
Abstract
Abstract
Introduction
P
We present a case involving a patient with Crohn's disease complicated by prior rectovaginal and perianal fistulas with bothersome stage 3 uterovaginal prolapse and a pessary-induced rectovaginal fistula, who underwent a single-stage fistula repair and prolapse correction without colonic diversion.
Case
Our case is a 57-year-old, para 0, postmenopausal, obese Caucasian female who presented to the Female Pelvic Medicine and Reconstructive Surgery clinic with complaints of symptomatic uterine prolapse and stool within the vagina. Her medical history was significant for longstanding Crohn's disease complicated by recurrent rectovaginal fistulas several years ago. Upon review of her prior records, she had required multiple incision and drainage procedures and closure of her fistulas with a prior diverting colostomy performed to aid in healing. Ten years ago, her colostomy had been reversed.
Her Crohn's disease was well controlled on infliximab and she denied any rectal or vaginal drainage or fistulous tracts during that time. A year before presentation to our clinic, she saw an outside provider for complaints of pelvic organ prolapse and a ring pessary was placed. This was cared for by the outside provider with office visits, removal, and cleaning every 3–4 months. She had been on esterified estrogen/methyltestosterone hormone replacement therapy for 11 years.
At the time of her annual examination with her primary care provider, she mentioned the presence of stool in her vagina for several days in addition to concerns for worsening vaginal protrusion. She was referred to our Urogynecology Division, where she was seen the following week. She denied any abnormal vaginal bleeding or dyspareunia.
On examination in the urogynecology clinic, she was noted to have atrophic vaginal epithelium with an attenuated perineal body. She had a stage 3 uterine pelvic organ prolapse with the presence of a stage 3 prolapse involving the anterior, posterior, and apical compartments. A grossly evident posterior fistulous tract 2 cm in diameter was noted 6 cm proximal to the posterior vaginal introitus to the left of the midline.
Due to the patient's history of Crohn's disease, she was subsequently seen by our colorectal surgeon and underwent a colonoscopy with biopsy, which showed a chronic active proctitis without granulomas or dysplasia identified (Fig. 1). Evidence of active Crohn's disease was not identified within the colon.
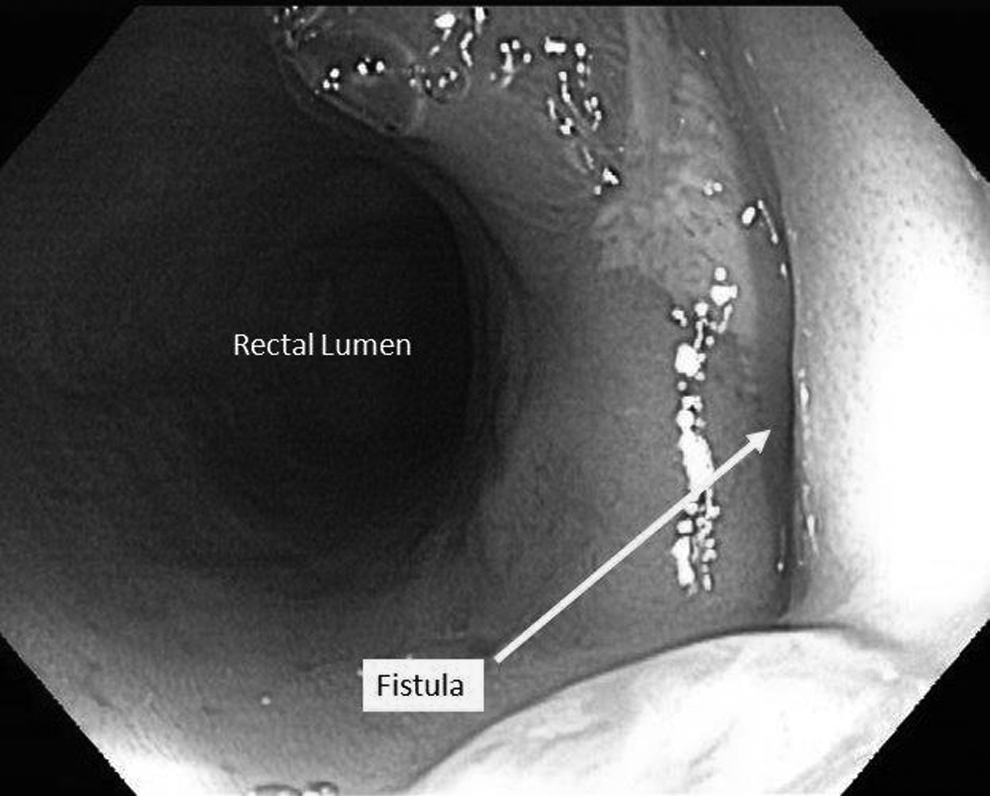
Colonoscopy revealing chronic active proctitis and large anterior rectovaginal fistula.
