
Abstract
Abstract
Introduction
H
Reduction in the future risk of ovarian cancer is the single most common reason for normal ovaries to be removed during a hysterectomy. As a result of poor screening tools and delay in diagnosis, there has been little improvement in the overall prognosis of patients with ovarian cancer in past 2 decades. Between 4% and 14% of women who developed ovarian cancer had prior hysterectomies in which the ovaries were retained. 10
The postmenopausal ovary has been regarded as a source of sex steroids, especially androgens, which are assumed to play important roles in physiologic, psychologic, and sexual well-being. However, an article in 2005 stated that androgen values over the lives of females are compatible with a U-shaped distribution, in which androgen decline starts in the early reproductive years, flattens out in middle life, and then has a small rise in later years. 11
Couzinet et al. refuted the role of the postmenopausal ovary as a site of significant androgen production and suggested that androgen in these females originate from the adrenal glands. 12 Above all, even if ovaries are conserved during hysterectomy, the risk of surgical menopause remains.
Currently, there are three main routes of hysterectomy, namely, abdominal, vaginal, and laparoscopic. Vaginal hysterectomy has the shortest operating time (66–84 minutes), rapid recovery, lower cost, and no detectable differences in quality of life thereafter. 13 However, perceived inaccessibility to the ovaries vaginally, risk of ureteral injury, and incomplete removal of ovarian tissue are the concerns noted in the literature about vaginal salpingo-oophorectomy. Studies have shown that it is possible to remove the ovaries completely by the vaginal route in 92%–97.5% of cases.4,14–17
In cases when it becomes impossible to perform vaginal salpingo-oophorectomy, laparoscopic assistance can be used. Laparoscopic oophorectomy with vaginal hysterectomy has an acceptable operating time (85 minutes), low intraoperative and postoperative complications, and the advantage of abdominopelvic exploration, and is suitable for larger uteri and those with little or no descent, which may prove difficult to remove vaginally.17,18 However laparoscopic oophorectomy's role in vaginal hysterectomy with salpingo-oophorectomy is very small. Thus, the present study was designed to compare the two routes of oophorectomy with vaginal hysterectomy, namely laparoscopic and vaginal.
Materials and Methods
This was a prospective, randomized open-label study conducted in the Department of Obstetrics and Gynecology at the University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi, India, from October 2011 to April 2013.
The study protocol was explained to the subjects and informed consent was obtained from them. Ethical approval was obtained from the institutional ethical committee.
Considering the variability of mean duration of 34.6 minutes and 27.9 minutes for vaginal hysterectomy with vaginal salpingo-oophorectomy and laparoscopic oophorectomy with vaginal hysterectomy, respectively, a power of 80%, and a significance level of 5%, to study a difference of 30 minutes, a total of 42 women were scheduled to undergo vaginal hysterectomy were enrolled in the study and assigned to 2 groups: laparoscopic oophorectomy with vaginal hysterectomy (group 1) and vaginal hysterectomy with vaginal oophorectomy (group 2), using a computer-generated random number table. A detailed history was obtained, and a careful clinical examination, investigations for operative fitness, and ruling out of underlying malignancy was performed for each patient. All of the women underwent same standard preoperative preparation, and all procedures were performed under general anesthesia. Inclusion criteria were woman with benign uterine pathology, and age >50 years or age <50 with high risk for ovarian malignancies (e.g., family history, high risk for breast cancer or other familial cancers. Exclusion criteria were women with contraindications to vaginal hysterectomy or laparoscopy, with suspected or confirmed malignant diseases or uterine size >14 weeks of gestation.
In the laparoscopic group, after insertion of the laparoscope, complete inspections of pelvis and abdomen were performed. For each patient, the first step was localization of a ureter, which was traced from the pelvic brim downward. Thereafter, the round ligament was identified, cauterized with a bipolar or harmonic scalpel and transected (Fig. 1). The infundibulopelvic ligament with ovarian vessels was isolated, cauterized, and severed (Figs. 2 and 3). Hysterectomy was then begun vaginally and completed. After completion of the hysterectomy, laparoscopic inspection of the pelvis was performed to confirm hemostasis.
