
Abstract
Abstract
Introduction
H
Case
A 13-year-old adolescent, who had attained menarche 8 months prior, was referred to the current authors with a 5-month history of dysmenorrhea. She had been prescribed antispasmodics–analgesics intermittently, but she did not experience any relief from her symptoms. She complained of severe colicky pain in her lower abdomen during menstruation, along with a continuous dull, aching abdominal pain throughout the cycle. An abdominal examination revealed a slight tenderness in the lower abdomen. Her external genitalia were normal. Speculum and vaginal examination were not performed. Her routine hematologic and biochemical profiles were normal.
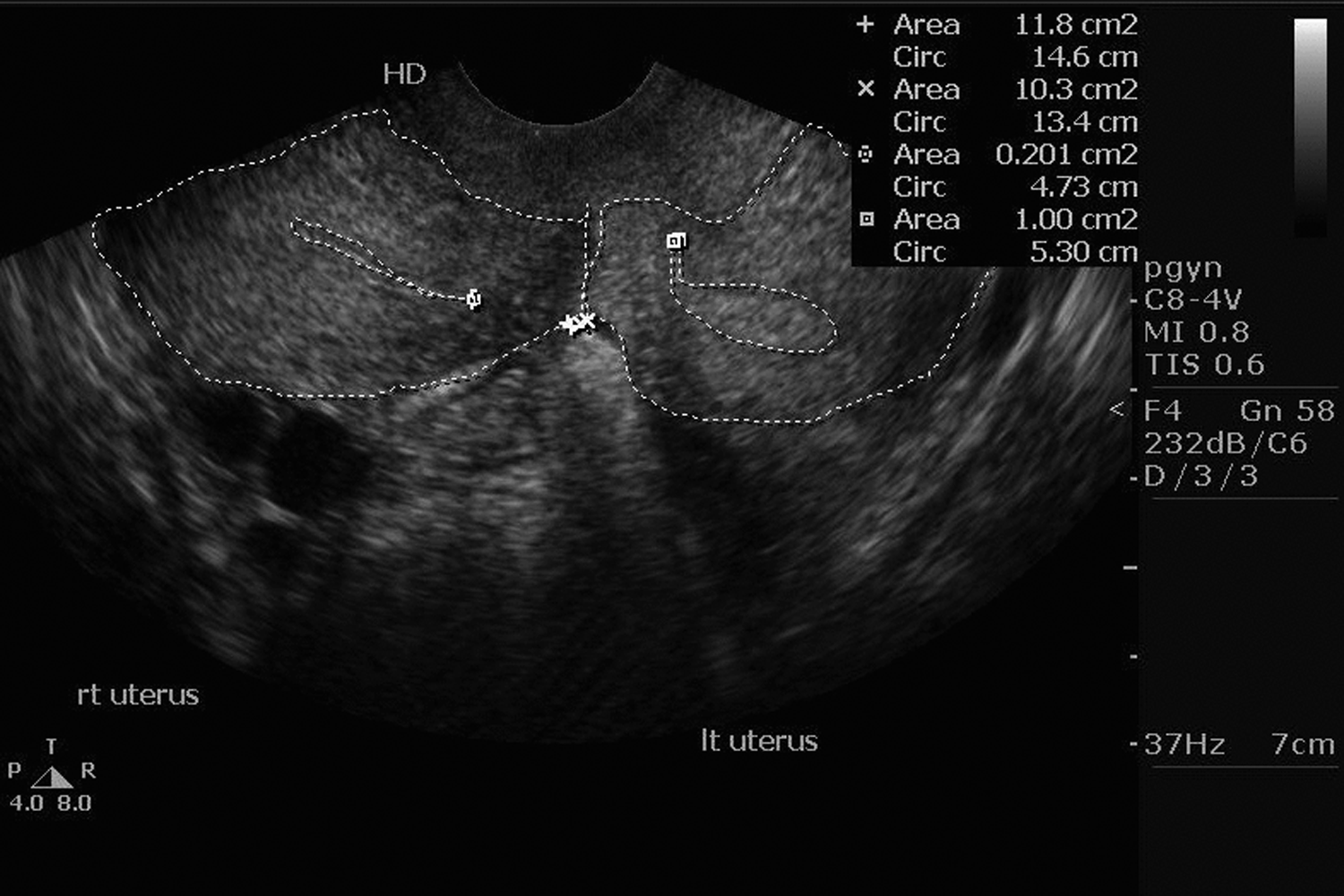
Ultrasonography of this patient's abdomen and pelvis revealed uterine didelphus with a double vagina with collection of fluid in the vagina and uterus on