
Abstract
Abstract
Introduction
L
RV, rectovaginal.
Methods
A literature review was conducted. A Medline search was used, using the terms Vaginal diseases, Vaginal neoplasms, Rectal diseases, and Rectal neoplasms.
Results
Reported lesions of the rectovaginal septum were reviewed. Many of these lesions can be mistaken for each other clinically.
Discussion
Anatomy and histology
The rectovaginal septum (rectovaginal fascia) is thought to derive from the urogenital sinus/vaginal plate and is predominantly composed of fibroconnective tissue containing nerves and vessels (Fig. 1). The smooth muscle tissue present in this region is actually derived from the ventral rectum, 1 and elastic tissue and vessels are present as well. 2 Damage to the rectovaginal septum can lead to rectoceles, incontinence, and constipation. 1 The histology differs between the lower and upper portions. 2 Nagata et al. 2 studied elderly Japanese female cadavers and found that the rectovaginal interface was tight in the lower half and loose in the upper half. This looseness in the upper portion may impact on high rectocele or enterocele repair by providing minimal anchoring tissue to utilize in the repair. The authors also noted a variation among patients in the tissue components, suggesting individualization of repairs.
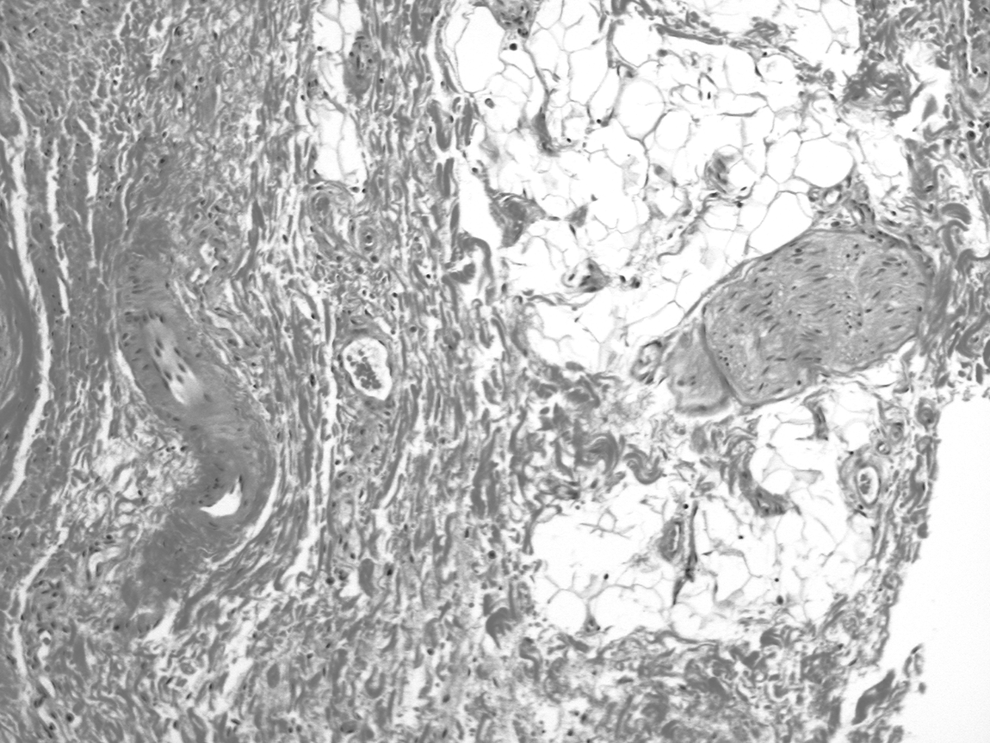
Rectovaginal septum composed of fibroconnective tissue (left) and adipose tissue (right). A nerve is seen at 3 o'clock.
