (OR) staff and the surgeon, which resulted in a shorter operative time and subsequently less cost. The average operative time in 2008 cases was 202 minutes and has been reduced to 88 minutes in 2013 cases.
(C) Hospital stay: In our study, the length of hospital stay was significantly lower in RLH with 1.38 days (95% CI: 1.36–1.40) and TVH with 1.62 days (95% CI: 1.57–1.67), compared to TAH 2.71 days (95% CI: 2:70–2.73). This results in a main financial advantage for the RLH and TVH versus TAH.
(D) Other costs: It is difficult to calculate the amount of savings for sick leave, disability insurance for inability to work, and so forth (comparing RLH, TVH, and TAH), since it varies tremendously among each individual. It is demonstrated in our study that RLH reported a significant lower time when returning to work than TVH and TAH (Table 3).
(E) Allowing patients to resume self-care and professional activities sooner.
Conclusion
Study findings reveal a significantly higher hospital stay in TAH versus all other methods. TAH and RLH had significantly higher total hospital charges versus TVH. TAH had significantly higher EBL than RLH. TAH had higher levels of postoperative pain than RLH and TVH. The learning curve has a significant impact on the operative time of RLH and subsequently on the cost of the procedure.
Footnotes
Acknowledgments
The author thanks Shawky Z.A. Badawy, MD, Professor, Department of Obstetrics and Gynecology, for his review and input in this article. The author thanks Ms. Rebecca Cantrell, BS, Ms. Laura Creech, BS, Ms. Michelle Nunez, BS, for data collection and statistical analysis in this study. Emory Saint Joseph's Hospital's IRB determined that this study is exempt from IRB review pursuant to the provisions of 45 CFR 46.101 (b) (2) and (4).
Author Disclosure Statement
No competing financial interests exist.