
Abstract
Abstract
Introduction
E
The da Vinci surgical platform consists of a surgeon console, a three-dimensional camera system, and a patient-side cart controlling wristed laparoscopic instruments. This system was approved for use in general laparoscopic surgery on July 11, 2000, and for gynecologic laparoscopic procedures on April 26, 2005 in the United States (U.S.). The platform's uses have expanded greatly in the past decade to include both benign gynecologic procedures and complex cancer operations. By 2012, a total of 373,000 robotic procedures were performed in the U.S. this number had increased from 228,000 in 2010 to 292,000 in 2011. 1 In 2012, gynecologic surgery comprised 222,000 procedures; of these, there were 176,000 hysterectomies. 2
There have been multiple studies comparing robotic to laparoscopic or open techniques for gynecologic surgeries. Robotic surgeries have shown advantages over open surgery and results comparable to traditional laparoscopy, but these surgeries have incurred increased costs.3,4 Recently, however, there have been safety concerns and high-profile lawsuits involving robotic surgery, especially robotic hysterectomy. Intuitive Surgical, Sunnyvale, CA, is currently named in approximately 50 product-liability lawsuits filed by patients who claim injury or relatives of patients who claim death as a result of robotic procedures. 1
Clearly, instrumentation is not the only explanation for robotic-associated complications. Inadequate training, poor judgment, and the unique aspect of robotic surgery wherein haptic feedback is absent are other contributing factors to mishaps during robotic surgery. In an effort to facilitate reporting of device-related complications, the U.S. Food and Drug Administration (FDA) Manufacture and User Device Experience (MAUDE) Database was developed in June 1993 to accept voluntary reporting from health care professionals, patients, and consumers regarding adverse events (AEs) related to FDA-approved devices. Manufacturer reporting began in August 1996. Manufacturers are mandated to submit Medical Device Reports (MDRs) when becoming aware of device malfunctions or defects. Patients and health care providers may also submit reports on a voluntary basis.
Each year, the FDA receives several hundred thousand MDRs of suspected device-associated deaths, serious injuries, and malfunctions. The FDA uses MDRs to monitor device performance, detect potential device-related safety issues, and contribute to benefit–risk assessments of these products. Underreporting of robotic complications has been established as a major concern. 5 This creates a significant barrier to establishing safety and quality measures for robotic surgery. As a result of changes to reporting practices made in 2012, claims by plaintiff attorneys of patient injuries are required to be investigated and are usually submitted as MDRs. This led to a surge of new reports being filed in 2013.
The intent of this study was three-fold: first, to describe the use of the MAUDE database and encourage increased voluntary reporting of robotic complications associated with gynecologic procedures by hospitals, providers, and consumers; second, to investigate the trends in AE reporting related to robotic gynecologic surgery; and third, to describe the most common types of injuries and instrumentation malfunctions.
Materials and Methods
This study was conducted in compliance with the Dignity Health St. Joseph's Hospital and Medical Center's (Phoenix, AZ) institutional review board, which granted exempt status to this review of de-identified public data. The MAUDE database was accessed via the FDA website and searched by device name and event type from January 1, 2005 to December 30, 2013 (as reporting on the da Vinci system started in 2005). The dataset was then sorted, based upon event date to capture reports within the study period of January 1, 2003 to December 31, 2012. There is often a delay in reporting, therefore the event data from 2013 was excluded as immature data.
The event descriptions and manufacturer narratives in the database for events occurring during the study period were printed and cataloged. Each report of patient death or injury was individually reviewed to determine the type of surgery that was performed. Any general gynecology, urogynecology, or gynecologic oncology case was retained for further review. The following information was then abstracted and entered into a database: date of surgery and date of report; type of surgery; indication for surgery; injury sustained; interventions required; report of device malfunction; and whether or not the case was involved in legal proceedings. The malfunction data was processed separately, abstracting the instrument involved, the type of malfunction, whether or not patient harm resulted from the malfunction, and interventions performed in response to patient harm. This information was then codified in the database and processed to identify trends and associations.
Results
A total of 93 deaths related to robotic surgery were reported during the study period, and the number of reported deaths increased each year (Fig. 1). Thirty-two percent of these deaths occurred after gynecologic procedures. Urologic and cardiothoracic procedures were the second and third, respectively, most common procedure types resulting in death. Hysterectomy was the most likely procedure to result in death (Table 1). The most common cause of death after robotic gynecologic procedure was sepsis (a majority of which followed unrecognized bowel perforation), followed by hemorrhage and then pulmonary embolus (Fig. 2).