Congenital anomalies
Although most cases of rectovaginal fistulas are acquired, congenital fistulas may occur often in association with other anomalies in the region, such as rectosigmoid duplication. 3
A case of a villous adenoma that extended in continuity from the rectum through the rectovaginal septum and into the vaginal mucosa has been reported, and the authors postulated that this circumstance is best explained by an underlying congenital malformation where there was a communication through the rectovaginal septum. 4
Infections and inflammations
Although usually lateral in location due to their embryologic distribution, Gartner's duct cysts derived from Wolffian duct remnants may present in the posterior vaginal wall, where they have been described in association with rectovaginal septal abscess formation. 5 A rare case of echinococcosis has been described in the rectovaginal septum as an extremely rare etiology of a rectovaginal fistula. 6 Abscesses may also derive from infected cryptoglandular cysts of the distal gastrointestinal tract.
Rectovaginal fistulas
The most common etiologies for rectovaginal fistulas are prior obstetrical trauma and Crohn's disease. 7 Fistulas may also develop postoperatively after surgery for malignancy or endometriosis due to devitalization of tissue. Although not always present, the finding of granulomatous inflammation is supportive of a diagnosis of Crohn's disease (Fig. 2). Fistulas may also develop secondary to intercourse, although this is much more likely with assault than consensual intercourse.
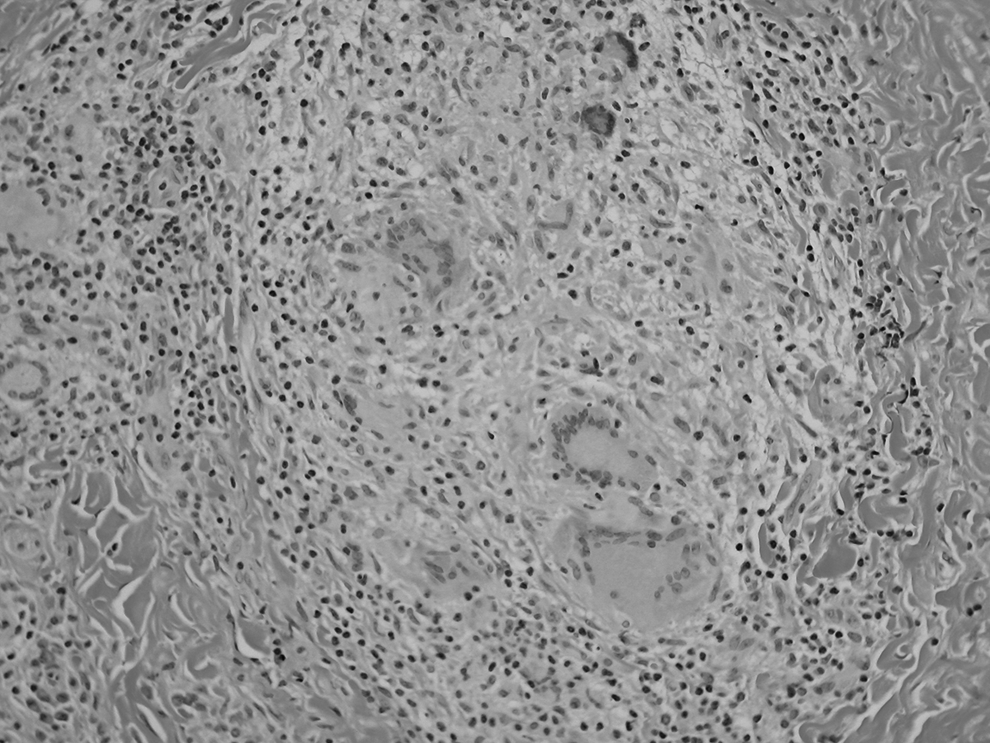
Granuloma with multinucleated giant cells in a patient with Crohn's disease.
