
Abstract
Abstract
Introduction
P
Risk factors specific to the minimally invasive surgery population include pneumoperitoneum that is necessary for pelvic procedures. 5 Other previously identified risks of PONV include previous history of PONV, nonsmoking status, duration of surgery, and postoperative opioid use. 6 Patients undergoing robotic-assisted gynecologic procedures may be exposed to additional risks, including prolonged operative time and steeper Trendelenburg position than traditional laparoscopy.7,8
Numerous trials have been undertaken to evaluate various methods to manage PONV. More than 1000 identified studies focus on one of the following three approaches: preoperative modalities, including counseling or administration of anti-emetogenic agents, intraoperative avoidance of emetogenic inhaled agents with utilization of intraoperative agents to reduce postoperative emesis, or postoperative agents that treat PONV. More recently, numerous investigators have focused on multi-modality suppression of PONV. It is clear at this time that multi-modality therapy combined with the benefits of improved gastrointestinal function and the latest minimally invasive surgical modalities may maximize the prevention of PONV, above all previously attempted multi-modality approaches.
Scopolamine is an anticholinergic agent that exerts central CNS effects to suppress nausea and vomiting. It is indicated for prevention of motion sickness and PONV and is applied as a transdermal 1.5 mg patch. However, review of the literature shows that research on the efficacy of transdermal scopolamine in the gynecologic laparoscopic population is sparse. 3 No studies to date have been conducted while investigating the incidence and severity of PONV after robotic-assisted gynecologic procedures, or the use of transdermal scopolamine in this population. Therefore, our main objective was to evaluate the efficacy of scopolamine for treatment of PONV as an integral measured part of a multi-modality regimen in women undergoing robotic-assisted gynecologic surgical procedures.
Materials and Methods
The patient population for this study was drawn from women undergoing robotic-assisted gynecologic surgical procedures performed by a single gynecologic oncologist from November 2012 to April 2013. Surgeries were performed at two academic-affiliated community hospitals, served by a single anesthesia group and a single institutional review board (IRB). The study was fully reviewed and approved by the IRB.
All patients scheduled to undergo robotic-assisted gynecologic surgery were eligible to participate. They were excluded for allergy to scopolamine or belladonna, history of narrow-angle glaucoma or difficult urination, or unwillingness to complete study procedures.
After informed consent, patients were randomized at the time of surgery to two groups. The experimental group received a 1.5 mg transdermal scopolamine patch applied in the preoperative holding area, which was then covered by an adhesive bandage. The control group received the adhesive bandage only. Randomization was achieved by sealed, consecutively numbered opaque envelopes with enrollment to either group determined by a computer-generated random number sequence. At the time of enrollment, the independent anesthesia staff assigned to the surgical case opened the envelope and placed either the patient's scopolamine patch or the placebo. In this way, we preserved a double-blinded, placebo-controlled study design with the surgeon, surgical team, and patient, all of whom were unaware of the study arm. Also contained in the envelope was a standardized anesthesia protocol with a recommended regimen for premedication, intraoperative and postoperative medications (Fig. 1).