right side (Figs. 1 and 2). The left uterus and bilateral ovaries were normal in size and shape. The right kidney was absent, with a compensatory hypertrophy of the left kidney. This patient underwent an intravenous pyelography test, which confirmed the absence of right kidney (Fig. 3). For better delineation of the pathology, a further investigated was made via magnetic resonance imaging (MRI) of the pelvis. The MRI revealed the presence of uterine didelphys with a normal left-sided uterus, fallopian tube, and ovary. The right-sided uterus, fallopian tube, and vagina was distended with hyperintense fluid (suggestive of blood). This was suggestive of right hematometra, hematocolpos, and hematosalpinx probably caused by an obstructed right hemivagina (Fig. 4).
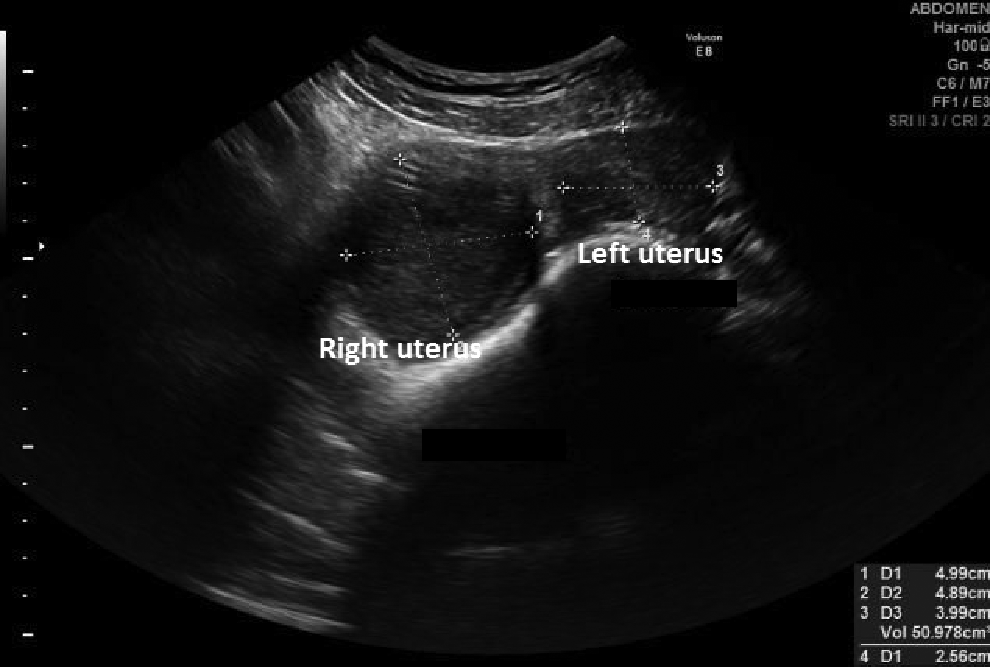
Pelvic sonography showing transverse section of left and right uteri.
