
Abstract
Abstract
Introduction
A
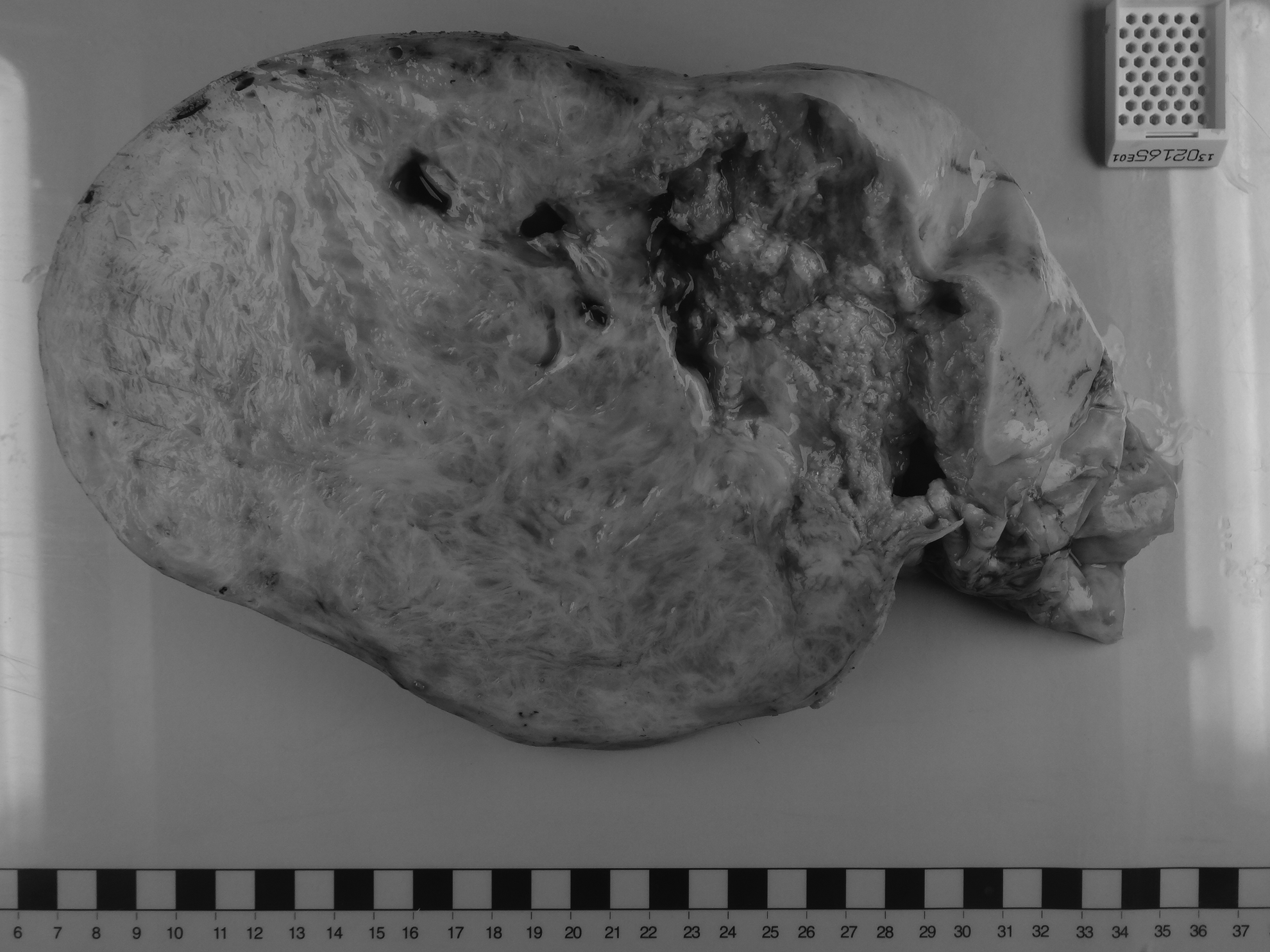
Left ovarian fibroma.
Case
A 57-year-old woman, presented to emergency medical services with a history of anorexia, abdominal pain, and abdominal distension over several months. She also complained of a chronic cough that had been persistent for 1 year; this symptom was associated with worsening dyspnea. There was no history of fever, urinary symptoms, or change in her bowel habits. She had been menopausal for 9 years. She was para 1 with a normal vaginal delivery. There was no history of abnormal cervical smears in her past. She had no significant medical or surgical history, and there was no family history of note. She was an overseas visitor from Peru.
On examination, she was noted to be cachectic. She was tachycardiac at 115 beats per minute and hypertensive at 153/96 mm Hg. Her oxygen saturation was 91% on room air. She was afebrile. On chest auscultation, it was noted that there was reduced air entry in the right lung base but there was no crepitation. No peripheral lymphadenopathy was noted. Her breast examination was norzmal. Her abdomen was grossly distended and tense with mild left-sided tenderness. Shifting dullness was present indicating the presence of ascites. It was difficult to determine any significant finding on pelvic examination because of the presence of tense ascites.