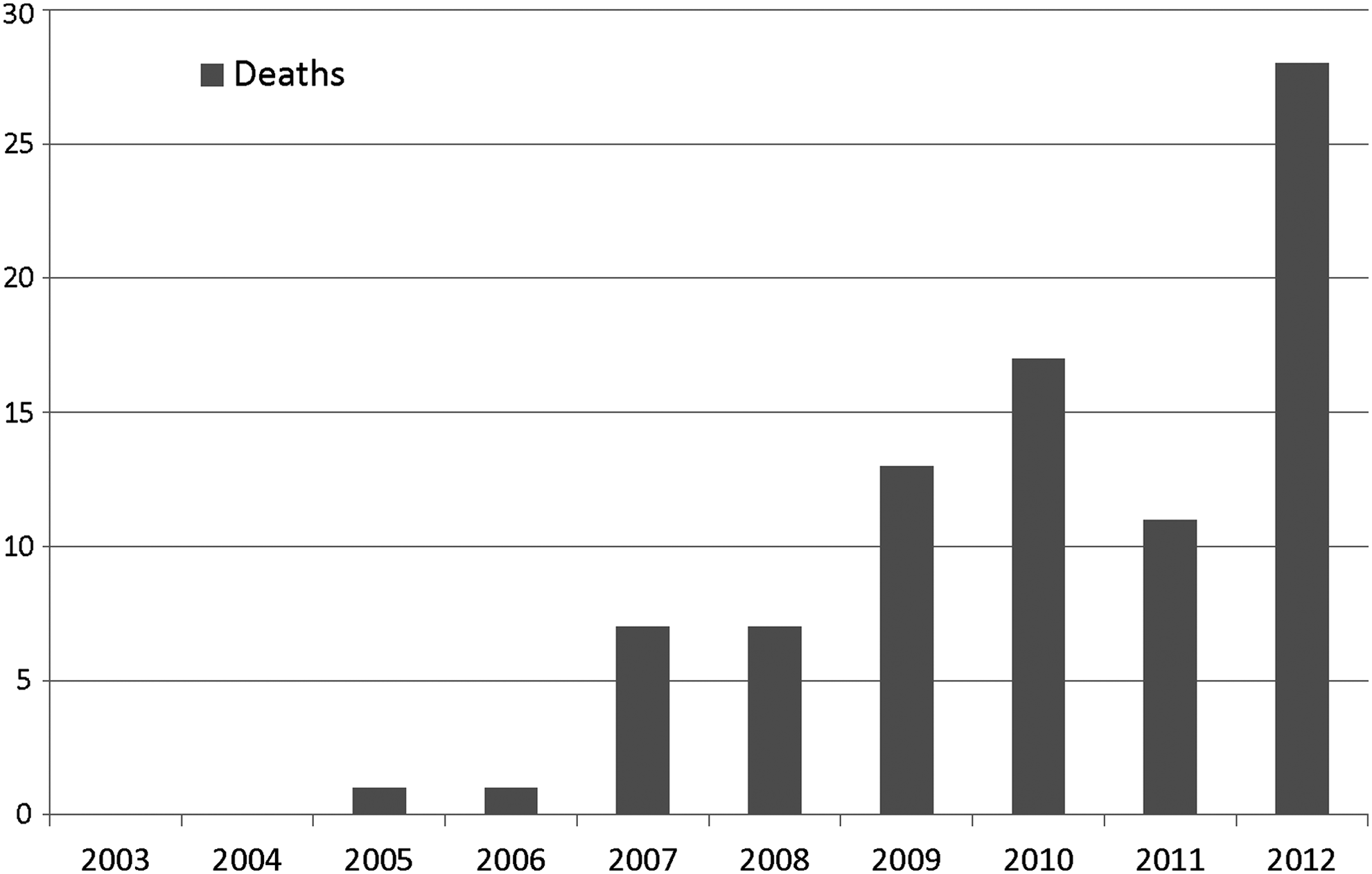
Reported deaths related to robotic surgery. Reporting of such deaths increased from 2003 to 2012.

Causes of death in gynecologic robotic procedures. Sepsis was the most common identifiable cause of death related to gynecologic robotic procedures, followed by hemorrhage and then pulmonary embolus.
TECAB, totally endoscopic coronary artery bypass; ENT, ear-nose-and-throat; TORS, trans-oral robotic surgery.
Injury reporting also increased during the study period (Fig. 3). Gynecologic cases represented 61% of reported injuries. The most commonly performed gynecologic procedure was hysterectomy (Table 2). Abnormal uterine bleeding was the most common indication for surgery, followed by pelvic pain and then fibroids. Many procedures listed multiple indications for surgery. The most common complications were genitourinary-tract injuries, including 86 ureteral injuries, 29 vesicovaginal fistulae, 30 ureterovaginal fistulae, and 43 bladder injuries. Although 64 intraoperative cystoscopies were performed, only 7 were diagnostic of urinary-tract injury. Ureteral stenting, ureteral reimplantation, and small-bowel resection or repair were the most common interventions performed (Table 3). Approximately half (50.6%) of injuries were delayed in presentation until after patients had been discharged to go home. Reoperation was necessary in 214 cases and 189 required readmission (defined as a >24 hour inpatient stay).

