
Abstract
Abstract
Introduction
C
In few rare cases, appendicitis has been found to be existing simultaneous to ectopic pregnancy, so an etiological relationship has been proposed among the two conditions. 1 We present a rare case report of simultaneous occurrence of chronic ectopic pregnancy with appendicitis and its successful laparoscopic management.
Case
A 34-year-old woman presented to us with pain in the abdomen for 2 days with one episode of vomiting and persistent nausea. There was no history of syncope. She had her period 1 month back, which remained for 2 days only with scanty flow and was accompanied by lower abdominal pain. Since then, the patient had been asymptomatic till the present episode. The patient was Para 1, with the last child birth 11 years back, normal vaginal delivery. Her previous menstrual cycles were regular, and she was not following any contraceptive methods.
On examination, the patient was having mild pallor. Her pulse rate was 82 beats per minute and blood pressure was 100/70 mm Hg. The abdomen was soft; no guarding or rigidity was observed but a minimal tenderness was noticed in the right iliac fossa. There was no palpable mass. On per vaginal examination, the uterus was anteverted, normal sized; slight tenderness on the right fornix was observed; and cervical movement tenderness was absent. All laboratory investigations were within normal limits except for the serum beta hCG value, which was 777 mIU/mL. A transvaginal ultrasound examination revealed the presence of a moderate amount of free fluid in the pelvis with internal echoes. An extra-uterine mass having features of an ectopic pregnancy abutting the posterior wall of uterus was also found in the right fallopian tube with an empty uterine cavity, and the right fallopian tube was seen to be filled with fluid, which was likely to be blood (Fig. 1). A decision for laparoscopy was taken. A 5 mm 30° telescope was used for laparoscopy through the umbilical port, which confirmed the presence of hemoperitoneum. Free blood was found in the pelvis (Fig. 2) and paracolic gutters. The right fallopian tube appeared inflamed, engorged near the ampullary region, and adherent to the right ovary with blood clots around it, suggestive of chronic ectopic pregnancy (Fig. 3). The left fallopian tube was also found to be edematous, suggestive of chronic salpingitis (Fig. 4). The tip of the inflamed appendix extending up to the right tubo-ovarian mass was noted (Fig. 5). Hemoperitoneum was drained, and bilateral salpingectomy was done. Laparoscopic appendectomy was also performed using the same ports.

Transvaginal sonography showing right tubal ectopic mass behind the uterus with right fallopian tube filled with blood.
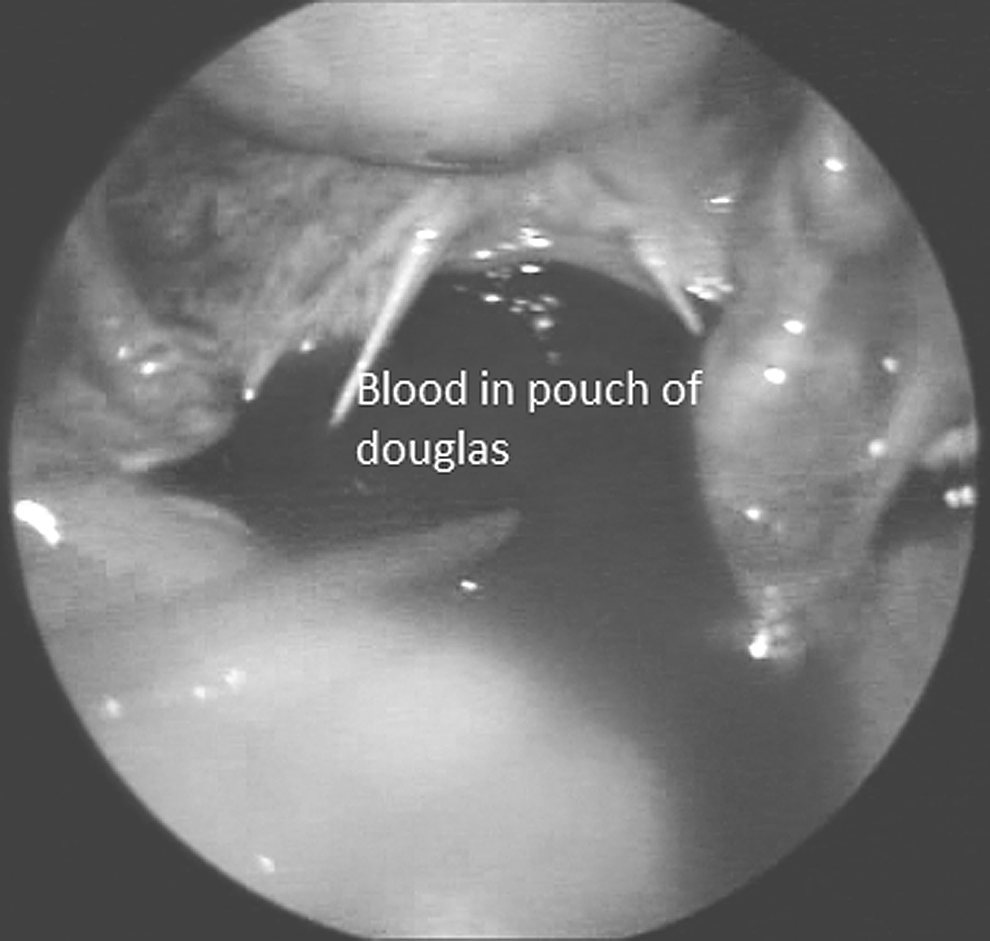
Laparoscopic image showing free blood in pelvis.

