
Abstract
Abstract
Introduction
E
Case
A 28-year-old female, with 40 days of amenorrhea, presented with complaints of a sudden onset of pain in the right iliac fossa. She had no history of difficulty in micturition, defecation, or vaginal bleeding. She also had no history of pelvic inflammatory disease (PID) or any contraceptive use such as an intrauterine device IUD. On clinical examination, she was noted to have had signs of shock, with a pulse rate of 108/minute and a blood pressure of 90/70 mm Hg.
This patient's abdomen was slightly distended and both of her iliac fossae were tender. Her routine hematologic and biochemical test results were within normal limits except for mild leucocytosis with neutrophilia. A vaginal examination revealed tenderness in all the fornices. A clinical diagnosis of a possible ruptured ectopic pregnancy or acute PID was made. Her urine showed positive results for a pregnancy test. Transvaginal sonography revealed a right adnexal, hyperechoic mass measuring 30×25 mm. The endometrium was 9 mm thick (∼ 7 weeks) but there was no intrauterine sac. There was moderate free fluid in the pouch of Douglas.
On laparotomy, the right Fallopian tube appeared to be normal but the right ovary was enlarged and hemorrhagic. The left adnexa showed no abnormality. A right sided salpingo-oophorectomy was performed, and the excised specimen was sent for histopathologic examination. On gross examination, the ovary weighed 40 g and measured 3×3.5×2.5 cm. The cut surface showed hemorrhagic areas (Fig. 1). No embryo was identified grossly. The Fallopian tube, measuring 5.0 cm, appeared to be normal. On microscopic examination, the sections showed ovarian stroma along with extensive areas of hemorrhage and scattered chorionic villi (Figs. 2 and 3). This patient's serum human chorionic gonadotropin (hCG) level had not been tested as this patient had presented in an acute condition with shock in the emergency department, but the presence of chorionic villi within the ovarian stroma suggested the likely possibility of an extrafollicular pregnancy.
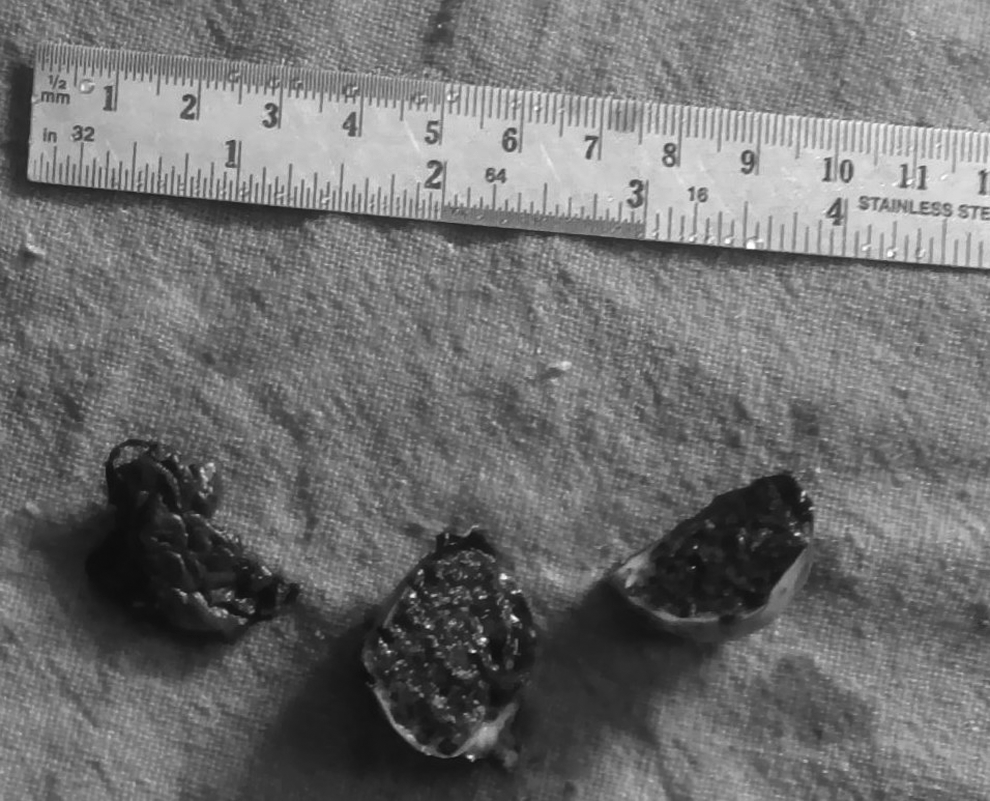
Gross appearance of ectopic ovarian mass.