Benign tumors and tumor-like lesions
Cysts
A variety of cysts may affect the rectovaginal septum, including endometriotic cysts and dermoid cysts. Inclusion cysts may arise from the posterior vaginal mucosa. This is not unexpected, as trauma is thought to be a contributor to the development of these cysts, and a history of episiotomy may be present. In one case, a squamous cell carcinoma of the vagina extending into the rectovaginal septum arose in one of these squamous inclusion cysts. 8
Iatrogenic
Postoperative traumatic neuromas can be the cause of severe pain. A debilitating rectovaginal neuroma arising after a total vaginal hysterectomy and posterior colporrhaphy was described in a 32-year-old female, whose pain resolved after excision of the neuroma. 9
Endometriosis
The rectovaginal septum is a common location for deep endometriosis, potentially causing severe pain, and dyspareunia. It is often associated with fibrosis as well as proliferation of smooth muscle, 10 and hence may present as a mass. Exceptionally rare rectal obstruction has been reported. 10 Histologically, endometriosis, as elsewhere, is characterized by the presence of endometrial glandular epithelium and stroma. In the rectovaginal septum, this may be accompanied by smooth muscle proliferation, sometimes nodular, leading some investigators to suggest that this type of deep endometriosis is more appropriately termed adenomyosis, although this and the existence of adenomyomas is debated.11,12 Rarely, this type of endometriosis may be associated with subsequently developing rectal injury with an intact perineum during childbirth, possibly due to loss of elasticity from the endometriosis. 13
It is well recognized that adenocarcinomas may arise in endometriosis and while this is most commonly in the ovary, the second most common site and most common extraovarian site is the rectovaginal septum. 14 Histology may be papillary serous, endometrioid, or clear-cell adenocarcinoma, 14 consistent with Müllerian origin.
Benign mesenchymal neoplasms
A variety of benign mesenchymal masses have been described arising in the rectovaginal septum, including fibromas, leiomyomas, adenomyomas, neurofibroma, fibromyoma, teratoma, lipoma, and schwannoma.5,15 Such masses may be asymptomatic, or symptoms may be nonspecific, with impingement on adjacent organs such as the bowel or bladder. An unusual case of a rectovaginal leiomyoma presenting as a posterior vaginal wall prolapse was described. 15 A case of gliomatosis peritonei involving the rectovaginal septum of an adolescent has been reported. 16 This case was, in addition, unusual for occurring in association with a prior recurrent benign teratoma rather than an immature teratoma, the more usual association.
Malignant neoplasms
Carcinoma
Usual colorectal carcinomas may present as rectovaginal masses. In one unusual case, adenocarcinoma of colonic origin arose in a rectovaginal fistula in a setting of chronic Crohn's disease. 17 Immunohistochemistry is helpful in distinguishing adenocarcinomas of colonic origin from those of Müllerian origin.
Most primary malignancy arising in the RV septum is adenocarcinoma in association with endometriosis, and primary de novo Müllerian-derived carcinoma is very rare.18,19 Sampson's criteria 20 for attributing a neoplasm to endometriosis include that the neoplasm must be of compatible histologic origin, there must be no other primary, and endometriosis has to be present adjacent to the tumor. In many cases, it is possible that the neoplasm overruns adjacent endometriosis, obscuring it. Among theories for de novo carcinoma is the Müllerian rest origin.18,21 Neoplasms of the RV septum can present with rectal or vaginal bleeding, acute urinary retention or other urinary symptomatology, 18 and abdominal pain or dyspareunia. 21 Nelson et al. 18 presented a case in a 47-year-old woman who was initially diagnosed as having a uterine prolapse. The histology was consistent with papillary serous carcinoma. Adenocarcinoma with squamous and clear-cell differentiation has also been reported. 21 These Müllerian carcinomas may also be of endometrioid histology, clear-cell adenocarcinoma, or even possible adenosarcomas or carcinosarcomas, and may present with symptoms attributed to colon cancer, such as rectal bleeding, abdominal pain, and/or constipation. A case of atypical proliferating (borderline) endometrioid tumor was also described in the rectovaginal septum, where the tumor was thought to arise due to many years of unopposed estrogen therapy leading to malignant degeneration of endometriosis. Of interest, this lesion was androgen producing. 22 Due to the differences in therapy between these Müllerian tumors and primary colorectal cancer, it is important to be aware of this diagnosis.19,23 At least some of the adenocarcinomas arising in the rectovaginal septum appear to be less aggressive than the ovarian counterparts. 24
Secondary carcinomas may also extend through the rectovaginal septum, such as squamous cell carcinoma of the cervix (Fig. 3), vaginal carcinoma, rectal adenocarcinoma, or urachal carcinoma (Fig. 4). A rectovaginal septal metastasis may be the first sign of an unexpected neoplasm, such as the fallopian tube cancer described by Asai-Sato et al. 25 The lesion was grossly unapparent in the fimbria, documented histologically, and showed matching p53 mutational analysis with the rectovaginal tumor.