Right chronic tubal ectopic adherent with ovary showing clots on the surface.

Laparoscopic image showing edematous left fallopian tube.

Edematous appendix seen after separation from the chronic ectopic mass; tip of appendix with clots over it was adherent to the ectopic pregnancy mass.
The patient made an uneventful recovery. Histopathology examination of the specimen confirmed the presence of products of conception in the right fallopian tube along with chronic inflammation (Fig. 6). The specimen of the appendix and the left fallopian tube also confirmed the presence of inflammation (Figs. 7 and 8).
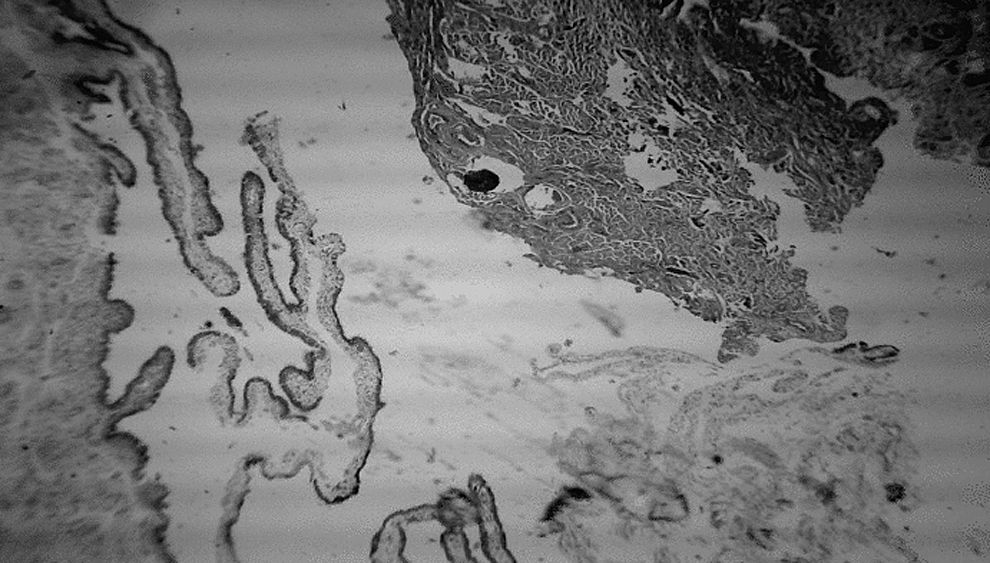
Histopathology picture of right fallopian tube with ectopic gestation inside.
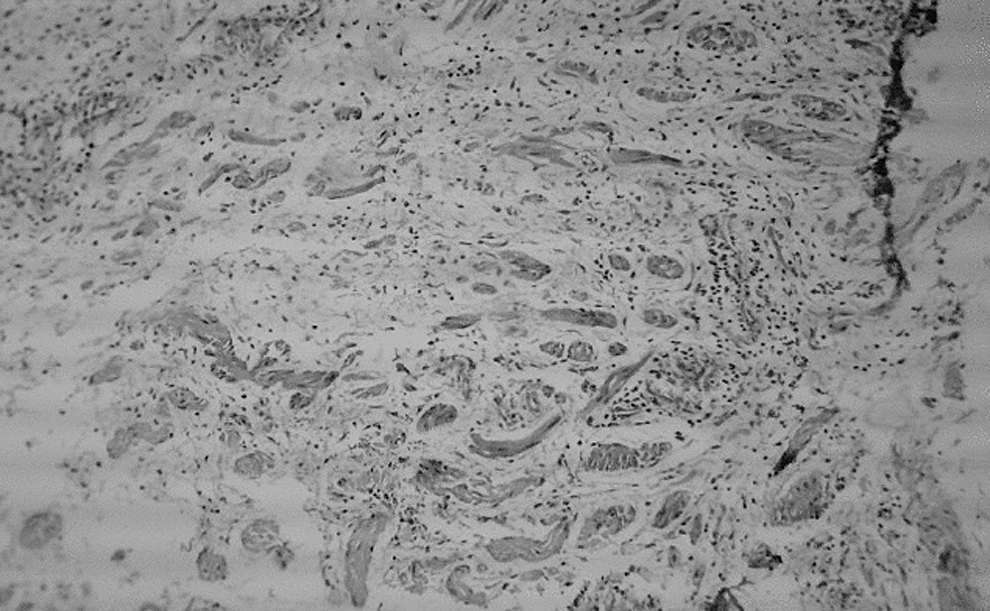
Histopathology picture of left fallopian tube showing inflammatory changes.