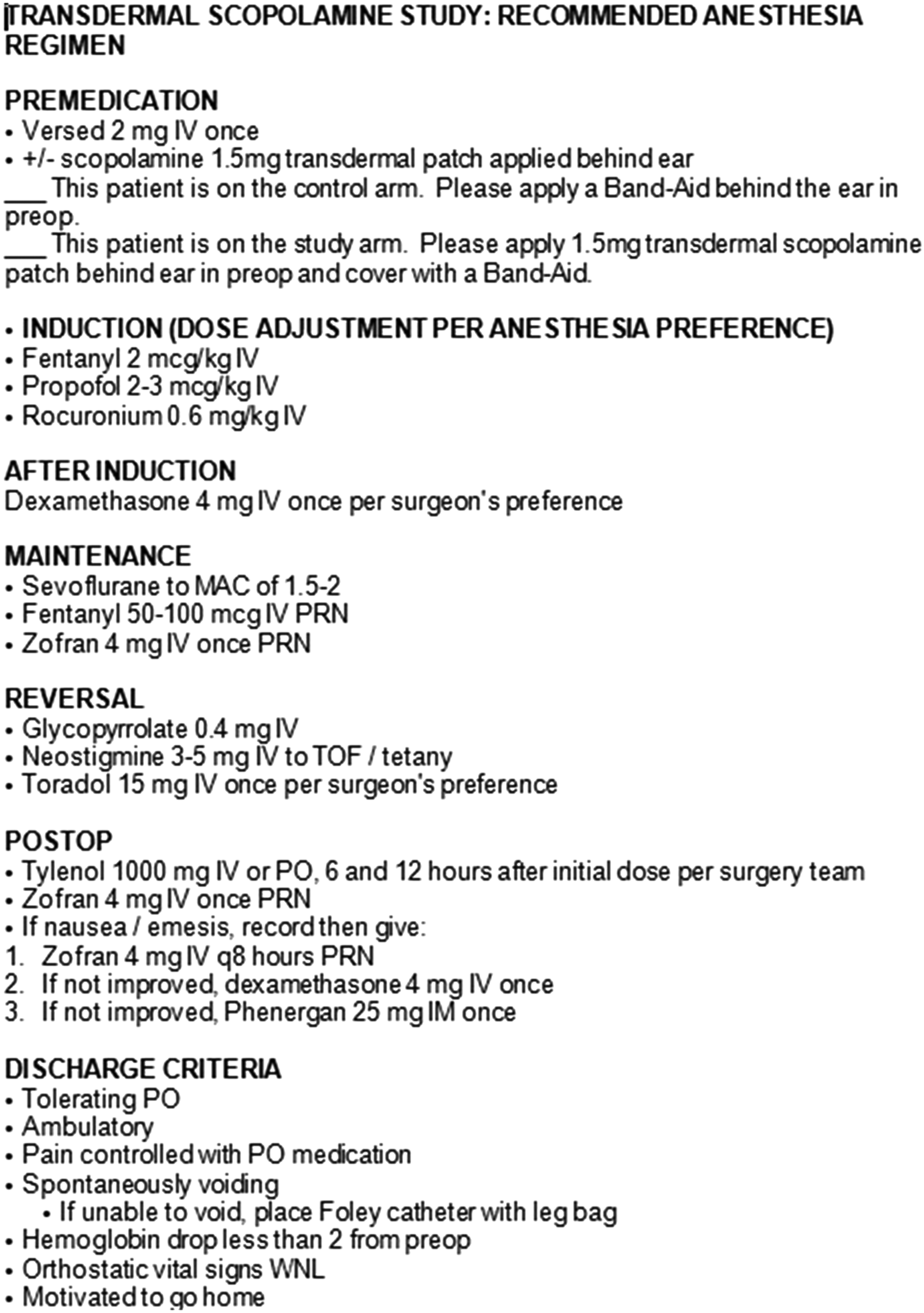
Anesthesia regimen.
Patients were given a series of questionnaires to complete in time intervals of 6, 12, 24, 48, and 72 hours postoperatively (Fig. 2). Each group of questions asked the study subject to quantify their episodes of nausea and vomiting in each time interval. The patients then rated the severity of their nausea and vomiting on a visual analogue scale (VAS). A VAS has been successfully used in previous studies of PONV in the gynecologic laparoscopic setting.3,9–11 Each questionnaire also asked the patient to rate the impact of PONV on their well-being as well as on their overall well-being via VAS. Patients were asked whether they experienced any side effects common to the study intervention: dry mouth, visual disturbances, tiredness, and skin irritation. Finally, patients were asked how many times they required antiemetic medication in each time interval. Patients were instructed to remove their scopolamine or placebo patch 24 hours postoperatively, and they returned their study questionnaires at their routine postoperative visit 1 week after their procedure. Patients who did not return their questionnaires were contacted by phone and asked to either return their study forms or transmit them by fax or email.

Sample questionnaire.
We defined our primary outcome as severity of PONV as scored by VAS. Secondary outcomes were antiemetic use, time to discharge, effect on patient well-being of PONV, and patient overall well-being as scored by VAS at defined time intervals. A priori power analysis with a power of 80% and p-value of 0.05 led to a sample size calculation of a total study population of 40 patients divided between the two arms. Data analysis was performed with SPSS (SPSS Statistics Windows Version 21, Chicago IL). The two groups were assumed independent, and Levene's test was run to analyze equality of variance. If equal variance was assumed, an independent sample t-test was run; otherwise a ranked sum test for analysis of variance was run. p-Values were set at 0.05.
Results
Forty-seven patients were enrolled in the study (Fig. 3). Of these, several did not return their study questionnaires: four in the experimental group and four control patients. One of these control patients did not complete her questionnaire, because her patch fell off before 24 hours, postoperatively. Four other patients (one control, two experimental) did not complete the entire questionnaire. Three patients in the control arm were administered transdermal scopolamine by their anesthesia team; these data were analyzed with the experimental subjects. One patient who underwent a planned laparotomy was enrolled to the control arm. None of the patients undergoing robotic procedures experienced any operative complications or conversions to open procedure.