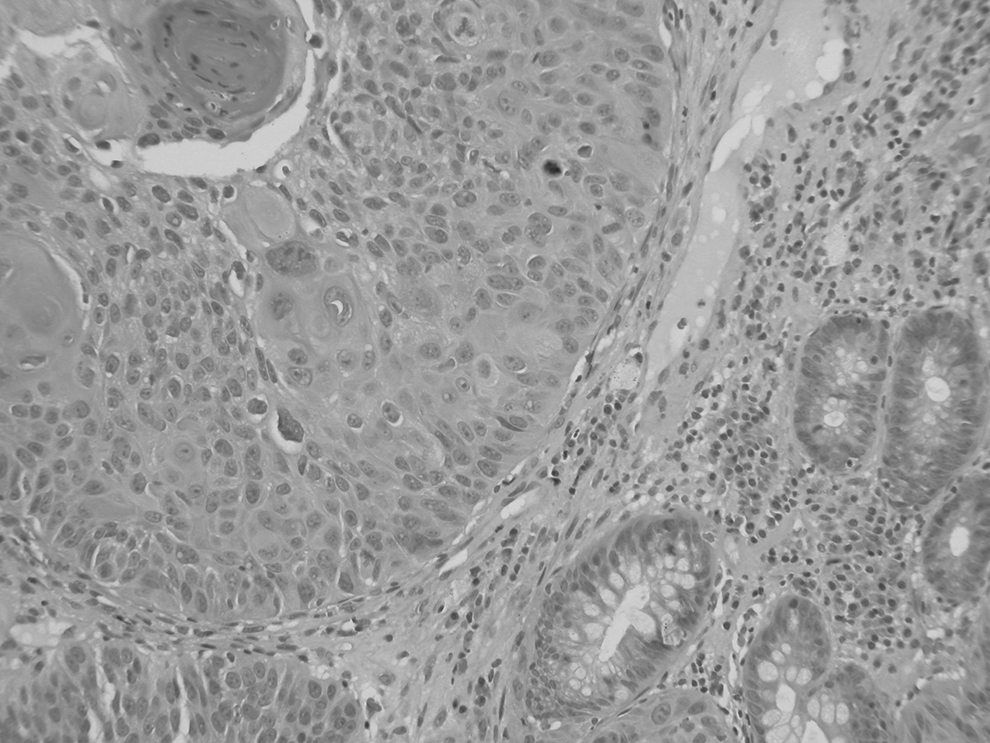
Cervical squamous cell carcinoma, which had eroded through the rectovaginal septum, is here seen adjacent to rectal glands.