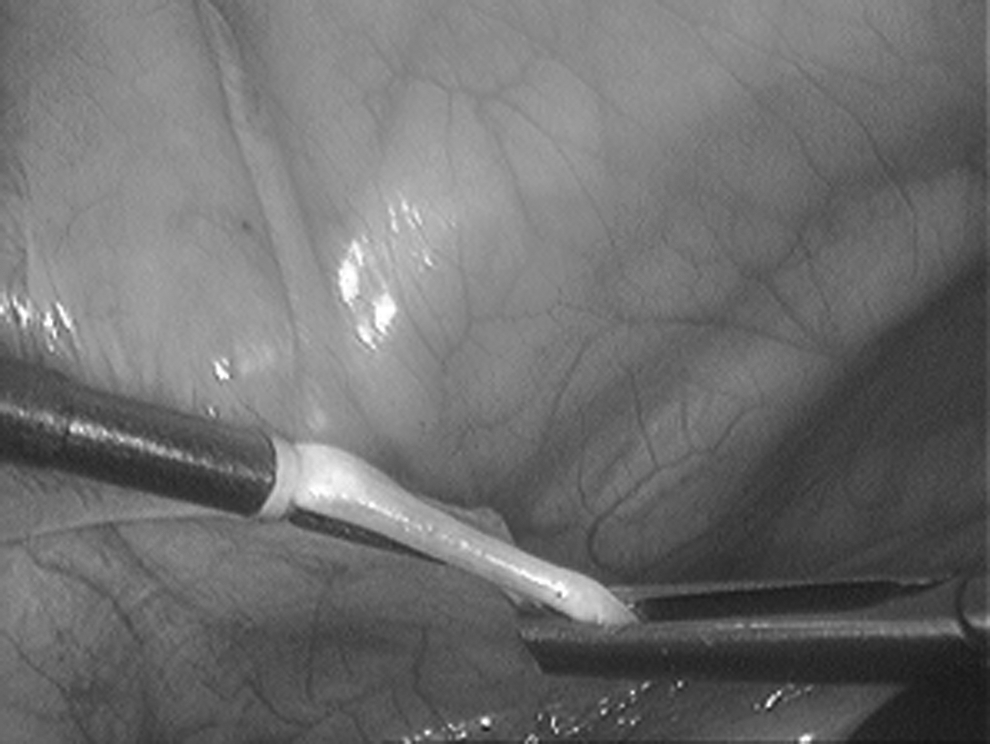
Ligation of round ligament.

Coagulation of infundibulopelvic ligament.

Transecting infundibulopelvic ligament with bipolar scissors.
In the vaginal group, the usual steps of vaginal hysterectomy were carried out for each patient until bilateral ligation of the uterine arteries. This was followed by the complete bisection of the uterus up to the fundus. Then, one-half of the bisected uterus was repositioned in the peritoneal cavity, and the other half was drawn down and medially to visualize the round ligament. The round ligament was then ligated and cut as laterally as possible for easier access to the infundibulopelvic ligament. With adequate exposure and traction, the infundibulopelvic ligament was cut and ligated, and the ipsilateral tube with an ovary and the bisected half of the uterus were delivered. The same procedure was carried out on the other side and the contralateral tube and ovary were then removed. This technique of bilateral salpingo-oophorectomy after uterine bisection, isolating round ligaments and clamping infundibulopelvic ligaments, was developed by the second author (Shalini Rajaram, MD, MAMS) and is called Rajaram's technique of vaginal bilateral salpingo-oophorectomy.
Sheth, using his own technique of bilateral oophorectomy, has performed salpingo-oophorectomy on one side with oophorectomy on the other side. 18 However with the current evidence, it is was decided to remove bilateral salpinges as some ovarian cancers arise from the fimbrial end of the fallopian tube.
The primary outcome measure was total operating time, which was calculated from abdominal skin or vaginal incision to closure. The time of laparoscopic oophorectomy was calculated from abdominal skin incision to transection of infundibulopelvic ligament and round ligament. For vaginal oophorectomy, operating time was calculated from completion of fundal bisection to transection of round and infundibulopelvic ligament and delivery of tubes and ovaries. The secondary outcome measures were blood loss (measuring blood volume in a suction bottle and by weighing standardized mops or swabs); need for blood transfusion; conversion rate (laparoscopy converted to laparotomy and vaginal oophorectomy to laparoscopic oophorectomy); technical difficulty during the procedure according to subjective rating by the surgeons as “easy,” “difficult,” and “very difficult”; intraoperative complications; postoperative pain (assessed at 15 minutes, 30 minutes, 1 hour, 2 hours, 6 hours, after 24 hours, 48, hours, and at 72 hours by visual analogue scale [VAS]); duration of first rescue analgesics (intramuscular diclofenac in mg/kg at VAS ≥3), intake of total analgesics in 72 hours; return of bowel sounds (hours); postoperative complications; need for reoperation; discharge time (days), and late postoperative complications within 6 weeks.