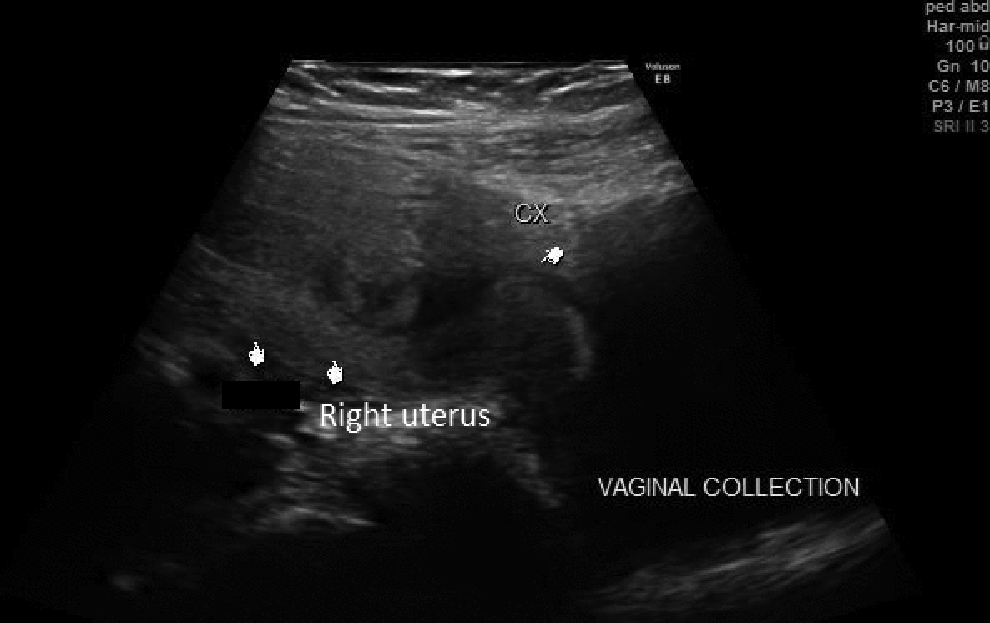
Right uterus with hematometra communicating with hematocolpos.

Intravenous pyelography film showing a functioning left kidney and absence of right kidney and ureter.
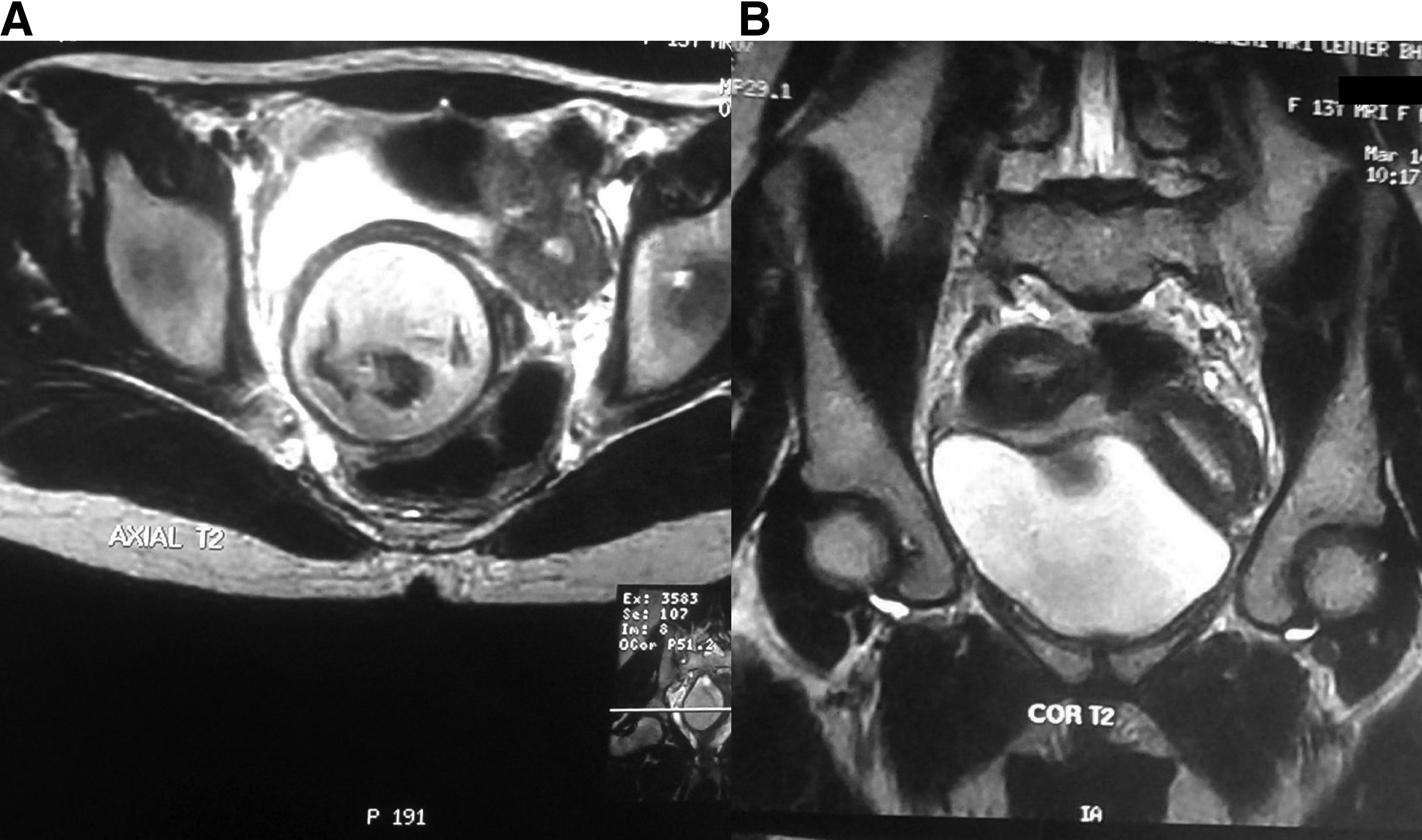
Magnetic resonance imaging of pelvis in axial
After this complete preoperative analysis, a diagnostic laparoscopy, with excision of the obstructing vaginal septum, was planned. Examination under anesthesia revealed a cystic mass in the right lateral wall of the vagina obscuring palpation of the cervix or uterus on the right side. On the left side, the normal cervix and uterus were palpable. Diagnostic laparoscopy showed two uteri with a cystic mass on the right side, which was formed as a result of hematocolpos (Fig. 5). The left uterine horn, fallopian tube, and ovary appeared to be absolutely normal. The right uterine horn and fallopian tube were distended because of hematometra and hematosalpinx, respectively (Fig. 6). Mild endometriosis was present with chocolate colored fluid in the pelvis. Diffuse endometriotic patches were present over the right uterine horn and right ovary, which were fulgurated with a bipolar energy source. A thorough peritoneal wash was performed. A cruciate incision was made at the bulging right vaginal septum, which led to drainage of ∼800 mL of dark old collected blood. The patient tolerated the procedure well and was discharged after 48 hours.

Laparoscopic image showing right and left uteri with the distended right vagina caused by hematocolpos.