The investigations were as follows. Full blood count: hemoglobin, 14 g/dL; white blood cells, 8.4×109; platelets, 628×109. Electrolytes, urea, and creatinine levels were normal. C-reactive protein level was 20.7 mg/L. Amylase and LFTs were normal, except for reduced albumin at 23 g/L. CA-125 was raised at 3267 kU/L. The other tumor markers were normal. Chest X-ray showed a right pleural effusion. Abdominal X-ray result was normal.
Computed tomography scans of this patient's thorax, abdomen, and pelvis showed a large right-sided pleural effusion; a 20-cm solid-cystic right adnexal mass; 3 other similar solid-cystic masses within the peritoneal cavity; a 3-cm calcified parenchymal liver mass; an 8-cm complex mass involving the umbilicus; an omental cake; and a thickened mesentery with no pelvic or para-aortic lymphadenopathy.
The differential diagnosis was advanced ovarian carcinoma with pelvic, peritoneal involvement and pleural effusion (Stage 4) or disseminated mycobacterial tuberculosis infection. Cytologic examination of the pleural and peritoneal fluids showed lymphocytic effusions but no evidence of malignancy. Microbiologic assessment of the ascitic fluid showed no evidence of acid-alcohol fast bacilli either on microscopy or via culture.
This case was discussed in a multidisciplinary team meeting, and a decision was made to consider neoadjuvant chemotherapy pending a cytologic or histologic confirmation of malignancy.
However, a percutaneous needle core biopsy of the omentum showed the presence of fibrotic tissue only. In view of this patient's increasing abdominal discomfort, she underwent an exploratory laparotomy for palliation. The operative findings were a 30-cm left ovarian mass, a 10-cm right ovarian mass, a 6-cm left pelvic side wall mass, a 10-cm mass adherent to the posterior uterine wall, a 3-cm omental nodule with mucinous cystic membranous material, and a 5-cm umbilical mass. No disease was noted on the surface of the liver. There were no clinically enlarged or suspicious retroperitoneal lymph nodes. Resection of all macroscopic disease, including resection of the umbilicus, was performed. The patient's intraoperative and postoperative course was unremarkable.
Histopathology of the left ovarian mass showed the presence of an ovarian fibroma (Fig. 1). The right ovarian cyst, umbilical, omental, and other peritoneal nodules all contained hydatid disease. There was no evidence of malignancy.
This patient was treated with a course of 400 mg of albendazole twice daily for the first postsurgical month, followed by 100 mg three times daily for 3 months. Her pleural effusion resolved without further intervention. The postoperative hydatid enzyme-linked immunoassay (ELISA) results were equivocal.
Results
At a 6-month follow-up abdominal ultrasound scan of this patient, there was no evidence of disease recurrence and her calcified liver lesion had reduced in size.
Discussion
Cystic echinococcosis is an anthrozoonosis caused by the larval form of tapeworm genus Echinococcus, most commonly Echinococcus granulosus. Dogs and canids are the definitive hosts, which harbor the adult stage of the worm in their small intestines. Eggs released by the gravid proglottids are passed out in the feces and ingested by the intermediate hosts (sheep, cattle, horses, goats). Humans are the accidental intermediate hosts. Transmission occurs by consumption of contaminated water or food, or by contact with infected animals.
Incidence and sites of disease
The incidence of pelvic hydatidosis is 0.2%–0.9%.3,4 Hydatid disease is endemic in Mediterranean, the Middle and Far East, and South America, but travel and migration has facilitated global distribution. 5 The most common organs involved in hydatid disease are the liver (55%–60%) followed by the lungs (30%). Unusual sites of hydatidosis are the kidneys, heart, bones, omentum, ovaries, pelvis, muscles, brain, and spleen. 6 Intraperitoneal hydatid disease develops secondary to spontaneous or iatrogenic rupture of hepatic, splenic, or mesenteric cysts. Rarely, a primary pelvic hydatid cyst may develop without evidence of cysts in any other intra-abdominal organs. 7 In the current case, disseminated abdomino-pelvic hydatid disease may have occurred because of a rupture of a liver hydatid cyst.
Symptoms and signs
Presenting symptoms of echinococcosis are nonspecific and depend on the site involved, the size of the cyst and the parasite load, complications related to cyst rupture, and systemic host reactions. 8 Abdominal pain, swelling, menstrual irregularity, infertility, and pressure symptoms have all been reported. The cyst fluid is highly antigenic, and rupture of the cyst can rarely present as anaphylactic shock. Disseminated intraperitoneal disease can mimic abdominal or ovarian malignancy. Spread to the lungs can occur via a transdiaphragmatic or hematogenous route. Large pulmonary cysts can shift the mediastinum, induce a pleural reaction, or cause atelectasis of adjacent lung parenchyma. 9 Hydatid lung abscess, pleural effusion, and empyema have also been noted. Pulmonary hydatid disease affects the right lung in ∼60% of cases.