Statistical analysis was performed, using the statistical program SPSS for Windows. Continuous outcome variables were analyzed using an unpaired Student's t-test. VAS score was analyzed using a repeated measure analysis of variance test followed by a posthoc Tukey's test. Discrete variables were analyzed using a χ2 test or Fisher's exact test. A p-value <0.05 with a confidence interval (CI) of 95 % was considered statistically significant.
Results
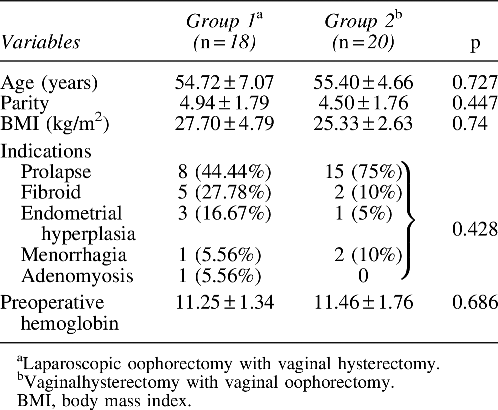
The two groups were matched with respect to age, parity, body mass index (BMI), religion, residence, socioeconomic status, preoperative hemoglobin, and indications for surgery (Table 1). The mean ages of the women were 54.72 ± 7.07 and 55.40 ± 4.66 years (p = 0.727), and the mean parities were 4.94 ± 1.798 and 4.50 ± 1.762 (p = 0.447) in groups 1 and 2, respectively. The mean BMI of the women was 26.45 kg/m2 in both groups. The mean preoperative hemoglobin levels for groups 1 and 2 were 11.25 ± 1.34 g/dL and 11.46 ± 1.76 g/dL, respectively (p = 0.686).
The total operating time (oophorectomy and hysterectomy) for group 1 was 85.53 ± 17.572 minutes (95% CI: 76.64–93.38) and for group 2 was 70.00 ± 13.650 minutes (95% CI: 64.01–75.98), which was found to be significantly different between the two groups, with p = 0.005. A statistically significant difference was seen in the mean operating time for oophorectomy, 37.06 ± 10.16 minutes (95% CI: 32.36 to 41.75) and 20.75 ± 5.56 minutes (95% CI: 18.31 to 23.18), p = 0.001, while no significant difference was found in mean operating time of vaginal hysterectomy in both groups, 48.06 ± 10.709 minutes (95% CI: 42.96–53.15) versus 49.25 ± 11.318 minutes (95% CI: 44.28–54.21), p = 0.746.
There was no statistically significant difference in blood loss, need for blood transfusion, technical difficulty, intraoperative or postoperative complications, postoperative pain, need for rescue analgesics, return of bowel sounds, and discharge time (Table 2 and Fig. 4) in both groups. The mean blood loss was 383.89 ± 39.26 mL (range: 150–1200) and 408.25 ± 186.923 mL (range: 120–800), p = 0.727, and blood transfusion was required in 6 women (33.33%) in group 1 and in 8 women (40.00%) in group 2, respectively (p = 0.671). The mean time for first rescue analgesic was 4.06 ± 0.86 hours (range: 2.75–6.00) in group 1 and 4.51 ± 1.27 hours (range: 3–8) in group 2, p = 0.224.

Visual analogue scores of the two groups (group 1, laparoscopic oophorectomy with vaginal hysterectomy; group 2, vaginal hysterectomy with vaginal oophorectomy). min, minutes; hr, hour.
Laparoscopic oophorectomy with vaginal hysterectomy.
Vaginal hysterectomy with vaginal oophorectomy.
VAS, visual analogue scale; min, minutes; hr, hour.