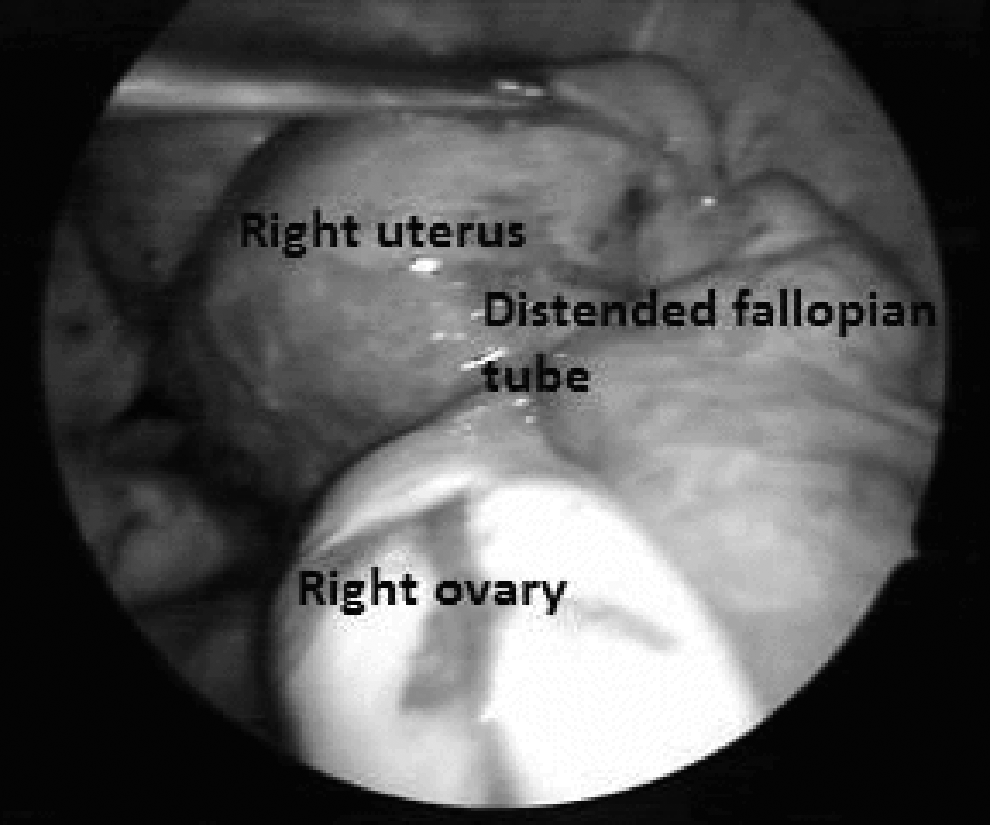
Laparoscopic image showing distended right fallopian tube and ovary with endometriotic patches on the surface.
Results
On follow-up, after 1 month, the patient had a normal menstrual flow with no complaints of dysmenorrhea. Two years after her surgery, this patient again experienced severe dysmenorrhea. Sonography testing showed a hematocolpos of ∼5 × 5 cm and minimal hematometra. Excision of the vaginal septum was performed, the hematocolpos was drained, the and edges of the excised septum were stitched with No. 1-0 vicryl. Postoperatively, sonography was performed, and no collection in the vagina or uterus was identified (Fig. 7). The patient was advised to use a vaginal stent for 1 month to prevent reocclusion of her septum. On follow-up, patient reported having normal menstruation without any complaints of dysmenorrhea.
Pelvic sonography after reexcision of the septum demarcating the two uterine cavities without any collection in uterus or vagina.
Discussion
Müllerian duct anomalies (MDAs) are congenital malformations of the female genital tract resulting from aberrant development of the Müllerian or paramesonephric ducts in the forms of agenesis, incomplete fusion, or resorption.4,5 The reproductive system develops in close proximity with the urinary system—paramesonephric and mesonephric ducts, respectively—during the early developmental stages of the embryo at ∼6–8 weeks. Anomalies in one system may be associated with abnormalities in the other system. Renal anomalies that are associated with Müllerian anomalies include renal dysplasia, duplication of the collecting system, and an ectopic ureter. 2 Renal-tract anomalies are associated with MDA in as many as 30% of cases. 6 Wolffian ducts, apart from giving rise to kidneys, also play important role in induction of fusion of Müllerian ducts. On the side where the Wolffian duct is absent, it leads to lateral displacement of the Müllerian duct such that it cannot fuse adequately with the contralateral duct, giving rise to uterine didelphus. For the current case, this article presented a rare situation wherein both of the uteri were functioning with an absence of the kidney on the obstructed side.
