
Abstract
Abstract
Introduction
E
Case
A 36-year-old woman, gravida 4, para 2, curetage 1 was admitted to the emergency department of the Kanuni Sultan Suleyman Training and Research Hospital, in Istanbul, Turkey. She had severe abdominal pain. She had two previous vaginal deliveries, both of which were unremarkable. She did not have any risk factors, such as a previous history of ectopic pregnancy or tubal surgery, or the presence of an intrauterine contraceptive device (IUD). She reported that she had been taking oral contraceptive pills and that the date of her last menstrual period was unclear to her because she had been experiencing abnormal bleeding between her menses. She had been having intermittent pain in her abdomino-pelvic region for 2 months and this pain had gotten worse in the last 3 days prior to her arrival at the hospital.
On admission, it was noted that this patient had mild vaginal bleeding and nausea. Her vitals were as follows: blood pressure, 90/60 mmHg; pulse rate, 120 beats per minute; respiratory rate, 16 breaths per minute; and body temperature, 37.6°C. A bimanual examination showed that her uterus was slightly enlarged and softened. Cervical motions were painful for her. A physical examination revealed abdominal tenderness. According to her signs, she was diagnosed as having an acute abdomen.
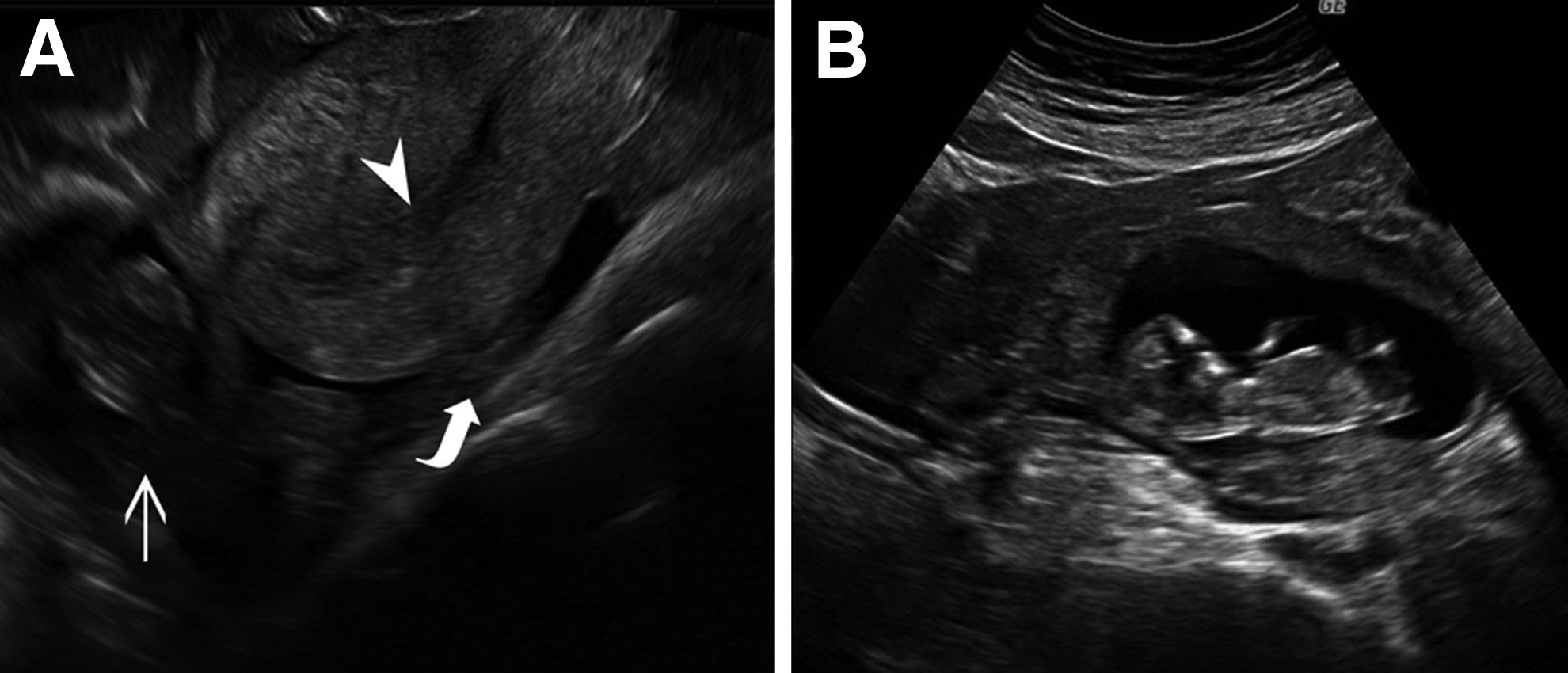
Transabdominal sonography revealed a gestational sac with a live fetus at a crown–rump length of 65 mm, which was concordant with 12 gestational weeks, located at the superior surface of the uterine fundus. The pregnancy mass measured 8×5 cm on the widest diameter (Fig. 1). Free fluid was observed in the cul-de-sac, and in the paracolic and perihepatic areas. Endometrial thickness was measured 5 mm. Laboratory results were as follows: hemoglobin level, 8.3 g/dL; hematocrit, 24.8%; platelet count, 271,000 mm3; renal and liver function, within normal ranges; and serum beta–human chorionic gonadotropin (β-hCG) level, 28,307 IU/L.