Mean intake of total analgesics for 72 hours in group 1 was 575.67 ± 53.381 mg (range: 490–660) and 535 ± 57.417 mg (range: 480–700) in group 2, p = 0.309. The mean duration of return of bowel activity was 5.05 ± 0.72 hours (range: 4–7) in group 1 and 5.30 ± 0.78 hours (range: 4–6) in group 2, p = 0.327. The mean time to discharge was 3.815 ± 1.07 days (range: 3–5) and 4.06 ± 2.54 days (range: 3–15) in groups 1 and 2 respectively, p = 0.425. The patients were discharged only after they were comfortable, passed stools and urine, and resumed full diets.
The level of technical difficulty was found to be similar between the two groups (p = 1.00). There were 2 cases of intraoperative complications in the laparoscopic group, in which ovarian vessels were injured and continued to bleed despite the use of cautery, necessitating conversion to laparotomy. No intraoperative complications were recorded in the vaginal group except conversion to laparoscopy in 3 cases in which infundibulopelvic ligaments were not accessible vaginally. In the postoperative period, 3 women (n = 1 in group 1 and n = 2 in group 2) had postoperative nausea and 3 had urinary tract infections (n = 1 in group 1 and n = 2 in group 2). Postoperative fever was noted in 2 women in the vaginal group. None of the cases required reoperation. Several of outcomes are detailed in the Discussion section and compared with examples from the literature.
Discussion
The aim of the present study was to compare the intra- and postoperative outcomes of laparoscopic oophorectomy and vaginal oophorectomy during vaginal hysterectomy. A demographic profile revealed that the majority of women in both groups were ages 50–60, and parity ranged from 2 to 8, which is in alignment with the age distribution of women as reported in previous studies.15,19,20 The total operating time was found to be longer for a laparoscopic group than a vaginal group, at 85.53 ± 17.57 minutes (95% CI: 76.64–93.38) versus 70.00 ± 13.650 minutes (95% CI: 64.01–75.98), p = 0.005. There was no significant difference in operating time for hysterectomy in both groups, which was 48.06 ± 10.709 minutes (95% CI: 42.96–53.15) for group 1 and 49.25 ± 11.318 minutes (95% CI: 44.28–54.21) for group 2, p = 0.746. It indicates that the difference in total operating time was because of the time taken for oophorectomy, which was longer for laparoscopic oophorectomy at 37.06 ± 10.16 minutes (95% CI: 32.36–41.75) and 20.75 ± 5.56 minutes (CI: 18.31–23.18), in groups 1 and 2, respectively (p = 0.001).
Sizzi et al. also reported the operating time for a laparoscopic group to be considerably longer (125 ± 21.3 in group 1 and 83.6 ± 38.28 minutes in group 2, p = 0.01), while Agostini et al. found no significant difference (100 ± 27.9 minutes in group 1 and 83.9 ± 34.6 minutes in group 2, p = 0.08);15,19 However few studies have compared the time of oophorectomy alone in both groups. Sheth found that time taken to perform additional surgery for oophorectomy by vaginal route varied from 7 to 35 minutes with an average of 14 minutes, while, according to Sizzi et al., it varied from 10 to 30 minutes (mean 21.41) in both groups.15,18
Blood loss was not found to be significantly different between groups nor was the need for blood transfusion. Sesti et al. reported blood loss to be higher in a laparoscopic group, compared to a vaginal group. 20 Similarly Agostini et al. reported a significant difference between blood loss and rates of transfusion between two groups, in which a blood loss >500 mL was more common in a laparoscopy group (p = 0.39). 19 The mean fall in hemoglobin levels, compared to preoperative hemoglobin levels was similar between the two groups in the current study at 0.994 ± 0.54 g/dL versus 1.01 ± 0.54 g/dL in groups 1 and 2, respectively, p = 0.930.
In the current study, the level of technical difficulty was grouped as easy in 61.1% (n = 11), difficult in 27.8% (n = 5), and very difficult in 11.1% (n = 2) of women. In the laparoscopic group, it was easy in 55.5% (n = 11), difficult in 30.0% (n = 6), and very difficult in 15% (n = 3) of women in the vaginal group (p = 1.00). Although laparoscopic procedures are considered technically challenging, no previous researchers have actually compared the level of technical difficulty between laparoscopic and vaginal route of oophorectomy. 21 Conversion of laparoscopy to laparotomy occurred in 11.1% (n = 2) and vaginal oophorectomy to laparoscopic oophorectomy in 15% (n = 3) of the women (p = 1.00).