Herlyn–Werner syndrome (i.e., renal agenesis and an ipsilateral blind hemivagina) was initially described in 1971 by Herlyn and Werner.
7
In 1976, Wunderlich described an association of right renal aplasia with a bicornuate uterus and simple vagina in the presence of an isolated hematocervix.
8
Its estimated occurrence is 0.1%–3.8%.
9
The acronym OHVIRA [
The diagnosis of HWW syndrome is often delayed because of less understanding of Müllerian anomalies by practitioners. The usual age of presentation is the postmenarchal period, with the symptoms of dysmenorrhea and pelvic pain. However, cases of presentation of this syndrome in newborns and middle-age females have also been reported in the literature. Wu et al. reported the presentation of HWW syndrome with a bulging vulvar mass in a newborn. 11 Cox et al. reported a case of OHVIRA syndrome presenting as pyocolpos. 12
Sonography is usually the initial diagnostic modality. Three-dimensional ultrasound can help to arrive at a precise diagnosis because, sonography enables one to view the coronal plane, which, in turn, allows a precise evaluation of the relationship of the uterine fundus with the cavity. 13 However, MRI is superior to ultrasound because of MRI's better delineation of anatomical relationships, owing to MRI's multiplanar capabilities and tissue characterization, which are important for surgical planning. 12 Laparoscopy is now considered to be more popular for evaluation of female reproductive-tract anomalies; this technique can not only confirm the diagnosis with certainty but can also be helpful in fulguration of endometriosis lesions formed as a result of retrograde menstrual blood flow in obstructing MDAs.
Treatment for cases of Müllerian anomalies is individualized, depending upon the age, complaints, and reproductive needs of each patient. Treatment of patients with HWW syndrome is drainage of collected blood or mucus by resection of the obstructing vaginal septum as completely as possible, using scissors, a scalpel, conventional scalpel diathermy, or a resectoscope.14,15 Resection under laparoscopic control helps to avoid or detect an inadvertent bladder injury, as the paravesical anatomy is distorted in such cases. Hysteroscopic, vaginal septum resection under transabdominal ultrasound guidance is preferable in young females to preserve hymenal integrity. 2 In fewer cases, hemihysterectomy and excision of the vaginal septum have also been reported.16,17 In cases complicated by cervical atresia, ipsilateral hysterectomy is suggested, because resection of the septum would not relieve symptoms caused by an obstruction. 18
In the current case, a complete excision of the septum was performed and sutures were run at the edges to achieve complete hemostasis and to prevent reocclusion of the septum, as it had occurred after the initial treatment when only a cruciate incision was made in the septum to relieve the obstruction. The minimal amount of endometriosis arising as a result of obstruction of draining passage was fulgurated with bipolar diathermy. Patients with these types of endometriotic-like lesions have very good prognoses, because, as soon as the obstructions are removed and the outflow tracts become normal, these lesions usually regress, as they are not true endometriotic lesions.
Conclusions
In young females presenting with intractable dysmenorrhea, a thorough evaluation should be conducted to rule out Müllerian anomalies. A delay in diagnosis can lead to complications such as acute abdomen or long-term sequelae such as severe endometriosis, adhesion formation in the pelvis, infertility, and recurrent pregnancy losses. In females with Müllerian anomalies complete evaluation of the urinary system should be performed, as there are frequent associations of urinary-system anomalies with MDAs. In addition, evaluation of the genital tract in all female adolescents diagnosed with renal agenesis is recommended. Obstructive Müllerian anomalies have a tendency toward reocclusion after the primary surgery, so meticulous follow-up and counseling is important to ensure recognition of recurrence. In such cases of restenosis, having the patient retain a vaginal stent for some time after the repeat surgery can help prevent further occlusions.
Footnotes
Author Disclosure Statement
No competing financial conflicts exist.