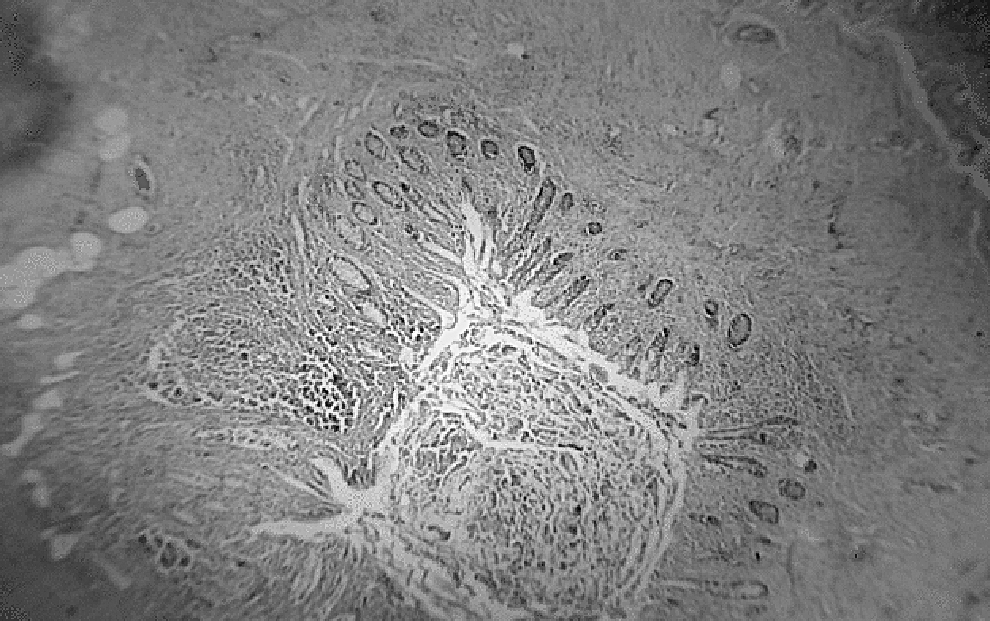
Histopathology picture of appendix showing inflammation.
Discussion
Chronic ectopic pregnancy is a conundrum as the clinical presentation can be deceiving, with absent or subtle symptoms. The frequent association of negative urine pregnancy test and poor specificity of sonographic patterns can be misleading, and the correct diagnosis is sometimes established only at surgery or even histopathologically after the surgery.
Ectopic pregnancy has been rarely reported in conjunction with appendicitis. The possible underlying etiologic relationship between ectopic pregnancy and appendicitis has been postulated. It is unknown whether appendicitis is coincidently associated with ectopic pregnancy or is a possible risk factor for subsequent development of ectopic pregnancy. Some authors have stated that appendicitis may induce varying degrees of inflammation in the fallopian tube that predisposes to subsequent development of ectopic pregnancy,1–3 while others have asserted that ectopic pregnancy may induce inflammatory changes in vicinity, leading to appendicitis.1,4 It has been seen that the cases of concurrent ectopic pregnancy and appendicitis have a predilection for right tubal ectopic pregnancy (75%) versus left tubal ectopic pregnancy (16%). 1
In our case, the patient presented with very subtle signs and symptoms of ectopic pregnancy and appendicitis was an incidental finding on laparoscopy. Laparoscopy has both a diagnostic and a therapeutic role in a hemodynamically stable patient. A 5 mm telescope is good enough for diagnostic purposes to confirm hemoperitoneum or locate the ectopic pregnancy.5–9 The patient had her family completed with no desire of future pregnancy, so the contralateral fallopian tube was also removed considering the fact that it appeared edematous and it could have acted as a nidus for a recurrent ectopic pregnancy in future. The histopathogical report confirmed the presence of inflammation in both fallopian tubes and appendix too, confirming the diagnosis. From these findings, we can infer that the basic pathology could be longstanding pelvic inflammatory disease that led to ectopic pregnancy as well to the appendicitis.
Conclusion
Chronic ectopic pregnancy is a challenge for obstetricians, especially when associated with the negative urine pregnancy test. It can present with just menstrual irregularity and very mild abdominal symptoms. One has to be very careful while doing sonography to see the minimal amount of hemoperitoneum and mild adhesions around the tube and ovary. Although the combination of ectopic pregnancy and appendicitis is quite rare, it is advisable to visualize the appendix and the other fallopian tube for the possibility of coexisting inflammation during laparoscopy in patients of ectopic pregnancy, especially if it is on the right side due to a possible inter-etiological relationship. By following this simple dictum, we can save the patient from the possibility of ongoing morbidity and future surgeries involving the appendix or the other fallopian tube. But it should be kept in mind that whenever the appendix and/or the contralateral fallopian tube are removed on the basis of laparoscopic appearance, it is necessary to confirm the diagnosis by histopathology. The postoperative morbidity can be reduced dramatically by laparoscopic management of these cases.
Footnotes
Disclosure Statement
No competing financial interests exist.