Gynecologic robotic injury reporting. Reporting of such injuries increased from 2003 to 2012.
Ureteral stenting and percutaneous nephrostomy tubes are n=1 for unilateral or bilateral procedures in the same patient.
IVCF, inferior vena cava filter.
Within the 10 years studied, 177 robotic malfunctions were reported (Fig. 4). Conversion to open procedure was necessary in 20 patients. Aborting a procedure or converting to open procedures occurred as a result of loss of visualization caused by camera and/or system errors, or malfunction of the master tool manipulator. Of 40 reports of equipment pieces breaking off into a patient, most (78%) were retrieved successfully (Table 4). The endoscopic instrument control system was most commonly cited piece of equipment to malfunction, followed by the insulating tip cover for the monopolar scissors. Arcing current caused by damaged monopolar insulating tip covers led to 5 of 6 reported internal-organ burn injuries. Of 2 reports of skin burns, both cited grounding of the patient through the robotic arm, possibly because of abnormally high cautery settings. Two operating room fires were also reported.
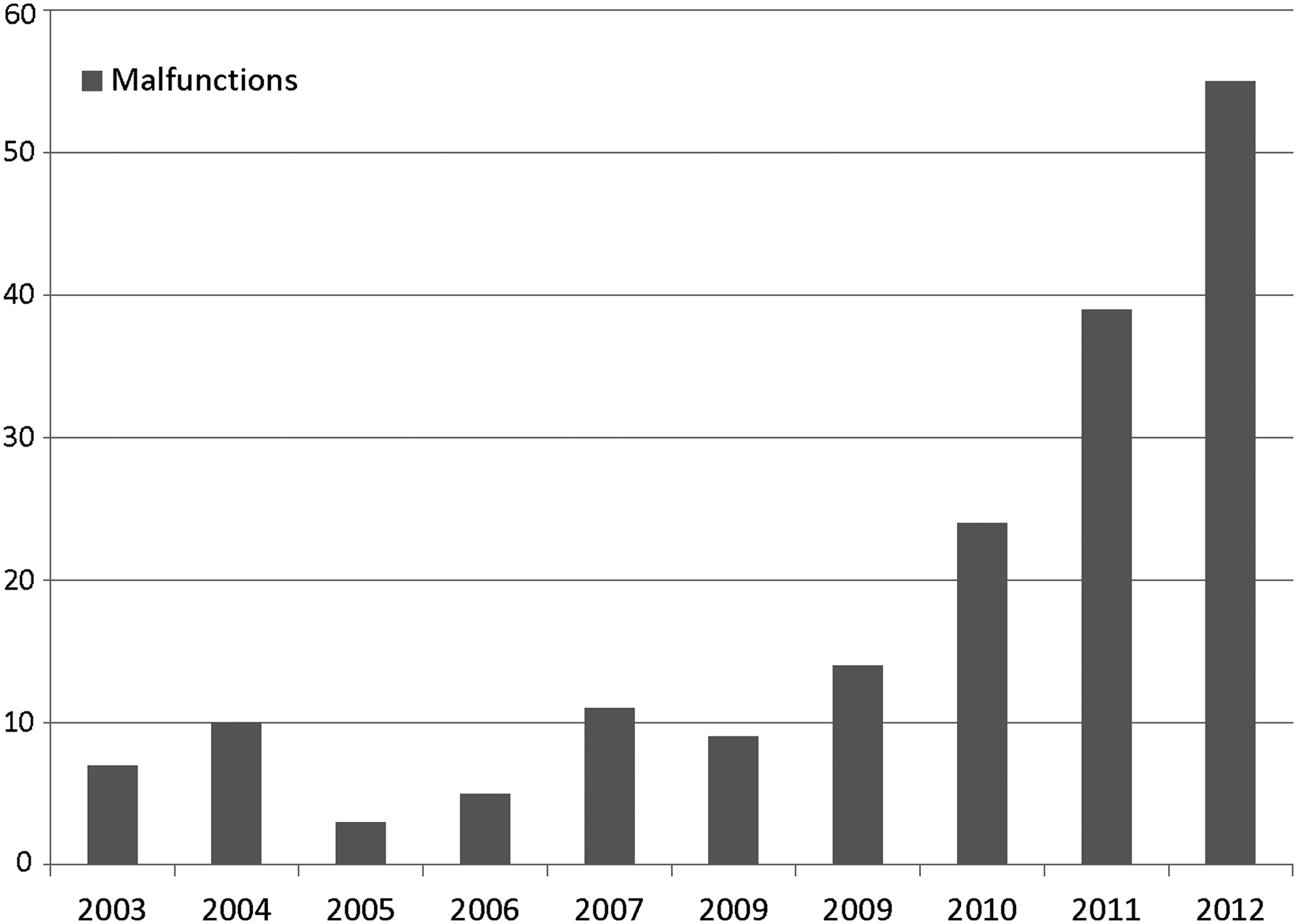
Robotic device malfunctions. Reports of such malfunctions increased during the study period (in all surgical specialties including non-gynecologic areas).