The patient underwent a combined procedure with colorectal surgery, which included a transvaginal rectovaginal fistula repair with posterior repair, bilateral sacrospinous ligament hysteropexy through a posterior approach, anterior paravaginal repair, perineorrhaphy, cystoscopy, and anoscopy. In this procedure, after sigmoidoscopy was performed, revealing healthy appearing rectal mucosa, the fistula was closed in a vertical manner with interrupted 2-0 polyglactin 910 suture. Due to the patient's significant prolapse, a redundant amount of rectovaginal fascia allowed for a multilayered fistula closure in three layers. Subsequently, the pararectal spaces were dissected bilaterally and two 2-0 prolene sutures were placed on the lateral 1/3 aspects of the sacrospinous ligaments on each side. The opposite ends of these sutures were then attached to the proximal-most aspect of the rectovaginal fascia and the posterior aspect of the cervix and held without tension. The anterior vaginal wall was then opened and dissected to reveal lateral defects on both sides as well as an apical transverse defect. A vaginal–paravaginal repair was performed by attaching the lateral-most aspects of the pubocervical fascia to the arcus tendineous fascia pelvis bilaterally with three sutures of 2-0 polyester suture on each side. An apical transverse defect repair was then performed by reattaching the apical-most aspect of the pubocervical fascia to the anterior cervical stroma. Once all sutures were tied down, it was assured that no undue tension was present along the fistula suture line and excellent elevation of the uterus was noted. A native tissue posterior colporrhaphy was then performed. No foreign materials or grafts were used. At the conclusion of the procedure, the patient had a normal sigmoidoscopy without the evidence of fistula patency or rectal injury. The estimated blood loss was 150 mL. The final pathology was consistent with the fistula tract.
The patient had an uncomplicated postoperative recovery and was discharged home from the hospital on postoperative day 2. At the 12-month postoperative follow-up, the patient denied symptoms of recurrent pelvic organ prolapse or fistula. She had a normal gynecologic examination without evidence of notable pelvic organ prolapse or recurrent fistula.
Discussion
Our case is unique in the following three ways: it involved a successful combined transvaginal approach for both fistula correction and prolapse repair, it involved a uterine suspension, and it did not involve an intestinal diversion procedure despite the patient's known inflammatory bowel disease.
The acuity and potential complications associated with Crohn's disease tend to preclude that specific patient population from undergoing many pelvic floor corrective procedures, and if performed, they are rarely done at the same time as a fistula correction. Fistula repair alone has only a 44% success rate in patients with active Crohn's disease with a high likelihood of recurrence. 1 Although the majority of rectovaginal fistulas occurring in inflammatory bowel disease patients are due to an inflammatory disease, other causes exist, including iatrogenic causes, foreign body erosion, and inflammation. There have been a limited number of published cases in the literature of pessary-induced rectovaginal fistula, with the documented cases being attributed to neglect.2,3 However, there are no previous reported attempts to transvaginally repair both a rectovaginal fistula and uterine prolapse with a uterine-sparing technique in the same procedure.
Without any prior literature available, the decision to proceed with a single-stage combined procedure rested in the fact that the patient's tissue quality appeared to be healthy, and a preoperative colonoscopy revealed no evidence of mucosal disease within the rectum attributable to the patient's Crohn's disease. In addition, we were reassured by the fact that the patient's Crohn's disease was well controlled on a single biologic agent. Thus, our surgical plan was guided by the basic surgical principles of fistula repair. This included a preoperative bowel preparation and avoidance of hysterectomy to minimize potential infectious complications. We also undertook a multilayered repair without overlapping suture lines and the use of delayed absorbable minimally inflammatory suture materials to maximize tissue healing. Furthermore, we selected procedures such as extraperitoneal sacrospinous hysteropexy that would minimize the operative time and potential infectious complications. We were aware that performing surgery as a staged approach may subject the patient to additional perioperative complications, a prolonged duration of convalescence, and increased cost to the patient.
In selection of the method for prolapse repair, we chose procedures that would be both effective, time-efficient, and minimize native tissue damage. Specifically, this formed our decision to preserve the uterus and perform a sacrospinous hysteropexy. Our decision to leave the uterus in situ avoided entrance into the peritoneal cavity, which could potentially increase operative complications as well as postoperative infectious morbidity. In addition, we utilized the patient's posterior and apical compartment anatomy and redundant tissue to aid in the rectovaginal fistula repair allowing a multilayered closure. Despite the large size of the fistula, we were able to avoid the use of foreign or graft materials, which may potentially act as a nadir for infection if any communication between the vagina and rectum continued to exist. 3
Although a recent small chart review by Alshaikh noted sacrospinous hysteropexy to have higher rates of recurrence, compared to hysterectomy followed by a uterosacral ligament suspension, a systematic review by Detollenaere et al. concluded that based on limited studies, the uterus-preserving procedure was associated with shorter operating time, shorter hospital stay, and less blood loss.4,5 Prior literature has suggested that sacrospinous hysteropexy was associated with favorable postoperative outcomes in 62%–100% of patients, with improved quality of life and sexual function and vaginal anatomical outcomes similar to vaginal hysterectomy with a sacrospinous ligament suspension. 6 In this case, our patient was noted to have an absence of prolapse symptoms and no recurrence of the rectovaginal fistula after 1 year of follow-up.
Regarding the fistula repair itself, it was closed in multiple layers without the use of grafts. Multilayer closure and a transvaginal approach has a high cure rate between 80% and 100% based on previous literature.1,7 Although graft augmentation has been found to be a beneficial addition to the procedure in select cases, it was excluded in this instance in the setting of Crohn's disease and concern for graft-related complications. 3
In summary, the preceding case provides an example of successful combined repair of a large rectovaginal fistula and stage 3 uterovaginal prolapse using approaches that minimize native tissue damage and potential complications. To consider such a treatment plan, it was of utmost importance to determine the stability of the patient's Crohn's disease. Our patient was in a quiescent stage of her Crohn's disease and based on her preoperative evaluation with colorectal surgery, the fistula was diagnosed as likely to be arising due to pressure necrosis associated with the patient's pessary leading to anterior rectal erosion. Therefore, the risk for fistula recurrence was low, and we could therefore be more aggressive with her treatment regimen. If considering a single-stage combined procedure, we suggest careful patient selection within a multidisciplinary setting to optimize treatment outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.