In the current study, the mean weight of the uteri was similar between the two groups (79.17 ± 29.36 g, ranging from 50 g to 150 g in group 1, versus 68.00 ± 23.41, ranging from 30 g 130 g for group 2, p = 0.201). The mean uterine weight in previous studies was higher (mean >200 g) because of differences in the frequency of indications for hysterectomy. In a study by Drahonovsky et al., the majority of the patients were operated for uterine myoma with or without menorrhagia (75.2%, n = 94/125), while, in Agostini et al., indications were fibroids in 70.8% (n = 34/48) and adenomyosis in 29.16% (n = 14/48), matched for both study groups.13,19 Sesti et al. had only included patients with symptomatic myoma with uterine sizes >12 weeks of gestation. 20
Early postoperative complications were minimal in both groups. Sesti et al. also reported no significant differences in the rate of intra and postoperative complications between two groups (p = not significant [NS]). 20 In the present study, the mean duration of return of bowel activity was 5.05 ± 0.72 hours in the laparoscopic group and 5.30 ± 0.78 hours in the vaginal group, p = 0.327. Similarly, Sizzi et al. reported no significant differences in the rates of overall complications between 2 groups, 9% versus 9.9%, p = NS. 15 Agostini et al. reported overall postoperative complications to be higher in laparoscopic compared to a vaginal group. 19 There were 2 cases of trocar-site hematoma, 2 cases of vaginal cuff hematoma, and 1 case of postoperative fever in the laparoscopic group, while the vaginal group had 1 case of vaginal cuff hematoma and none of the other complications.
Postoperative pain assessment, using VAS scores, was similar between the two groups (p = 0.202). Sesti et al. compared postoperative pain in 2 groups at 24 hours and found that women who underwent laparoscopic-assisted vaginal hysterectomy complained of pain more frequently than women who underwent vaginal hysterectomy with vaginal oophorectomy (p = 0.01). 20 The mean duration to first rescue analgesic was 4.06 ± 0.86 hours (range: 2.75–6.00) in the laparoscopic group and 4.51 ± 1.27 hours (range: 3–8) in the vaginal group, p = 0.224. The mean intake of analgesic in 72 hours was also not different in the 2 groups, 575.67 ± 53.381 mg (range: 490–660) in group 1 and 535 ± 57.417 mg (range: 480–700) in group 2, (p = 0.309). Drahonovsky et al. reported the consumption of analgesic to be lower in the laparoscopic group, while Sesti et al. found that the laparoscopy group needed more analgesics than the vaginal group.13,22
The mean time to discharge was 3.815 ± 1.07 days (95% CI: 3.319–4.310) in group 1 and 4.06 ± 2.54 days (95% CI: 2.944–5.175) in group 2, p = 0.425. Agostini et al. reported a mean discharge time of 5.6 ± 1.14 and 5.5 ± 1.09 days (p = 0.76). 18 Likewise, Drahonovsky et al. reported similar a discharge time for 2 groups, 5.3 days (range: 3–14) versus 5.4 days (range: 3–10), p = NS. 13 Sesti et al. found the mean discharge time to be significantly longer in a laparoscopy group than in a vaginal group (72 ± 4.2 hours versus 48 ± 2.6 hours, p = 0.000) while Sizzi et al. reported the discharge time for a laparoscopy group to be shorter, compared to a vaginal group (2.1 versus 2.9 days, p < 0.01)15,22
Conclusions
Both vaginal and laparoscopic routes of oophorectomy can be used during vaginal hysterectomy. However, the vaginal route may be a better option, considering the shorter operating time and feasibility under regional anesthesia with a comparable surgical outcome to laparoscopy. In cases when vaginal hysterectomy with bilateral salpingo-oophorectomy cannot be completed because of highly placed ovaries laparoscopic oophorectomy can be performed.
Footnotes
Acknowledgments
This study was supported by the Guru Teg Bahadur Hospital, in Delhi, India.
Author Disclosure Statement
There were no commercial associations. There are no conflicts of interest.