Photomicrograph showing chorionic villi, trophoblastic tissue, and hemorrhage within ovarian stroma (hematoxylin and eosin, 200 ×).

High-power view confirming the presence of chorionic villi, trophoblastic tissue, and hemorrhage within ovarian stroma (hematoxylin and eosin, 400 ×).
Results
At the follow-up of 6 months, patient is doing well.
Discussion
An ectopic pregnancy is characterized by implantation and development of an embryo outside of the uterine cavity. Primary ovarian pregnancy is a rare entity. The reported incidence is 0.15%–3% of all ectopic gestations. 1
This kind of pregnancy can be classified as primary or secondary. It is called primary when the ovum is fertilized while still within the follicle and secondary when fertilization takes place in the Fallopian tube and the conceptus is regurgitated later to be implanted in the ovarian stroma. These pregnancies can be intrafollicular or extrafollicular. An intrafollicular pregnancy is invariably primary in nature and an extrafollicular pregnancy may be primary or secondary in nature, wherein ovarian tissue is usually absent in the gestational sac.1,2
In the current case, chorionic villi were seen within the ovarian stroma, suggesting the likely possibility of an extrafollicular ovarian pregnancy.
The Spiegelberg criteria define ovarian pregnancy as occurring when there is: (1) an intact ipsilateral tube that is clearly separate from the ovary; (2) a gestational sac occupying the position of the ovary; (3) a sac connected to the uterus by the ovarian ligament; and/or (4) histologically proven ovarian tissue located in the sac wall. 3
Risk factors, such as PID and prior pelvic surgery, may not play significant roles in the etiology of an ovarian pregnancy, in contrast to patients with tubal pregnancies. An IUD is found in 14%–30% of patients with a nonovarian extrauterine pregnancy while this device is found in proportions ranging from 57% to 90% of patients with primary ovarian pregnancy. This phenomenon could be explained by altered tubal motility, thereby facilitating the implantation in the ovary. The increase in the incidence of ovarian pregnancy is closely related to the use of the IUD as a contraceptive method. These devices prevent uterine implantation but do not provide protection against ovarian implantation. Ovarian pregnancies usually terminate in rupture during the first trimester in 91.0% cases, 5.3% in the second trimester, and 3.7% in the third trimester. Only 1 case has been reported in the literature, wherein an ovarian pregnancy had progressed to full-term delivery.1,2,4
Ovarian pregnancy can be misdiagnosed as a ruptured corpus luteum cyst in 75% of cases. The diagnosis is often made at surgery and requires histologic confirmation. A correct diagnosis of ovarian pregnancy during surgery is only possible in 28% of cases, because an ovarian pregnancy is difficult to differentiate from a hemorrhagic corpus luteum intraoperatively. 5
Diagnosis is based on the classic description of a cyst with a wide ectogenic outer ring, using ultrasound. Although ultrasound may suggest the diagnosis, surgery (laparoscopy or laparotomy) remains the best method of differential diagnosis and management. 5
A high index of suspicion is based upon a combination of ultrasound findings (both grayscale and color Doppler) and high levels of serum hCG. Ultrasound diagnosis of an ovarian ectopic pregnancy may be different, such as serum-cell tumors or other ovarian pathology. Diagnosis is suspected during laparoscopy or laparotomy and confirmed by histopathology. 5
Treatment of almost all known ovarian ectopic pregnancies has been surgical. In addition, case reports have described successful treatment with methotrexate. However, the preferred mode of treatment is oophorectomy via either laparotomy or laparoscopy. Fertility after ovarian pregnancy has been reported to be unmodified. 5
Conclusions
Although ovarian pregnancy is a rare event, awareness of this condition is important for reducing its associated morbidity and mortality. Hence, it can be concluded that ovarian ectopic pregnancy should be considered as one of the important differential diagnoses in a female of reproductive age presenting with an acute abdomen.