After these examinations, a decision for an operation was made with the prediagnosis of an abdominal pregnancy, or a ruptured intrauterine or horn pregnancy. First, a diagnostic laparoscopy was performed. On examination, it was noted that there was a massive hemoperitoneum; thus, because of this patient's hemodynamic instability and massive abdominal bleeding, and emergency midline laparotomy was performed. On exploration, ∼1 L of hemoperitonium was seen, and, in the right Fallopian tube, an unruptured ectopic mass of 75×45 mm was noted, with torsion of this Fallopian tube and some bleeding from the fimbrial os. The ovary was normal in appearance (Fig. 2A).

Two perioperative views of the patient's ectopic pregnancy.
According to these findings, a right salpingectomy was performed. Intraoperatively, 2 units of packed red blood cells were administered. When the salpingectomy material that had been excised was examined, the crown–rump length of the fetus measured 72 mm, which was compatible with 13 weeks and 3 days' gestational age (Fig. 2B).
Results
This patient's postoperative recovery was uneventful, and she was discharged on the 3rd postoperative day.
Discussion
Ectopic pregnancy is one of the significant causes of morbidity and mortality in the first trimester of pregnancy. Previous ectopic pregnancy, tubal pathology and surgery, tubal ligation, in utero dietylstilbestrol exposure, and current usage of any intrauterine device are underlying risk factors. 2 Abdominal pain, amenorrhea, and vaginal bleeding are the classic symptoms of an ectopic pregnancy. 3
Any reproductive-age woman who is experiencing abnormal vaginal bleeding is a candidate for an ectopic pregnancy. The diagnosis of ectopic pregnancy is usually obvious for women with the classic symptoms of a ruptured ectopic pregnancy. Today, the concept of a “discriminatory zone” is being used: An intrauterine sac should be visible when a patient's β-hCG level is between 1500 and 2500 mIU/mL. Otherwise, further investigation is needed for exclusion of an ectopic pregnancy.
Classically, the earliest and the latest ruptures are expected to be in isthmic and interstitial (cornual) pregnancies, respectively, among tubal ectopic pregnancies. In a study by Frates et al., 231 patients were evaluated retrospectively for a correlation between tubal ruptures and sonographic findings; the mean and maximum lengths for ectopic pregnancy masses with fetal cardiac activity are 2.45 cm and 6 cm, respectively. 4 Sindos et al. pointed out the risk factors for ectopic pregnancies in their study wherein these researchers observed 223 subjects retrospectively. 5 These researchers indicated that gestational week has a borderline correlation with the risk of rupture among all the factors. The mean and maximum gestational ages were shown to be 53.9 and 71 days, respectively. Gestational age was calculated with the date of last menstrual period when the crown–rump length measurements were not included. In another study the mean gestational age for ruptured ectopic pregnancies was 7.2±2.2 weeks and for the unruptured pregnancies the gestational age was 6.9±1.9 weeks. 6
Isthmic ectopic pregnancies are likely to rupture earlier than ampullary ectopic pregnancies. It has been reported in many studies that the time of ruptures in ampullary pregnancies are ∼7– 8 weeks of gestation.5,6 Although it has been reported in past literature that ampullary pregnancies were rarely able to proceed until 10th week, currently, they may even reach 12 or 13 weeks.
The current case is one of largest pregnancies in this category ever reported. Isolated torsion of the Fallopian tube without ovarian torsion in this case can be explained by the bulking effect of the ectopic pregnancy. As in this current case, the first differential diagnosis must exclude any abdominal pregnancy besides a horn pregnancy or a huge ectopic pregnancy, as was considered. In the literature, isolated torsions of the Fallopian tubes without ovarian torsions are mostly detected in cases, such as hydatids of morgagni, hydrosalphinxes, and hematosalphinxes, which are known to produce a bulking effect in the Fallopian tubes. 7 In the pediatric age group, dysfunctional motility in excessively long and tortuous Fallopian tubes are suspected to be caused by isolated torsion of the Fallopian tubes. 8
It is rare for ampullary ectopic pregnancies to progress to the 13th week of gestation. However, rare advanced ectopic pregnancies have been presented in the literature. Kocak et al. reported a 30-week tubal ampullary pregnancy 8 while Grullon et al. reported an asymptomatic ectopic pregnancy that reached the 20th week of gestation. 9 This current case is original and rare in that the pregnancy had advanced to 12–13 weeks with torsion and yet was without rupture. Torsional involvement in this case may have been caused by the excessive growing of the mass, and this might have contributed to worsening of the pain in the patient's groin. The differential diagnosis of abdominal pregnancies can be supported by magnetic resonance imaging, but operational diagnosis may be considered, as urgent laparotomy is crucial in some cases.
Conclusions
Localization of any pregnancy should be determined cautiously in order not to miss rare ectopic pregnancies and to decrease maternal morbidity and mortality.
Footnotes
Disclosure Statement
The authors declare that there is no conflict of interests regarding the publication of this article.