CONSORT diagram.
The study groups demonstrated similar demographic statistics (Table 1) and similar estimated blood losses and rates of administration of intraoperative prophylactic dexamethasone and ondansetron (Table 2).
PONV, postoperative nausea and vomiting.
There was no significant difference in the primary outcome of number and severity of nausea or vomiting via VAS at any of the study time points, and no difference when patients were asked to rate the impact on their well-being by PONV and their overall well-being via VAS (Table 3).
VAS, visual analogue scale.
There was no significant difference in length of hospital stay or modified length of stay (Table 4). Modified length of stay was calculated by excluding all patients with a documented nonmedical reason for staying overnight on postoperative day zero (e.g., patient desire, or late operating room start time, N=9 experimental, N=4 control). There was a statistically significant decrease in the number of rescue antiemetics administered in the first 6 hours postoperatively when reviewed directly from the medication administration record (MAR); however, there was no difference in number of antiemetic doses used as reported by the patients. There was no other significant difference at any other time point in number of antiemetic doses used as reported by the patients, and no difference in overall number of antiemetics used (Table 5).
MAR, medication administration record.
There were no significant differences in rates of dry mouth, vision changes, tiredness, or skin irritation at patch site between the two groups other than at 24 hours postoperatively, when the control group reported a statistically significant higher rate of dry mouth (Table 6).
Discussion
We did not show a statistically significant benefit to the administration of preoperative scopolamine for the prevention of PONV in patients undergoing robotic-assisted gynecologic surgical procedures. Although we showed a benefit to the number of antiemetic doses required in the immediate postoperative period in patients who received the scopolamine patch, there was no overall reduction in incidence or severity of nausea and vomiting, and no overall benefit to number of antiemetic doses required.
The strengths of our study included its randomized, double-blinded, placebo-controlled design, and the use of a standardized anesthesia protocol for all subjects. It is also the first to examine PONV in this specific robotic population. However, we did not have adequate power to assess our primary outcomes largely due to patient noncompliance with completing and returning questionnaires, as well as the underestimation of PONV in this robotic population. We also had a smaller control group than anticipated due to three subjects being administered the experimental intervention by the anesthesia team.
Our results contrast with those of previous similar studies, 3 which demonstrated ∼40% reductions in the incidence of nausea and vomiting in patients randomized to scopolamine. One reason for this may be a lack of sufficient power. We observed an overall rate of PONV of less than 40%, versus the previously reported rates of 40%–80%. 5 A larger study would have been required to observe an effect given that the incidence of our primary measure was lower than expected. It may be that prophylactic intraoperative dexamethasone and ondansetron, which the majority of our subjects received per standard protocol, render treatment with transdermal scopolamine irrelevant. There may also be some protective factor in the innate difference between robotic surgery and traditional laparoscopy.
We observed that scopolamine was well tolerated by our patient population, with no significantly different rates of known side effects from placebo. We were unable to demonstrate a benefit to patient well-being in the scopolamine population, although this outcome measure is difficult to quantify. 11 Currently, no satisfactory evaluation tool such as the VAS, previously and successfully used to measure nausea and vomiting, is used to measure the outcome of patient well-being. This may be why we failed to detect a difference in this outcome. We also did not show a benefit to time of discharge in the scopolamine group. The time-to-discharge measure may have been influenced by many confounders other than simply nausea.
In conclusion, this is the first study to evaluate the effect of scopolamine in a double-blinded, randomized fashion using a standardized anesthesia protocol, to prevent PONV in a gynecologic population undergoing robotic surgery. Although we cannot recommend the use of transdermal scopolamine as an adjunct to prevent PONV in patients undergoing robotic-assisted gynecologic procedures based solely on the outcomes of this study, the drug in question is of low cost and is well tolerated. Further studies are needed in this population to identify a benefit beyond a decrease in the number of rescue antiemetics administered in the first 6 hours postoperatively when reviewed directly from the (MAR). There may also be a lower rate of PONV in the robotic population when compared with a traditional laparoscopic population, and this warrants further investigation with a larger trial, as our rate of PONV in this robotic population utilizing a multimodality regimen was less than 40% with or without the use of scopolamine.
Footnotes
Disclosure Statement
No competing financial interests exist.