Structure of a hydatid cyst
A typical hydatid cyst has three layers of which the outermost one is the fibrous pericyst formed in response to the inflammation induced in the host by the parasite. 10 This layer is thick in liver and spleen hydatid cysts, can be thin in peritoneal cysts, and is absent in lung and brain cysts. Calcification of a pericyst can occur over time and, once complete, calcification can cut off the nutrient and oxygen supply to the parasites making the cyst nonviable. The parasite itself has an ectocyst and an endocyst. The ectocyst comprises an elastic laminated membrane (Fig. 2) made up of gelatinous chitinous material that curls in on itself when incised or ruptured, thus exposing the inner germinal layer. The endocyst or the germinal layer is the cellular viable layer of the cyst, which produces brood capsules with scolices, secretes hydatid fluid, and forms the outer layer. Figures 1–3 show examples of hydatid cystic formations and the ovarian fibroma.

Peritoneal hydatid cyst with concentric laminations.

Hysterectomy specimen with adherent hydatid cysts.
Diagnosis and classification systems
A diagnosis of hydatid disase can be made by imaging and/or serologic tests. However, confirmation of infection requires histopathologic asessment. Ultrasound is a useful, inexpensive initial diagnostic tool, while contrast-enhanced CT scanning can provide detailed cyst morphology.
Various classification systems have been proposed for hydatid cysts, based on their ultrasonographic appearances and clinical courses. The two most widely used systems are those proposed by Gharbi et al. in 1981 11 and the WHO-IWGE [World Health Organisation–Informal Working Group on Echinococcosis] in 2001. 12 These are described (including pathognomonic signs) and then compared in Tables 1, 2 and 3.
WHO-IWGE, World Health Organisation—Informal Working Group on Echinococcosis.
WHO-IWGE, World Health Organisation—Informal Working Group on Echinococcosis.
The WHO-IGWE classification allows standardization and takes clinical information into account, thus allowing stage-specific treatment options to be tested in prospective trials. CE1 and CE2 are considered to be active cysts (that are usually fertile), CE3 represents transitional cysts (that starting to degenerate but still contain viable protoscoleces), and CE4 and CE5 are considered to be inactive cysts (that are degenerate or partially or totally calcified cysts).
Serologic tests can contribute to diagnosis mainly in hepatic hydatid disease. Immunoglobulin G detection by ELISA has a sensitivity of 95% and a specificity of 94%. The sensitivity of the indirect hemagglutination test has been found to be 87.5%. 13 However, serology testing may not be as useful for detecting extrahepatic disease. 14
Despite advances in radiologic and serologic techniques, histologic assessment of tissue biopsy or resection specimens remains the “gold standard” diagnostic test for hydatid disease. In the current case, the left ovarian tumor was confirmed to be a fibroma, with no evidence of active hydatid scoleces. All of the other masses had identifiable features of hydatid disease with viable scoleces. Differentiating an ovarian fibroma from a type V/type CE5 hydatid cyst on clinical or histologic assessment remains very difficult. In the current case, it is likely that the pleural and peritoneal effusions noted clinically could have been be part of Meig's syndrome, a known complication of large ovarian fibromas, and this complicated the clinical picture significantly. The pleural effusion in this case could also be explained by hydatid lung disease, which occurs more commonly on the right side.
Treatment
Surgery is the mainstay of treatment especially for intraperitoneal and abdominopelvic hydatid disease. 15 The surgical goals are complete removal of the cyst, preventing further contamination, and to preserve as much parenchyma as possible in case there is solid organ involvement. To prevent further dissemination, the operative field should be packed with sponges soaked in a scolicidal solution such as sodium chloride. In the current case, because of the suspicion of malignancy and the extensive involvement of the ovaries, uterus, omentum, pelvic side wall, and umbilicus, complete radical resection was undertaken without any spillage.
Other nonsurgical management options include systemic medical treatment with mebendazole or albendazole and PAIR treatment (this is defined below). Use of medical treatment is recommended as preoperative adjuncts in cases when hydatid disease is suspected or postoperatively to prevent recurrences after surgery.16,17 PAIR is a minimally invasive technique that is useful for selected cases when surgery is contraindicated or refused and for cases in which there is relapse after surgery. The treatment involves
This case also emphasizes the important clinical decision to avoid neoadjuvant chemotherapy in the absence of cytologic/ histologic evidence of malignancy despite suspicious imaging, a raised CA 125 level, and a clinical picture that appeared to be highly suggestive of advanced ovarian malignancy.
Conclusions
The focus of health care in countries with aging populations is the management of malignant disease, and there is a presumption that patients referred to gynecologic-oncology services will typically have malignant disease. However, in an age where transcontinental migration is increasing, nonendemic diseases also need to be considered in differential diagnosis, and eliciting a history of foreign travel is essential for directing investigations that are likely to establish the correct diagnosis. Finally, this highly unusual case highlights the need for histologic and/or cytologic confirmation of malignancy before considering neoadjuvant treatment for suspected malignancy.
Footnotes
Disclosure Statement
No conflicts of interest for all the authors with regard to the submitted manuscript.