Excluding unnecessary anesthesia from aborted procedures and conversion to laparotomy, the reported rate of injury from malfunction was 12%, of which there were 9 retained foreign bodies, 3 burns to internal organs, and 3 skin burns. During the study period, the total number of robotic procedures was increasing. While specific numbers were not available for all years studied, there was a slight increase in the reported death, injury, and malfunction rates (Table 5). The reported death rate per procedure in 2008 and 2009 was 0.006%. This increased to 0.007% in 2010 and 2012, with an intervening decrease to 0.004% in 2011. The reported rate of malfunctions had steadily increased in the years for which the current authors had data. The rate of reported injuries from gynecologic procedures increased from 0.06% in 2010 and 2011 to 0.08% in 2012.
Discussion
This study endeavored to describe trends in complication reporting for robotic gynecologic surgery. The number of AEs being reported in robotic gynecologic surgery is increasing. This, in part, reflects the increase in numbers of procedures being performed. It may also be a result of legal proceedings and changes to MDR submissions. Another goal of this study was to describe the most common injuries associated with robotic gynecologic surgery. Whereas infectious or bleeding complications are more common in open procedures, genitourinary-tract injuries are the most commonly reported injury in robotic surgery. Injuries in robotic surgery are often delayed in presentation, and result in the need for reoperation and hospital readmission.
One limitation of the MAUDE database is that the information contained within the reports is variable in detail and reliability. The reports can come from any source, including patients and lawyers. There is no ability to determine causality in a majority of AEs. Indeed, many of the reported injuries in the database occurred from trocar placement, which is not specific to the robotic platform. There is also a great deal of underreporting of AEs, and the incident rate cannot be abstracted from the data. The increased AE reporting demonstrated in the study period can be attributed both to increasing numbers of procedures being performed each year as well as changes to reporting requirements in 2012 to mandate reporting of any cases involved in litigation. Of the reported injuries, 81% were associated with legal proceedings. The database is useful for its large population and accessibility. As the number of robotic gynecologic procedures increases, it is useful to understand the most common types of robotic-related AEs and track the prevalence of these events. A more thorough method of tracking robotic complications is needed.
As cost-effectiveness in health care is increasingly scrutinized and reimbursement allotted according to quality indicators, it is important to recognize areas where quality may need to be monitored more effectively. Currently, the most frequently used quality indicators in gynecologic surgery are the Surgical Care Improvement Project (SCIP) measures. Increased use of outcome measures such as the incidence rate of urologic injury during hysterectomy may lead to patient safety improvements. Better monitoring of AEs in robotic surgery may help define appropriate use of robotic surgery and develop safety standards for its use.
One component of safe robotic surgery is adequate training and volume. Low surgical volume in robotic surgery is a risk factor for complications, and it has been found in other surgical specialties that the most complications arise from low-volume surgeons. 6 A variable minimum number of robotic procedures necessary to become proficient has been reported as being anywhere from 9 to 91 robotic surgeries.7–9 A more-standardized method of training and credentialing robotic surgeons should be studied to determine if this could be effective for limiting AEs.
Conclusions
Currently, reporting of AEs related to robotic surgery by health care professionals is voluntary. As a result, it is difficult to ascertain their true incidence. As AEs are increasingly being monitored as metrics of health care quality, it is important for surgeons to embrace active management of reporting systems. If gynecologic surgeons are not prepared to lead the way on quality improvement in robotic surgery, we may face future mandated reporting from health care legislators. The Affordable Care Act has already changed the purpose of the Physician Quality Reporting System (PQRS) from a voluntary reporting system to a mechanism to quantify compliance with quality reporting, leading to decreased reimbursement for noncompliance. While the PQRS Measures List currently has few items directly related to outcomes in gynecologic surgery, such measures are likely to join the growing list of quality care metrics. 10 The current authors recommend reporting of robotic surgical complications at the hospital level.
Footnotes
Disclosure Statement
There are no reported conflicts of interest for any of the authors of this article.