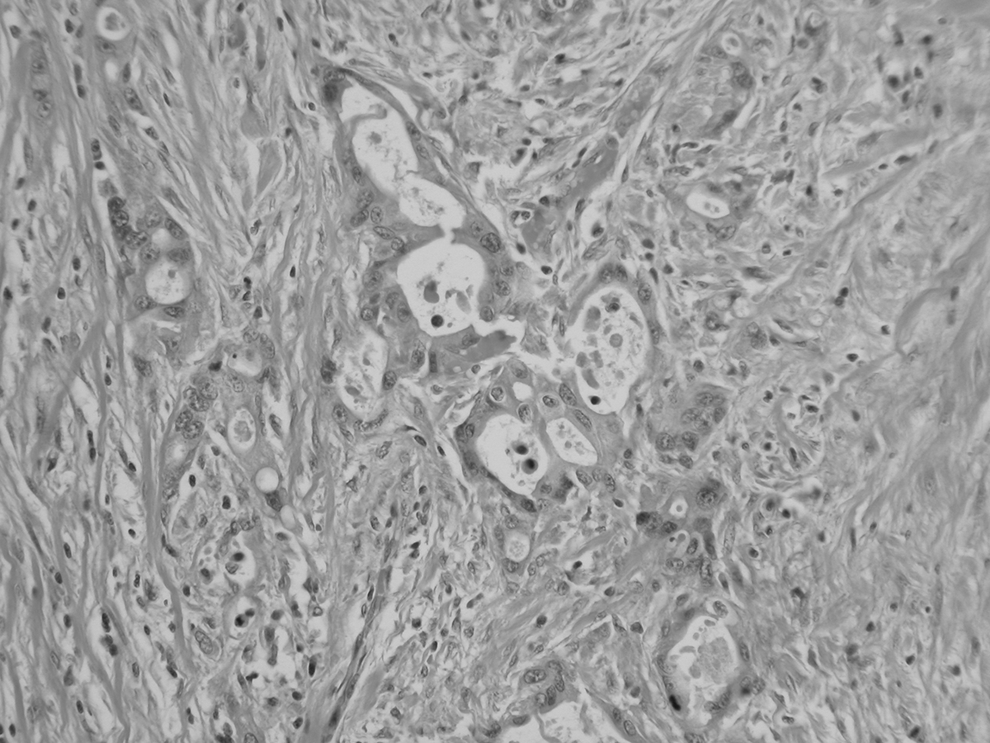
Urachal adenocarcinoma, which infiltrates the rectovaginal septum.
Sarcoma
Because the rectovaginal septum is composed of mesenchymal tissue, a wide variety of unexpected soft tissue neoplasms may rarely occur. A case of leiomyosarcoma arising in the rectovaginal septum has been reported. 26 The patient was 70 years old and succumbed to her disease, which obstructed her urinary tract and eroded into the posterior vagina.
Extragastrointestinal stromal tumors (eGISTs) have rarely been described in the rectovaginal septum. These tumors most commonly arise in the stomach and are thought to originate from the interstitial cells of Cajal. 27 They may behave in a benign or malignant manner, but have recurred locally frequently when arising in extragastrointestinal locations. 27 Tumor size, mitotic rate, cellularity, necrosis, and Kit mutations have been utilized as prognostic factors for GISTs, but prognostic data for eGISTs are less clear.27,28 Most cases present in midlife patients. Grossly, they are similar to leiomyomata, presenting as masses in the rectovaginal septum. Masses may be asymptomatic or impact on urinary and bowel function, with possible urinary frequency and/or constipation. 27 The similarity extends to microscopy, where the lesion is composed of spindle cells in fascicles, and hence, an eGIST needs to be considered. Immunohistochemistry will distinguish the two lesions; leiomyomata stain for smooth muscle markers, while GISTs stain for CD 117(c-kit) and CD 34.
Aggressive angiomyxoma, usually described as a vulvar tumor with a potential for pelvic extension and locally aggressive behavior, can present in the rectovaginal septum. 29
Rare malignancies
A case of extraosseous Ewing's sarcoma was reported in a 45-year-old patient, who refused surgery after chemotherapy. 30 A case of rectovaginal mesothelioma was reported in a woman with a history of asbestos and beryllium exposure, and it was felt that the location of the neoplasm related to implantation during an obstetrical injury, as beryllium was identified in the neoplasm as well as in water the patient douched with to treat her obstetrical lacerations. 31
Conclusions
The rectovaginal septum may rarely be found to contain a mass. Knowledge of specific lesions of the region will be helpful if such a patient is encountered.
Footnotes
Disclosure Statement
No competing financial interests exist.